
Androgens are male sex hormones responsible for the development and maintenance of male characteristics. Androgens include Testosterone, which is primarily produced in the testes, and other androgens produced in the adrenal glands.
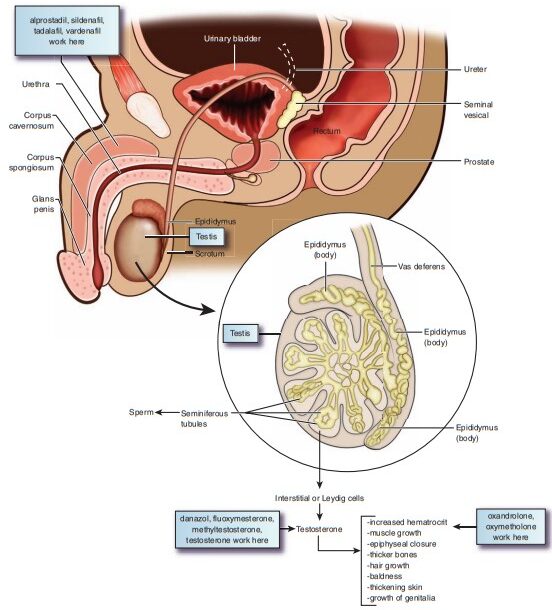
- Androgens are chiefly produced in the testes (by Leydig cells) and in small amounts in the adrenal cortex.
- In females, small amounts of androgens are produced in the ovaries and the adrenal cortex.
- Testosterone is the most important natural androgen. In an adult male, approximately 8–10 mg is produced daily.
- Secretion is regulated by gonadotropins (Luteinizing Hormone - LH, and Follicle-Stimulating Hormone - FSH) and Gonadotropin-Releasing Hormone (GnRH).
- Inadequate production of androgens (hypogonadism) can be due to pituitary malfunction, hypothalamic deficits, testicular atrophy, injury, or removal of testicles.
- Testosterone: The principal androgenic hormone produced by the Leydig cells of the testes.
- Dehydroepiandrosterone (DHEA): A weaker androgen produced by the adrenal cortex.
- Androstenedione: Another weak androgen produced by the adrenal glands and gonads, serving as a precursor to testosterone and estrogens.
| Term | Definition |
|---|---|
| Anabolic Steroids | Synthetic androgens developed with more anabolic (protein-building and muscle-enhancing) effects than androgenic (masculinizing) effects. |
| Androgenic Effects | Effects associated with the development of male sexual characteristics and secondary characteristics (e.g., deepening of voice, facial/body hair distribution, genital development, acne). |
| Androgens | Male sex hormones, primarily testosterone, produced in the testes and adrenal glands. |
| Hirsutism | Abnormal hair distribution associated with male secondary sex characteristics in women (e.g., increased hair on the trunk, arms, legs, and face). |
| Hypogonadism | Underdevelopment or decreased function of the gonads (testes in males, leading to low testosterone levels). |
| Penile Erectile Dysfunction | A condition in which the corpus cavernosum does not fill with adequate blood to allow for a penile erection; can be related to aging, vascular, neurological, or hormonal conditions. |
| Drug Name | Usual Dosage | Usual Indications |
|---|---|---|
| Danazol (Danocrine) | 100–600 mg/day PO, depending on use and response | Prevention of ovulation for the treatment of endometriosis; prevention of hereditary angioedema; fibrocystic breast disease. |
| Fluoxymesterone (Androxy) | 5–20 mg/day PO for replacement therapy; 10–40 mg/day PO for certain breast cancers | Treatment of delayed puberty in male patients and certain androgen-responsive breast cancers in postmenopausal women. |
| Testosterone (Androderm, Depo-Testosterone) | 50–400 mg IM every 2–4 weeks (dose varies with preparation). Dermatological patch: 4–6 mg/day. | Replacement therapy in hypogonadism, delayed puberty, advanced inoperable breast cancer in women. |
| Methyltestosterone (Testred, Virilon) | Males: 10–50 mg/day PO. Females: 50–200 mg/day PO. | Replacement therapy in hypogonadism; treatment of delayed puberty in males; advanced breast cancers in postmenopausal women. |
- Therapeutic Class: Hormone
- Pharmacological Class: Androgen
- Pregnancy Category: Category X (Strictly contraindicated in pregnancy due to fetal masculinization).
- Schedule: Schedule III Controlled Substance (due to high potential for abuse).
- Dosage: 50–400 mg IM every 2–4 weeks; varies with preparation (e.g., Enanthate, Cypionate). Long-acting depository forms are available. Dermatological patch: 4–6 mg/day, replace patch daily. Topical gels and buccal tablets also exist.
Testosterone has two primary categories of effects on the body:
- Increases protein anabolism and decreases protein catabolism (breakdown).
- Maintains bone density and counteracts osteoporosis.
- Regulates fat distribution.
- Supports muscle growth, strength, and overall body mass.
- Speeds up recovery from tissue injury.
- Helps in Red Blood Cell production by stimulating erythropoietin synthesis (erythropoiesis).
- Increases the retention of nitrogen, sodium, potassium, and phosphorus.
- Decreases the urinary excretion of calcium.
- Development and maintenance of male sex organs (penis, scrotum, seminal vesicles, prostate).
- Spermatogenesis and maturation of spermatozoa.
- Enhances sex drive (libido) and increases aggression.
- Stimulates the growth of beard and body hair, while promoting male pattern baldness in genetically susceptible individuals.
- Stimulates sebaceous glands, often leading to acne.
- Deepens the voice by enlarging the larynx and thickening the vocal cords.
- Increased size of the prostate gland.
Testosterone production is tightly regulated by the Hypothalamic-Pituitary-Gonadal (HPG) Axis via a negative feedback loop:
- The Hypothalamus releases Gonadotropin-Releasing Hormone (GnRH).
- GnRH stimulates the Anterior Pituitary Gland (APG) to secrete Follicle-Stimulating Hormone (FSH) and Luteinizing Hormone (LH).
- LH stimulates the Leydig cells in the testes to synthesize and secrete testosterone. (FSH stimulates Sertoli cells for spermatogenesis).
- Negative Feedback: High levels of serum testosterone exert an inhibitory effect:
- The APG suppresses the secretion of LH.
- The Hypothalamus suppresses the release of GnRH.
- Hypogonadism and impotence in males due to testicular, pituitary, or hypothalamic deficiency.
- Treatment of delayed male puberty.
- Breast cancer treatment as a palliative, secondary therapy in postmenopausal women with inoperable, hormone-responsive tumors.
- Prevention of postpartum breast engorgement (historical use).
- Blockage of FSH and LH release in women to prevent ovulation for the treatment of endometriosis (typically using synthetic derivatives like Danazol).
- Prevention of hereditary angioedema.
- Illegally: Sportsmen and bodybuilders often use anabolic steroids and testosterone derivatives to promote musculature and sporting abilities.
- Allergy: Known hypersensitivity to androgens or vehicle ingredients.
- Pregnancy and Lactation: Category X. Causes virilization and severe abnormalities in the female fetus. It is not clear whether androgens enter breast milk, but they are contraindicated.
- Prostate or Breast Cancer in Males: Androgens stimulate the growth of these hormone-dependent carcinomas.
- Liver Dysfunction and Cardiovascular Disease: Can be exacerbated by fluid retention, altered lipid profiles, and hepatotoxicity.
- Nephrosis / Nephritis: Due to increased fluid and sodium retention.
- Black Box Warning (Topical Forms): Risk of virilization (development of male characteristics) in children or women who come into secondary contact with unwashed skin where the drug was applied.
- Black Box Warning (Danazol): Risk of severe thromboembolic events, fetal abnormalities, peliosis hepatis (blood-filled cysts in the liver), and benign intracranial hypertension.
- Use with caution in: Patients with Diabetes Mellitus (can alter blood sugar), Benign Prostatic Hyperplasia (BPH - can cause urinary retention), and Sleep Apnea (androgens may stimulate or worsen obstructive sleep apnea).
- Gynecomastia (breast enlargement due to peripheral conversion of testosterone to estrogen).
- Testicular atrophy and oligospermia/azoospermia (due to negative feedback shutting down endogenous LH/FSH).
- Inhibition of normal testicular function and potential impotence post-use.
- Enlargement of the penis and frequent erections (priapism).
- Male pattern baldness, acne, and oily skin.
- Hepatotoxicity (jaundice, drug-induced hepatitis, hepatic carcinoma—especially with oral 17-alpha-alkylated androgens).
- Psychiatric effects: anxiety, altered mood, depression, increased aggression ("roid rage"), and confusion.
- Systemic effects: edema, nausea, vomiting, headache, fatigue, abdominal cramps, gingivitis.
- Virilization: Acquisition of male sexual characteristics (deepening of the voice, enlargement of the clitoris). These may become irreversible if the drug is not stopped promptly.
- Amenorrhea and severe menstrual irregularities.
- Hirsutism (increased facial and body hair distribution) and male-pattern baldness.
- Acne and oily skin.
- Anticoagulants (Warfarin): Androgens may increase the action of oral anticoagulants, leading to an increased risk of bleeding. Dosage reductions of warfarin are often required, along with strict PT/INR monitoring.
- Oral Hypoglycemic Agents and Insulin: Androgens can decrease blood glucose levels, increasing the risk of hypoglycemia. Diabetic drug dosages may need adjustment.
- Corticosteroids: Concurrent use increases the risk of severe fluid retention and edema formation, which is dangerous for heart failure or renal patients.
- Hepatotoxic drugs: Increased risk of severe liver damage when combined with oral androgens.
- Route-Specific Administration:
- Buccal tablets: Demonstrate placement (between cheek and gum). Warn the patient not to swallow or chew the tablet and allow it to dissolve completely. Instruct the patient not to eat, drink water, or smoke until it is fully dissolved.
- IM Injections: Administer deep IM into the gluteal muscle (upper outer quadrant) using a Z-track method, as the solutions are oil-based and can be highly irritating.
- Oral preparations: Give with or before a meal to decrease gastric upset.
- Transdermal Patches (e.g., Testoderm): Place on clean, dry scrotal skin. Optimal skin contact is achieved by carefully dry-shaving scrotal hair before application. (Note: Androderm patches are applied to non-scrotal skin like the back, abdomen, or thighs).
- Monitoring Parameters:
- Monitor strict fluid input and output. Weigh the patient twice a week to detect fluid retention. Assess for peripheral edema and pulmonary congestion.
- Monitor for changes in secondary sexual characteristics in men and signs of virilization in women (deepening voice, facial hair, clitoromegaly).
- Monitor Hemoglobin and Hematocrit periodically (risk of polycythemia due to increased erythropoiesis).
- Monitor urine and serum calcium levels (risk of hypercalcemia, especially in breast cancer patients with bone metastases).
- Monitor liver function tests (AST, ALT, bilirubin) and lipid profiles (androgens typically lower HDL and raise LDL).
- Advise male patients to immediately report signs of priapism (prolonged, painful erection), difficulty in urinating (signs of BPH exacerbation), or testicular shrinkage.
- Instruct all patients to report signs of hypercalcemia (nausea, vomiting, lethargy, muscle weakness), severe edema, unexpected rapid weight gain, swelling of the feet/ankles, unusual bleeding, or signs of hepatitis (jaundice, dark urine, right upper quadrant pain).
- Explain the strict rationale for prohibiting the illicit use of testosterone and anabolic steroids for increasing athletic performance (severe cardiovascular, hepatic, and psychiatric risks).
- Females must strictly avoid pregnancy and notify the physician immediately if pregnancy is suspected. Instruct female patients to report signs of virilization immediately, as some changes (voice deepening) can be irreversible.
- Diabetic patients must monitor their blood sugar closely as hypoglycemia may occur.
- Emphasize the need for regular follow-up, laboratory tests (lipids, LFTs, CBC, PSA for men), and physical examinations.
Anabolic steroids are synthetic agents that have been structurally modified to maximize anabolic effects (tissue-building) while minimizing androgenic effects (masculinization). They are derivatives of testosterone and are designed to prevent the conversion to the potent androgen 5-alpha-dihydrotestosterone (DHT).
All of these drugs are regulated as Schedule III controlled substances, making their use by athletes without a prescription illegal. Notable examples include:
| Drug Name | Description and Details |
|---|---|
| Nandrolone (Deca-Durabolin) | A steroid naturally produced by the body in trace amounts, but synthetically manufactured in high doses. Highly anabolic. Professional athletes like Barry Bonds and Roger Clemens allegedly used nandrolone illegally to enhance performance. |
| Stanozolol (Winstrol) | A synthetic steroid that is unusual because it can be taken orally and survives first-pass metabolism. Baseball players like Rafael Palmeiro tested positive for its illegal use. Strength athletes use it to quickly build power. |
| Oxandrolone (Anavar) | An oral synthetic steroid approved for medical use in treating severe weight loss (e.g., post-surgery, chronic infection) and osteoporosis. Bodybuilders abuse it to rapidly create greater muscle mass. |
| Methenolone (Primobolan) | A mild anabolic steroid with very low androgenic properties, available in both oral and injectable forms. |
| Methandrostenolone (Dianabol) | One of the most popular and historically abused oral anabolic steroids; highly hepatotoxic and known for rapid muscle and water retention. |
- Severe Catabolic States: Acute illness, severe trauma, major surgery, extensive burns, or HIV/AIDS-related muscle wasting. Enhances appetite, improves nitrogen balance, and promotes a feeling of well-being.
- Osteoporosis: To counteract bone loss and stimulate bone formation, particularly in chronic glucocorticosteroid therapy or refractory postmenopausal osteoporosis.
- Sub-optimal Growth: Stimulates linear growth in prepubertal boys with growth failure.
- Renal Diseases: Treatment of severe anemia associated with chronic renal failure (stimulates erythropoietin).
- Male patients with known or suspected carcinoma of the breast or prostate.
- Carcinoma of the breast in females with hypercalcemia (androgenic anabolic steroids may stimulate osteolytic bone resorption).
- Pregnancy (Category X) due to severe masculinization of the female fetus.
- Nephrosis or the nephritic phase of nephritis.
- Severe hepatic dysfunction.
- Dermatological: Severe cystic acne, oily skin, and hair loss (premature male pattern baldness).
- Hepatic: Severe liver diseases, including peliosis hepatis (blood-filled cysts in the liver) and hepatic carcinoma.
- Cardiovascular: Alteration in blood lipids (lowered HDL, elevated LDL), high blood pressure, increased risk of blood clotting, heart attacks, stroke, and left ventricular hypertrophy.
- Psychiatric: Altered mood, irritability, intense aggression ("roid rage"), severe depression during withdrawal, and suicidal tendencies.
- Reproductive (Males): Gynecomastia (abnormal mammary gland development due to aromatization to estrogen), shrinking of testicles (testicular atrophy), azoospermia (absence of sperm, leading to infertility), prostate enlargement, and prostate cancer.
- Reproductive (Females): Menstrual irregularities, infertility, excess facial or body hair (hirsutism), clitoral enlargement, and a deeper, masculine voice.
- Musculoskeletal: Stunted growth in teens due to premature closure of the epiphyseal growth plates; increased risk of tendon damage/rupture.
- Infectious: High risk of viral (HIV, Hepatitis B/C) or bacterial infections due to shared or unsterile injection practices.
- General: Edema (fluid retention) and injury from skin-to-skin transfer of topical testosterone gels.
Anticoagulants: Anabolic steroids may severely increase sensitivity to oral anticoagulants (e.g., warfarin). The dosage of the anticoagulant often has to be decreased to maintain the prothrombin time (PT/INR) at the desired therapeutic level. Patients receiving oral anticoagulant therapy require very close monitoring, especially when anabolic steroids are started, adjusted, or stopped.
The physician and nurse should instruct patients to immediately report any of the following effects, which may indicate severe toxicity or virilization:
- Hoarseness or deepening of the voice (females).
- Severe acne or oily skin changes.
- Changes in menstrual periods or completely missed periods.
- Development of more hair on the face or body (hirsutism).
- Nausea, vomiting, right upper quadrant abdominal pain, or yellowish skin/eyes (jaundice).
- Changes in skin color.
- Ankle swelling or unexpected rapid weight gain (edema).
Antiandrogens, also known as androgen antagonists or testosterone blockers, are a class of drugs that prevent androgens from mediating their biological effects in the body. They act primarily by blocking the androgen receptor directly, inhibiting the enzymes responsible for androgen synthesis, or suppressing pituitary gonadotropin production.
- 5-Alpha-Reductase Inhibitors: Finasteride, Dutasteride
- Androgen Receptor Antagonists (Non-steroidal): Flutamide, Bicalutamide, Nilutamide
- Androgen Receptor Antagonists (Steroidal): Cyproterone acetate, Spironolactone
- Gonadotropin Suppressants / Weak Androgens: Danazol
- Steroidogenesis Inhibitors: Ketoconazole
- Available preparations: Tablets (1 mg and 5 mg). Brands: Propecia (1 mg), Proscar (5 mg).
- Mechanism of Action: It is a specific inhibitor of the enzyme 5-alpha-reductase, which is responsible for converting testosterone to its highly potent active metabolite, 5-alpha-dihydrotestosterone (DHT) in the prostate, liver, and skin. The development of the prostate gland and the miniaturization of hair follicles are dependent on DHT. By lowering serum and tissue levels of DHT, finasteride decreases prostate size and halts hair loss. (Note: Dutasteride inhibits both type 1 and type 2 5-alpha-reductase, making it even more potent and long-acting).
- Indications & Dose:
- Benign Prostatic Hyperplasia (BPH): 5 mg once daily. It shrinks the prostate, improving urine flow. Often used in combination with alpha-1 blockers.
- Androgenetic Alopecia (Male pattern baldness): 1 mg/day for 3 months or more (for men only).
- Side Effects: Decreased libido, decreased volume of ejaculation, erectile dysfunction/impotence, breast tenderness and enlargement (gynecomastia), and testicular pain.
- Contraindications: Known hypersensitivity. Women of childbearing potential. Use with caution in hepatic impairment.
- Nursing Implications:
- Assess for symptoms of BPH (e.g., feeling of incomplete bladder emptying, weak stream, urgency).
- Digital rectal examination (DRE) should be done before therapy and periodically during treatment.
- Monitor baseline and periodic Prostate Specific Antigen (PSA) levels. Note: Finasteride artificially lowers PSA levels by about 50%, which must be accounted for when screening for prostate cancer.
- The drug can be taken without regard to meals.
- Patient/Family Teaching:
- Teratogenic Risk: Finasteride possesses a severe risk to a male fetus (abnormal genitalia development). Pregnant women or women who may become pregnant must absolutely NOT handle crushed or broken tablets.
- Tell male patients to inform the doctor immediately if their sexual partner is or may become pregnant; additional measures such as discontinuing the drug or strict use of condoms may be necessary, as the drug is secreted in semen.
- Explain that it may take 3-6 months to see a clinical improvement in BPH or hair loss.
- Mechanism: Non-steroidal androgen receptor antagonists. They competitively bind to target cell androgen receptors (e.g., in the prostate), blocking the uptake and binding of testosterone and DHT.
- Indications: Primarily used in the treatment of metastatic prostate carcinoma (often combined with a GnRH agonist to prevent the initial tumor flare and block adrenal androgens). Flutamide is also used off-label for severe female hirsutism.
- Dosage Example: Flutamide 250 mg every 8 hours; Bicalutamide 50 mg daily.
- Side Effects: Severe hot flashes, chills, edema, loose stools/diarrhea, extreme gynecomastia, breast tenderness, and severe hepatotoxicity (especially Flutamide; Bicalutamide is less hepatotoxic and longer-acting).
- Mechanism: Primarily a potassium-sparing diuretic (aldosterone antagonist). However, it also acts as a competitive antagonist at the androgen receptor and inhibits ovarian and adrenal steroidogenesis enzymes.
- Indications (Antiandrogen use): Used off-label heavily in dermatology and gynecology to treat female hirsutism, severe hormonal acne, and Polycystic Ovary Syndrome (PCOS).
- Side Effects: Hyperkalemia, hypotension, menstrual irregularities, and gynecomastia (in males).
- Mechanism: A synthetic steroid with weak androgenic properties that acts to suppress the pituitary-ovarian axis. It strongly inhibits the release of gonadotropins (LH and FSH), resulting in profound suppression of testicular and ovarian function.
- Indications: Endometriosis, menorrhagia, fibrocystic breast disease, and prevention of attacks in hereditary angioneurotic edema.
- Side Effects: Weight gain, acne, hirsutism, deepening of the voice, liver dysfunction, and lipid alterations.
- Mechanism: A steroidal antiandrogen that blocks androgen receptors and possesses strong progestational activity, which suppresses the release of LH and FSH.
- Indications: Inoperable prostate cancer, severe hypersexuality/sexual deviation in males, and severe hirsutism/acne in females (often formulated with ethinylestradiol as an oral contraceptive, e.g., Diane-35).
- Mechanism: Primarily an imidazole antifungal agent. However, at high systemic doses (e.g., 400 mg every 8 hours), it profoundly inhibits cytochrome P450 enzymes involved in gonadal and adrenal steroid hormone biosynthesis (effectively stopping testosterone production).
- Indications: Advanced, castration-resistant prostate cancer (off-label) when rapid reduction of testosterone is required.
- Side Effects: Severe hepatotoxicity, adrenal insufficiency, and significant drug-drug interactions.
| No. | Nursing Diagnosis | Interventions & Rationale |
|---|---|---|
| 1 | Excess Fluid Volume related to sodium and water retention secondary to androgen therapy. |
|
| 2 | Disturbed Body Image related to irreversible masculinizing effects in females (virilization) or feminizing effects in males (gynecomastia). |
|
| 3 | Risk for Impaired Liver Function related to the hepatotoxic nature of 17-alpha-alkylated androgens and anabolic steroids. |
|
| 4 | Deficient Knowledge / Risk for Abuse related to illicit use for athletic enhancement and complex therapeutic regimens. |
|
- Vallerand, A. H., & Sanoski, C. A. (2020). Davis's Drug Guide for Nurses (17th ed.). F.A. Davis Company.
- Burchum, J., & Rosenthal, L. (2021). Lehne's Pharmacology for Nursing Care (11th ed.). Elsevier.
- Katzung, B. G., & Vanderah, T. W. (2021). Basic & Clinical Pharmacology (15th ed.). McGraw Hill.
- American Academy of Pediatrics (AAP) and relevant endocrine society guidelines regarding hypogonadism and benign prostatic hyperplasia management.
Quick Quiz
Androgens Quiz
Pharmacology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Androgens Quiz
Pharmacology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.
I’m extremely impressed with your writing skills
and also with the layout on your weblog. Ιs this a paid theme or did you customize it yoᥙrself?
Anyway keep up thе nice quality wrіting, іt is rare to sеe a
great blog like this one today.