
White Blood Cells (Leukocytes)
By the conclusion of this exhaustive master guide, you will be deeply conversant with:
- The detailed morphology, abundance, and highly specific physiological functions of the five major classes of Leukocytes.
- The exact, step-by-step hematological pathways of Leukopoiesis, including progenitor lineage and regulatory cytokines.
- Comprehensive profiles of Quantitative, Qualitative, and Malignant WBC Disorders, complete with clinical presentations and diagnostic markers.
- The advanced clinical interpretation of the Differential WBC Count and absolute cell metrics in diagnostics.
I. Introduction to White Blood Cells (Leukocytes)
White blood cells (WBCs), also known as leukocytes, form the mobile, intelligent defensive army of the human body. Circulating continuously through the cardiovascular and lymphatic systems, they are fundamentally distinct from red blood cells (erythrocytes). Unlike RBCs, mature leukocytes are complete, true cells—they possess a distinct nucleus, active mitochondria, a Golgi apparatus, and the ability to manufacture proteins.
While confined to the bloodstream for rapid transport, their true battleground lies in the tissue spaces. Leukocytes possess a unique capability called diapedesis (or extravasation)—the ability to physically squeeze through the intact endothelial walls of capillaries to hunt pathogens directly in the interstitial fluid.
A normal adult has a WBC count ranging from 4,500 to 11,000 cells per microliter (μL) of blood. Based on the presence or absence of visible, chemical-filled vesicles (granules) when stained with standard Romanowsky stains (like Wright's or Giemsa), leukocytes are distinctly classified into two major categories: Granulocytes and Agranulocytes.
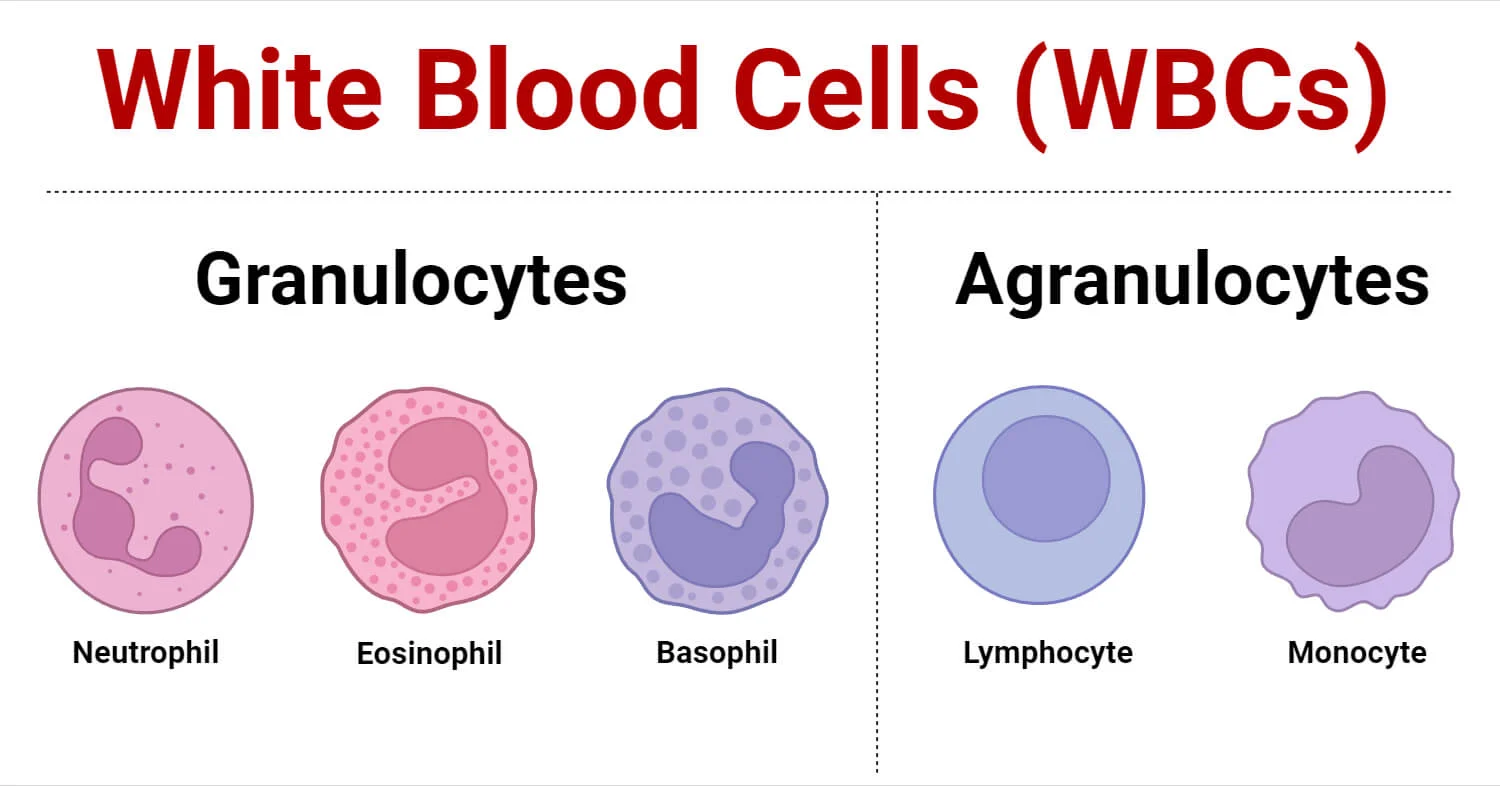
II. Category 1: The Granulocytes
Granulocytes are characterized by lobed, oddly shaped nuclei and cytoplasm packed with highly visible, reactive granules containing destructive enzymes, inflammatory mediators, and antimicrobial peptides. Because of their multi-lobed nuclei, they are often referred to clinically as Polymorphonuclear Leukocytes (PMNs), though this term is most strictly applied to neutrophils.
The First Responders (50-70% of total WBCs)
Morphology:
- Nucleus: Highly polymorphic, consisting of 2 to 5 distinct lobes connected by incredibly thin strands of chromatin. As a neutrophil ages, it gains more lobes. (Clinical Note: In females, a drumstick-shaped appendage called a Barr body—the inactivated X chromosome—is sometimes visible on one lobe).
- Cytoplasm: Packed with fine, pale lilac or pinkish-tan granules that stain neutrally (hence the name "neutrophil").
- Size: 10-14 μm in diameter.
Primary Functions & Deep Mechanisms:
- Rapid Phagocytosis: They are the acute phase responders to bacterial and fungal infections. They follow chemical trails (chemotaxis) to the site of infection.
- The Respiratory Burst: Once a bacterium is engulfed into a phagosome, the neutrophil unleashes a lethal "respiratory burst" (oxidative burst), creating massive amounts of superoxide anions, hydrogen peroxide, and bleach (hypochlorous acid via the enzyme Myeloperoxidase) to instantly vaporize the pathogen.
- Pus Formation: Neutrophils are essentially "kamikaze" cells. They fight fiercely, live for only 1 to 2 days in the tissues, and die. The accumulation of dead neutrophils, digested tissue, and dead bacteria forms the clinical exudate known as pus.
The Parasite Hunters (1-4% of total WBCs)
Morphology:
- Nucleus: Characteristically bi-lobed, frequently resembling an old-fashioned telephone receiver, a pair of eyeglasses, or headphones.
- Cytoplasm: Stuffed with large, coarse, uniform granules that stain a brilliant, fiery red-orange with eosin (an acidic dye). Under electron microscopy, these granules contain a distinct crystalline core.
- Size: 12-17 μm.
Primary Functions & Deep Mechanisms:
- Anti-Parasitic Warfare: Multicellular parasites (like tapeworms, hookworms, and flukes) are physically too massive for a single WBC to phagocytize. Eosinophils surround the worm and exocytose their toxic granules (specifically Major Basic Protein - MBP), which acts like acid, dissolving the parasite's tough outer cuticle.
- Allergy Modulation: They accumulate heavily in tissues during asthma attacks and severe hay fever. Interestingly, they play a dual role: they both promote tissue remodeling in asthma and release enzymes like histaminase to safely break down excess histamine, preventing allergic reactions from becoming uncontrollably fatal.
The Inflammatory Initiators (0.5-1% of total WBCs - The Rarest)
Morphology:
- Nucleus: Bi-lobed or S-shaped, but it is notoriously difficult to see because it is almost entirely obscured by the massive cytoplasmic granules.
- Cytoplasm: Contains immense, coarse, dark blue-purple granules (which have an affinity for basic dyes, hence "basophil").
- Size: 10-14 μm.
Primary Functions & Deep Mechanisms:
- Anaphylaxis and Allergy: The granules are essentially bombs filled with Histamine (a powerful vasodilator that causes vessels to leak fluid, producing redness and swelling) and Heparin (a potent anticoagulant preventing blood clotting in the infected area).
- IgE Cross-Linking: Basophils carry specific receptors for IgE antibodies. When an allergen (like peanut protein or bee venom) binds to these IgE antibodies on the basophil surface, the cell violently degranulates, triggering anaphylactic shock.
- Note: While functionally almost identical to tissue-dwelling Mast Cells, Basophils are distinctly different entities originating from different precursor pathways in the bone marrow.
III. Category 2: The Agranulocytes (Mononuclear Leukocytes)
Agranulocytes lack the dense, visually prominent specific granules found in granulocytes (though they do contain fine, non-specific lysosomes). Their nuclei are typically massive, rounded, un-lobed, or kidney-shaped.
1. Lymphocytes (20-40% of total WBCs)
Lymphocytes are the supreme generals of the Adaptive (Specific) Immune System. They do not just blindly attack anything foreign; they memorize specific pathogens and launch highly targeted strikes.
- Morphology: The nucleus is large, densely stained (dark purple), and perfectly round, taking up almost the entire volume of the cell. The cytoplasm is reduced to a tiny, pale-blue crescent rim around the nucleus. They range from small (7-9 μm) to large reactive forms.
- T Lymphocytes (T Cells): Responsible for Cell-Mediated Immunity.
- Cytotoxic T Cells (CD8+): The assassins. They seek out and inject lethal toxins (perforins and granzymes) directly into host cells that have been infected by viruses, or cells that have turned cancerous.
- Helper T Cells (CD4+): The commanders. They secrete cytokine signals that direct the entire immune response, telling macrophages to eat faster and B cells to produce antibodies. (These are the specific cells destroyed by the HIV virus).
- B Lymphocytes (B Cells): Responsible for Humoral (Antibody-Mediated) Immunity. Upon encountering a specific pathogen, B cells transform into massive factory cells called Plasma Cells. Plasma cells pump out millions of Y-shaped target-seeking missiles known as Antibodies (IgG, IgA, IgM, IgE) into the blood. Some B cells remain behind for decades as "Memory B Cells," granting lifelong immunity to diseases like measles.
- Natural Killer (NK) Cells: A unique subset that acts as a bridge to innate immunity. They patrol the body constantly and instantly destroy tumor cells or virus-infected cells without needing prior sensitization or memory.
2. Monocytes (2-8% of total WBCs)
Monocytes are the largest cells in the peripheral blood. They are the highly capable precursor cells of the tissue macrophage system.
- Morphology: Massive cells (14-20 μm) with a distinctive, indented, kidney-bean or horseshoe-shaped nucleus. The cytoplasm is abundant and has a dusty, pale gray-blue "ground-glass" appearance, often containing visible vacuoles (empty bubbles used for eating debris).
- The "Big Eaters" Transformation: Monocytes only circulate in the blood for 1 to 3 days. They then permanently exit the bloodstream, enter the tissues, and undergo a massive physical transformation into Macrophages. Based on where they settle, they get special names:
- Kupffer cells: In the liver.
- Microglia: In the central nervous system.
- Alveolar macrophages: In the lungs.
- Osteoclasts: In the bone.
- Antigen Presentation: After a macrophage devours a bacterium, it doesn't just destroy it. It acts as an Antigen-Presenting Cell (APC). It takes a piece of the dead bacterium, places it on a receptor (MHC Class II) on its own surface, and physically travels to a lymph node to "show" it to T-Helper cells, effectively sounding the alarm to start a specific immune war.
| WBC Type | Cytoplasm / Granules | Nucleus Morphology | Normal Abundance | Primary Clinical Function |
|---|---|---|---|---|
| Neutrophil | Fine, pale lilac, neutral. | 2-5 lobes, polymorphous. | 50-70% | Phagocytosis of bacteria/fungi; forming pus (acute first responders). |
| Lymphocyte | None/scant pale blue rim. | Large, round, dense, fills cell. | 20-40% | Specific adaptive immunity (T-cell assassins, B-cell antibodies), viral defense. |
| Monocyte | Dust-like, gray-blue, vacuolated. | Kidney-bean or horse-shoe shaped. | 2-8% | Transforms into Macrophages; heavy phagocytosis, antigen presentation. |
| Eosinophil | Large, brilliant red-orange. | Bi-lobed (headphone shape). | 1-4% | Destroys multicellular parasites (helminths); modulates severe allergies. |
| Basophil | Massive, dark blue-purple. | Bi-lobed, often obscured by granules. | 0.5-1% | Initiates severe allergic reactions/anaphylaxis (releases histamine/heparin). |
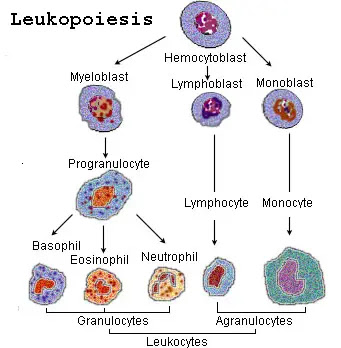
IV. The Process of Leukopoiesis (WBC Production)
Leukopoiesis is the highly orchestrated, continuous process of white blood cell production. It occurs primarily in the highly cellular red bone marrow (found heavily in the pelvis, sternum, ribs, and vertebrae in adults). Unlike erythropoiesis (red blood cell production), which is driven mostly by a single hormone (erythropoietin from the kidneys), leukopoiesis is governed by an incredibly complex chemical network of growth factors known as Colony-Stimulating Factors (CSFs) and Interleukins (ILs).
1. The Master Cell: Hematopoietic Stem Cells (HSCs)
Every single blood cell in your body begins as an identical, pluripotent Hematopoietic Stem Cell (HSC) in the bone marrow. These HSCs possess the ultimate ability to self-renew and to differentiate into two mutually exclusive progenitor pathways:
- The Common Myeloid Progenitor (CMP): The "factory" that produces the raw, non-specific blood cells: Granulocytes, Monocytes, Red Blood Cells, and Platelets (Megakaryocytes).
- The Common Lymphoid Progenitor (CLP): The specialized "factory" that strictly produces specific immune cells: T cells, B cells, and Natural Killer (NK) cells.
The Stages of Myelopoiesis (Creating Granulocytes)
The journey from a stem cell to a fully armed, multi-lobed Neutrophil is a 14-day process involving drastic morphological changes. Pathologists study these exact stages in bone marrow biopsies to diagnose leukemias.
- Myeloblast: The very first morphologically recognizable precursor. It is a massive cell with a huge nucleus, prominent nucleoli, and purely blue (basophilic) cytoplasm with absolutely no granules. (Finding Myeloblasts in peripheral circulating blood is severely abnormal and is the defining diagnostic hallmark of Acute Myeloid Leukemia - AML).
- Promyelocyte: The cell grows even larger. Crucially, the cell begins manufacturing primary (azurophilic) granules. These are dark purple, lethal lysosomes.
- Myelocyte: A critical turning point. The cell begins synthesizing specific (secondary) granules. This is the moment the cell officially commits to becoming either a neutrophil, eosinophil, or basophil. The nucleus begins to flatten. This is the last stage capable of cellular division (mitosis).
- Metamyelocyte: The nucleus becomes deeply indented, taking on a distinct kidney-bean shape. The cell stops dividing and focuses purely on maturation.
- Band Cell (Stab Cell): The nucleus becomes elongated, thin, and curved like a "C" or a horseshoe, but it has not yet segmented into distinct lobes. (Clinical goldmine: A high number of Band Cells released into the blood is called a "Left Shift," indicating the bone marrow is frantically pumping out immature soldiers to fight a massive bacterial infection).
- Mature Segmented Granulocyte: The nucleus completely pinches into distinct, thin-threaded lobes. The fully mature cell is released into the bloodstream.
2. Lymphopoiesis (Creating Lymphocytes)
The Common Lymphoid Progenitor (CLP) differentiates into a Lymphoblast, then a Prolymphocyte, and finally a mature Lymphocyte. However, their maturation locations are highly unique:
- B Lymphocytes: Born in the Bone marrow, and they stay in the Bone marrow to fully mature and learn how to make antibodies before migrating to lymph nodes.
- T Lymphocytes: Born in the bone marrow, but they immediately migrate to the Thymus gland (in the chest) to undergo a rigorous, brutal maturation and selection process. If a T-cell accidentally reacts to the body's own tissue, the Thymus forces it to commit apoptosis (cell suicide) to prevent autoimmune diseases.
3. Chemical Regulation of Leukopoiesis
The bone marrow relies on cytokine signals to know exactly what type of WBC the body needs at any given moment.
- GM-CSF (Granulocyte-Macrophage CSF): A broad-spectrum stimulator forcing myeloid progenitors to aggressively produce both granulocytes and monocytes.
- G-CSF (Granulocyte CSF): A highly specific hormone that commands the marrow to produce almost exclusively Neutrophils.
Clinical Application: Pharmacologists synthesize this hormone as a drug called Filgrastim (Neupogen). It is injected into cancer patients undergoing heavy chemotherapy to forcefully rescue them from deadly neutropenia (total loss of neutrophils). - M-CSF (Macrophage CSF): Promotes the differentiation of monocytes into tissue-destroying macrophages.
- Interleukin-3 (IL-3): A multilineage master switch; stimulates early stem cell growth across the board.
- Interleukin-5 (IL-5): The definitive, crucial cytokine required for the growth, differentiation, and explosive release of Eosinophils (levels spike heavily during parasitic worm infections).
- Interleukin-7 (IL-7): The master regulator essential for the survival and development of B and T lymphocytes.
V. Common Disorders Associated with White Blood Cells
Disorders involving white blood cells are highly diverse, ranging from simple numerical responses to severe infections, to devastating genetic functional defects, all the way to terminal malignant cancers.
1. Quantitative Disorders (Abnormalities in Number)
A. Leukocytosis (Too Many WBCs)
Definition: A total white blood cell count exceeding the upper normal limit (>11,000 WBCs/μL).
- Physiologic Causes: Pregnancy, extreme physical exertion, emotional stress, and high cortisol levels cause WBCs stuck to the walls of blood vessels (the marginating pool) to suddenly detach and float freely, artificially raising the blood count without actual new production.
- Pathologic Causes:
- Neutrophilia: Driven heavily by acute bacterial infections (pneumonia, appendicitis) or sterile tissue necrosis (a severe myocardial infarction / heart attack).
- Leukemoid Reaction: A massive, extreme, but benign elevation of WBCs (often >50,000/μL) in response to profound infection (like sepsis) or severe hemorrhage. It mimics leukemia on paper, but the cells are benign, functional responders.
- Lymphocytosis: Classic presentation of acute viral infections (e.g., Infectious Mononucleosis / Epstein-Barr Virus).
- Eosinophilia: Classic presentation of severe allergic asthma, systemic drug reactions, or parasitic helminthic infections (e.g., Ascaris, Schistosoma).
B. Leukopenia (Too Few WBCs)
Definition: A total white blood cell count dropping dangerously below the normal range (<4,000 WBCs/μL).
- Neutropenia (Agranulocytosis): The most clinically terrifying form of leukopenia. Without neutrophils, a patient loses their primary defense against basic bacteria. Minor infections rapidly escalate to lethal septic shock.
Causes include: Heavy radiation therapy, cytotoxic chemotherapy, severe viral destruction of the marrow (HIV/AIDS), or idiosyncratic, deadly reactions to certain medications (e.g., the antipsychotic Clozapine or the anti-thyroid drug Propylthiouracil). - Lymphopenia: Severe depletion of lymphocytes. Seen classically in end-stage HIV/AIDS (which specifically targets and eradicates CD4+ Helper T cells), causing the patient to succumb to bizarre, opportunistic infections.
2. Qualitative Disorders (Abnormal Function or Morphology)
In these genetic disorders, the patient may have a perfectly normal *number* of WBCs, but the cells are structurally defective or biochemically "blind" and useless.
An inherited, benign condition where neutrophils fail to segment properly. The nucleus is permanently hyposegmented (bilobed or entirely unlobed), resembling a classic "pince-nez" (old-fashioned pinching eyeglasses). While structurally bizarre, the cells usually function normally.
A severe, rare autosomal recessive genetic disorder characterized by a defect in microtubule polymerization. The lysosomes in the WBCs cannot fuse with phagosomes.
Hallmarks: Massive, abnormal, giant granules visible in phagocytes; severe albinism (defect in melanin transport); severe peripheral neuropathy; and highly lethal, recurrent pyogenic infections.
A fatal X-linked or autosomal recessive disorder where the neutrophils completely lack the NADPH oxidase enzyme. They can eat bacteria, but they cannot produce the "respiratory burst" (superoxide/bleach) to kill them. Bacteria survive happily inside the neutrophil.
Diagnosis: Diagnosed using the specialized Nitroblue Tetrazolium (NBT) test or Dihydrorhodamine (DHR) flow cytometry. Patients suffer massive, recurrent abscesses from catalase-positive organisms (like Staphylococcus aureus and Aspergillus).
3. Malignant Disorders (Cancers of the White Blood Cells)
When the highly complex genetic code controlling leukopoiesis mutates, WBC precursors begin dividing uncontrollably, refusing to mature, and refusing to die. These malignant clones overrun the bone marrow and systematically destroy the host.
A. The Leukemias ("White Blood")
Cancers originating directly inside the bone marrow, characterized by the explosive proliferation of abnormal, entirely useless, immature WBCs (known as blasts) that pack the marrow space and spill out into the peripheral circulating blood. Because the marrow is choked by blasts, it stops making normal RBCs and platelets, leading to the clinical triad of: Severe Anemia (fatigue), Thrombocytopenia (severe bleeding/bruising), and Neutropenia (massive infections despite a high total WBC count).
- Acute Leukemias: Extremely rapid, aggressive onset. The cells are highly primitive "blasts" that do not function. If untreated, death occurs in weeks to months.
- Acute Lymphoblastic Leukemia (ALL): The most common childhood cancer. Responds well to targeted chemotherapy.
- Acute Myeloid Leukemia (AML): Primarily affects older adults. Pathologists diagnose it by finding characteristic needle-like crystal inclusions called Auer rods inside the myeloblast cytoplasm.
- Chronic Leukemias: Slower, insidious onset spanning years. The mutated cells are more mature, but still functionally abnormal.
- Chronic Myeloid Leukemia (CML): Famously driven by a highly specific genetic chromosomal translocation: t(9;22), creating the Philadelphia Chromosome. This creates a hyperactive tyrosine kinase enzyme. Modern medicine treats this brilliantly with targeted enzyme inhibitors like Imatinib (Gleevec).
- Chronic Lymphocytic Leukemia (CLL): The most common leukemia in Western adults. Often asymptomatic for decades. Characterized on a blood smear by fragile, broken lymphocytes known as "smudge cells."
B. The Lymphomas
Cancers that originate as solid tumors within the secondary lymphatic system (the lymph nodes, spleen, or thymus) rather than floating freely in the blood. They classically present as painless, progressively enlarging, rubbery lymph nodes (lymphadenopathy) accompanied by "B symptoms" (severe drenching night sweats, unexplained spiking fevers, and massive unexplained weight loss).
- Hodgkin Lymphoma (HL): Highly curable. It spreads in an orderly, predictable, contiguous chain from one lymph node group to the next. The absolute diagnostic hallmark is the presence of massive, malignant, multi-nucleated cells that look exactly like an owl's face, known as Reed-Sternberg cells.
- Non-Hodgkin Lymphoma (NHL): A massive, diverse group of highly aggressive B-cell, T-cell, or NK-cell tumors. They spread erratically to non-contiguous lymph nodes and extranodal organs (like the GI tract or brain). Examples include Burkitt Lymphoma (associated with the Epstein-Barr Virus and jaw tumors in Africa) and Diffuse Large B-Cell Lymphoma (DLBCL).
C. Multiple Myeloma
A devastating, specific malignancy of terminally differentiated B-cells (Plasma Cells). Instead of making useful antibodies, the cancerous plasma cells proliferate inside the bone marrow and pump out millions of identical, useless, defective antibodies known as Monoclonal M-proteins. They also produce free light chains (Bence Jones proteins) that travel through the blood and physically clog and destroy the kidneys.
Clinical Hallmarks (The CRAB Criteria):
- C: Calcium elevation (hypercalcemia) due to massive bone destruction.
- R: Renal (Kidney) failure due to toxic Bence Jones proteins.
- A: Anemia due to the marrow being choked by plasma cells.
- B: Bone lesions. The cancer cells secrete chemicals that activate osteoclasts, which literally eat "punched-out" lytic holes into the patient's skull, ribs, and spine, leading to agonizing bone pain and sudden, spontaneous fractures.
VI. Clinical Significance of a Differential White Blood Cell Count
A Complete Blood Count (CBC) with a "Differential" is arguably the most profoundly useful routine diagnostic blood test in modern medicine. While the total WBC count tells you if there is an immune response, the Differential Count breaks down exactly *which* of the five types of WBCs are participating in the battle. This gives the clinician a highly accurate "fingerprint" of the underlying disease process.
1. How a Differential is Performed
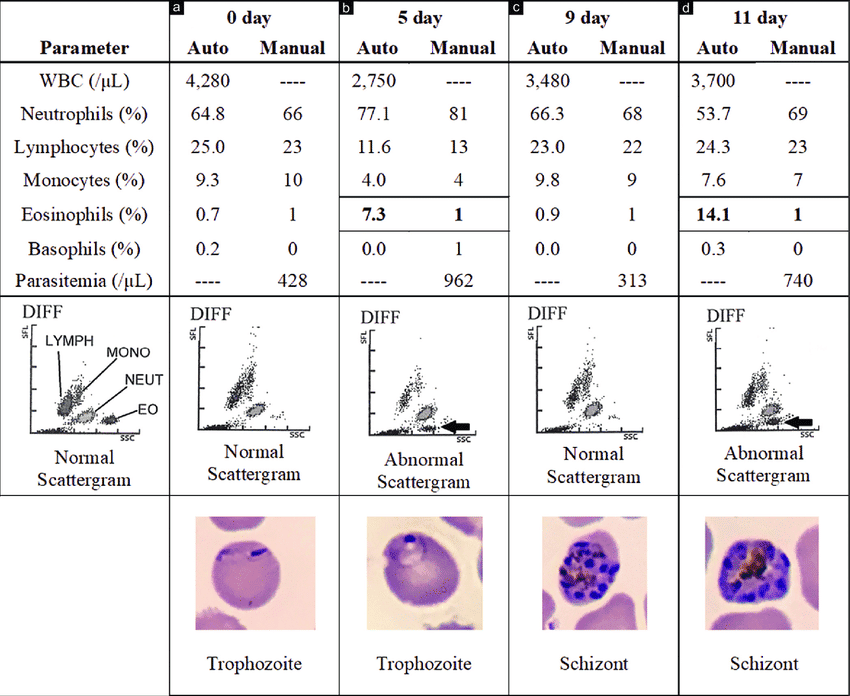
- Automated Flow Cytometry: Modern, high-tech hematology analyzers shoot a laser beam through a microscopic stream of blood. As thousands of cells pass the laser one by one, the machine analyzes the light scatter to instantly determine the exact size, nuclear complexity, and granular density of each individual cell, producing a highly accurate graph.
- Manual Peripheral Blood Smear: If the automated machine detects bizarre, immature blasts or highly atypical cells, a specialized hematology technologist takes a drop of the patient's blood, smears it onto a glass slide, stains it with Giemsa, and physically examines 100 consecutive white blood cells under a high-power microscope to visually confirm the pathology.
2. Interpreting the Differential: Absolute Counts vs. Percentages
A critical clinical rule: Absolute counts are always more important than percentages. If a patient has a massive total WBC count of 50,000, and their lymphocytes represent 10%, they still have 5,000 lymphocytes (which is a high absolute number), even though the percentage looks falsely "low."
Diagnostic Interpretation Patterns
- High Total WBC + Severe Neutrophilia (e.g., 85% Neutrophils) + "Left Shift" (Band Cells):
The classic fingerprint of an Acute Bacterial Infection (like pneumococcal pneumonia, acute appendicitis, or bacterial meningitis). The marrow is fighting a massive bacterial war. - Normal/Slightly High Total WBC + Severe Lymphocytosis (e.g., 60% Lymphocytes) + Atypical Reactive Lymphocytes:
The classic fingerprint of an Acute Viral Infection (e.g., Infectious Mononucleosis / Epstein-Barr, Cytomegalovirus, or viral hepatitis). Viruses hide inside cells, so the body relies entirely on Lymphocytes (T-cell assassins) to kill them, completely ignoring neutrophils. - High Eosinophils (Eosinophilia - e.g., 15%): + Skin Rash or Wheezing:
Highly indicative of an intense systemic Allergic Reaction (severe asthma, drug hypersensitivity, eczema) OR an invasive Parasitic Helminth Infection (like Hookworm or Strongyloides). - Massive Total WBC (e.g., 100,000/μL) + High Monocytes + High Neutrophils + Basophilia:
Often the suspicious fingerprint of a Myeloproliferative Disorder, particularly Chronic Myeloid Leukemia (CML). - Severe Neutropenia (Absolute Neutrophil Count / ANC < 500/μL) + Fever:
This is known as Febrile Neutropenia. It is a massive, life-threatening medical emergency often seen in chemotherapy patients. Because they have zero neutrophils, a simple fever means they have a bacterial infection that will progress to fatal septic shock in hours if not treated immediately with aggressive, broad-spectrum IV antibiotics.
VII. List of References for Further Reading
The exhaustive pathophysiological details, classifications, and diagnostic criteria provided in this master guide are drawn from and corroborated by the following gold-standard medical texts and hematological guidelines:
- Kumar, V., Abbas, A. K., & Aster, J. C. (2020). Robbins and Cotran Pathologic Basis of Disease (10th ed.). Elsevier. (Definitive text for leukocyte pathology, leukemias, and lymphomas).
- Hoffbrand, A. V., & Steensma, D. P. (2019). Hoffbrand's Essential Haematology (8th ed.). Wiley-Blackwell. (Gold standard for leukopoiesis, bone marrow morphology, and blood smear interpretations).
- Hall, J. E., & Hall, M. E. (2020). Guyton and Hall Textbook of Medical Physiology (14th ed.). Elsevier. (Definitive resource on the physiological mechanisms of phagocytosis, innate immunity, and the respiratory burst).
- Loscalzo, J., Fauci, A. S., Kasper, D. L., Hauser, S. L., Longo, D. L., & Jameson, J. L. (2022). Harrison's Principles of Internal Medicine (21st ed.). McGraw Hill. (Standard reference for the clinical interpretation of the differential WBC count, neutropenic emergencies, and multiple myeloma CRAB criteria).
- Abbas, A. K., Lichtman, A. H., & Pillai, S. (2021). Cellular and Molecular Immunology (10th ed.). Elsevier. (Exhaustive detail on T-cell, B-cell, and NK-cell molecular functions and cytokine regulation).
White Blood Cells Quiz
Test your knowledge with these 30 questions.
White Blood Cells Quiz
Question 1/30
Quiz Complete!
Here are your results, .
Your Score
27/30
90%