
Hand Hygiene
I. Introduction & Historical Context
Hand hygiene is universally recognized as the single most important, simplest, and least expensive means of reducing the prevalence of Healthcare-Associated Infections (HAIs) and combating the spread of antimicrobial resistance. It creates a mutually protective barrier, shielding both healthcare personnel (HCP) and patients from resistant pathogens.
Historical Milestone:
In 1822, a French pharmacist demonstrated that solutions containing chlorides of lime or soda could eradicate the foul odors of human corpses. This pivotal discovery proved that such solutions could be utilized effectively as disinfectants and antiseptics in medical practice.
II. Microbiology: Normal Bacterial Skin Flora
Normal human skin is naturally colonized with bacteria, but the concentration varies drastically depending on the anatomical region.
Bacterial Load by Body Area:
- Scalp: 1 × 106 Colony Forming Units (CFUs)/cm²
- Axilla (Armpit): 5 × 105 CFUs/cm²
- Abdomen: 4 × 104 CFUs/cm²
- Forearm: 1 × 104 CFUs/cm²
- Hands of Medical Personnel: Range from 3.9 × 104 to 4.6 × 106 CFUs/cm²
Skin Squames & Environmental Contamination:
- Humans shed approximately 1 million (106) skin squames (dead skin cells) containing viable microorganisms every single day.
- Clinical Impact: These squames easily contaminate patient gowns, bed linens, bedside furniture, and other immediate environmental objects.
Transmission During "Clean" Activities:
Healthcare workers frequently contaminate their hands during seemingly "clean" tasks, such as lifting a patient, taking a pulse/blood pressure, measuring oral temperature, or simply touching a patient's hand, shoulder, or groin.
Note: Perineal or inguinal (groin) areas of normal, intact patient skin are usually the most heavily colonized.
Transient vs. Resident Flora
Bacteria recovered from hands fall into two distinct categories. Understanding the difference is critical for NCLEX and clinical practice:
- Transient Flora: Colonize the superficial layers of the skin. They are easily picked up from patients and surfaces, but are highly amenable to removal by routine handwashing. Transient flora are the primary culprits behind HAIs.
- Resident Flora: Attached to the deeper layers of the skin (and hair follicles). They are part of the body's normal defense but are much more resistant to removal.
III. Standard Definitions & Terminology
To standardize infection control protocols, precise terminology must be used.
- Hand Hygiene (The Umbrella Term): A general term applying to handwashing, antiseptic handwash, antiseptic hand rub, or surgical hand antisepsis.
- Handwashing vs. Antiseptic Handwash:
- Handwashing: Washing hands with plain (non-antimicrobial) soap and water. Plain soap contains no antimicrobial agents (or only trace amounts as preservatives).
- Antiseptic Handwash: Washing hands with water and soap/detergents that contain an active antiseptic agent.
- Antiseptic Agents: Antimicrobial substances applied to the skin to reduce microbial flora (e.g., alcohols, chlorhexidine, chlorine, iodine, triclosan).
- Alcohol-Based Hand Rub (ABHR): An alcohol-containing preparation (usually 60%–95% ethanol or isopropanol) applied to hands to reduce viable microorganisms.
- Decontaminate Hands: The process of reducing bacterial counts by performing an antiseptic hand rub OR antiseptic handwash.
- Surgical Hand Antisepsis: An intense antiseptic handwash or hand rub performed preoperatively to completely eliminate transient flora and temporarily reduce resident flora.
❓ Applied Clinical Question: Flora Management
Case: A nursing student finishes inserting an IV for a patient. The student washes their hands thoroughly with soap and water. Which type of skin flora is the student primarily removing, and why is this critical for patient safety?
Answer: The student is primarily removing Transient Flora. This is critical because transient flora sit on the superficial skin layers, are easily acquired from patient contact, and are the most frequent cause of Healthcare-Associated Infections (HAIs) transmitted via cross-contamination.
IV. Methods and Indications for Hand Hygiene
Hand hygiene primarily involves three types: Handwashing, Hand rubs, and Surgical scrubs. Each has specific indications based on clinical context.
Alcohol-Based Hand Sanitizers (ABHS) - The Preferred Method:
ABHS is the most effective product for reducing germs and is the preferred method in most clinical situations.
When to use ABHS:
- Immediately before touching a patient.
- Before performing an aseptic task or handling invasive medical devices.
- Before moving from a soiled body site to a clean body site on the same patient.
- After touching a patient or their immediate environment.
- After contact with blood, body fluids, or contaminated surfaces (if hands are NOT visibly soiled).
- Immediately after glove removal.
Handwashing (Soap and Water) - The Mandatory Alternative:
The fundamental practice of using soap and water to physically remove dirt, debris, and microorganisms.
When you MUST use Soap and Water:
- Whenever hands are visibly dirty or soiled.
- Before eating and after using the restroom.
- After caring for a person with known/suspected infectious diarrhea.
- After known/suspected exposure to spores (e.g., Bacillus anthracis, Clostridioides difficile).
The Spore Exception
Why is ABHS ineffective against C. difficile? Alcohol denatures proteins, but spores have a tough, dormant outer coating that is highly resistant to alcohol. Washing with soap and water doesn't necessarily "kill" the spores, but the mechanical friction and rinsing action physically washes the spores off your hands and down the drain.
V. Proper Techniques for Hand Hygiene
Effective hand hygiene requires access to products, knowledge of when to perform it, and strict adherence to the correct technique.
Technique: Using ABHS (Hand Rub):
- Apply product to the palm and rub hands together.
- Cover all surfaces (palms, dorsum, between fingers, thumbs).
- Continue rubbing until hands feel completely dry (This should take around 20 seconds).
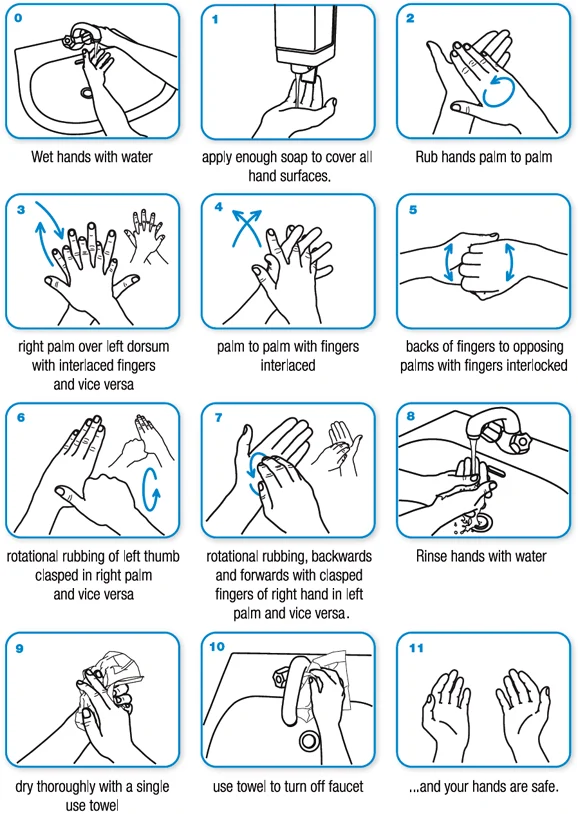
Technique: Washing with Soap and Water:
- Wet hands first with water, then apply the manufacturer-recommended amount of soap.
- Rub hands together vigorously for at least 15 seconds, covering all surfaces.
- Rinse with water and dry thoroughly using disposable towels.
- Crucial Step: Use the disposable towel to turn off the faucet (prevents re-contaminating clean hands).
Dermatology Note: Avoid using hot water. Hot water strips protective skin oils, leading to dryness, micro-tears, and dermatitis, which increases bacterial colonization.
VI. Hand Hygiene for Surgery (Surgical Scrubs)
Surgical scrubs are an intensive cleansing process designed to eradicate potential pathogens from the hands and forearms before invasive procedures.
- Pre-Scrub Preparation: Remove all rings, watches, and bracelets. Remove debris from underneath fingernails using a nail cleaner under running water.
- Using Antimicrobial Soap: Scrub hands and forearms for the length of time recommended by the manufacturer (usually 2–6 minutes).
- Using Alcohol-Based Surgical Scrub (Persistent Activity): Prewash hands/forearms with non-antimicrobial soap, dry completely, then apply the alcohol solution as directed. Allow to dry thoroughly before donning sterile gloves.
- Surgical Rationale: Scrubbing with an antiseptic slows bacterial growth. Reducing resident flora reduces the risk of bacteria releasing into the surgical field if gloves are punctured or torn. Double gloving is strongly advised during invasive surgeries due to increased blood exposure risk.
❓ NCLEX-Style Question: Surgical Prep
Question: A perioperative nurse is preparing to use an alcohol-based surgical hand-scrub product before a procedure. What must the nurse do before applying the alcohol scrub?
Answer: The nurse must prewash hands and forearms with a non-antimicrobial soap and dry them completely. Applying alcohol to wet hands dilutes the alcohol concentration, rendering it ineffective at achieving the required 60-95% germicidal threshold.
VII. Analysis of Preparations Used for Hand Hygiene
Different chemical agents have varied mechanisms of action, speeds of onset, and target pathogens. Healthcare facilities select agents based on these specific profiles.
| Preparation | Mechanism of Action & Characteristics | Antimicrobial Efficacy |
|---|---|---|
| Plain Soap (Non-Antimicrobial) |
Contains esterified fatty acids and sodium/potassium hydroxide. | Minimal intrinsic antimicrobial activity. Functions mechanically to remove loosely adherent transient flora. |
| Alcohols (60%–95% ethanol or isopropanol) |
Denatures proteins. Rapidly germicidal upon application, but has no persistent (residual) activity. | Excellent against gram-positive & gram-negative vegetative bacteria, multidrug-resistant pathogens (MRSA, VRE), Mycobacterium tuberculosis, fungi, and viruses. |
| Chlorhexidine | Attaches to and disrupts the cytoplasmic membrane, resulting in cellular content precipitation. Immediate activity is slower than alcohol, but it has excellent residual activity. | Good against gram-positive bacteria. Less effective against gram-negative bacteria and fungi. Minimal activity against tubercle bacilli (TB). |
| Iodine and Iodophors (5%–10%) |
Rapidly penetrates cell walls; forms complexes with amino acids/fatty acids to impair protein synthesis and alter cell membranes. | Bactericidal against gram-positive, gram-negative, and spore-forming bacteria. |
| Chloroxylenol (PCMX) | Causes inactivation of bacterial enzymes and alteration of cell walls. | Moderate general antimicrobial activity. |
| Hexachlorophene | Inactivates essential enzyme systems. It is bacteriostatic (prevents growth rather than killing outright). | Good activity against S. aureus. Weak against gram-negative bacteria, fungi, and mycobacteria. |
| Quaternary Ammonium Compounds | Nitrogen atom linked to four alkyl groups (e.g., benzalkonium chloride, cetrimide). | Widely used as general antiseptics; good surface-level decontamination. |
| Triclosan (0.2%–2%) |
Enters bacterial cells and affects the cytoplasmic membrane and synthesis of RNA, fatty acids, and proteins. | Broad-spectrum antimicrobial activity. |
Alcohol vs. Chlorhexidine
To remember the clinical difference between the two most common agents:
- Alcohol is the ASSASSIN: It strikes fast, kills everything instantly (MRSA, VRE, TB), but leaves the scene immediately (no residual activity).
- Chlorhexidine is the GUARD: It takes a little longer to set up (slower immediate action), but stays on duty for hours (excellent persistent/residual activity).
VIII. Product Selection & Compliance
Choosing the right hand hygiene product is essential for institutional compliance. If products irritate the skin or are inconvenient, healthcare workers will not use them.
Factors Influencing Product Selection:
- Relative efficacy, cost, availability, and dispenser convenience.
- Dermal tolerance: Must minimize skin reactions.
- Aesthetic preferences: Fragrance, color, texture, lack of "stickiness," and rapid drying time.
- Freedom of choice by HCP at an institutional level (giving staff input increases compliance).
IX. Barriers to Hand Hygiene Adherence
Despite knowing the importance of hand hygiene, adherence is often suboptimal. Barriers are divided into observed risks, self-reported factors, and perceived institutional barriers.
Statistically linked to poor adherence:
- Physician status or Nursing Assistant status (rather than Registered Nurse status).
- Male sex.
- Working in an Intensive Care Unit (ICU) or working during the week (vs. weekends).
- Wearing gowns/gloves (creates a false sense of security).
- Activities with high risks of cross-transmission.
Excuses/Complaints:
- Irritation/dryness from agents.
- Inconveniently located sinks or lack of soap/paper towels.
- Understaffing, overcrowding, or insufficient time (patient needs taking priority).
- Dangerous Beliefs: Skepticism regarding the value of hand hygiene, or the belief that wearing gloves obviates (removes) the need for hand hygiene.
How to fix the problem:
- Education, routine observation with feedback, and engineering controls (e.g., automated dispensers).
- Administrative sanctions for non-compliers and rewards for compliers.
- Avoiding overcrowding and understaffing.
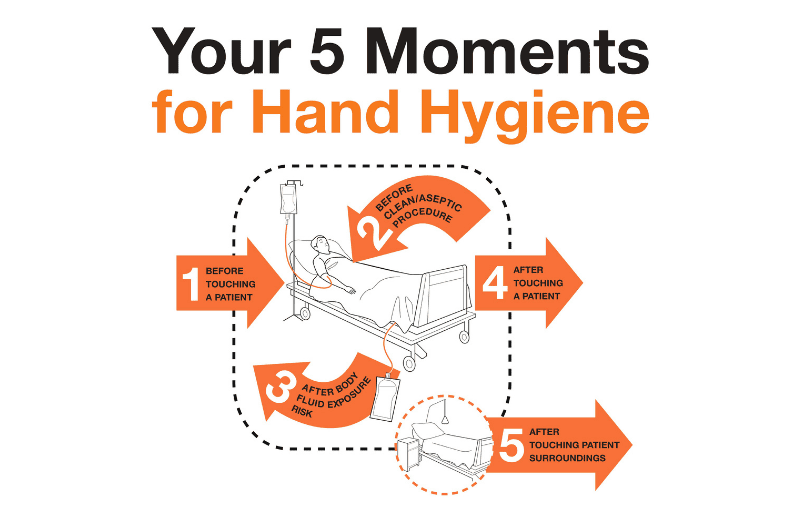
X. The WHO "5 Moments of Hand Hygiene"
Developed by the World Health Organization, this is a key, evidence-based strategy to protect patients, HCP, and the environment against the spread of pathogens.
- Before touching a patient. (Protects patient against harmful germs carried on your hands).
- Before a clean/aseptic procedure. (Protects patient against harmful germs, including their own, from entering their body).
- After a procedure or body fluid exposure risk. (Protects you and the healthcare environment from harmful patient germs).
- After touching a patient. (Protects you and the healthcare environment).
- After touching a patient's surroundings. (Protects you and the healthcare environment, even if you didn't touch the patient directly).
XI. Hand Hygiene Assessment
Continuous assessment identifies areas for improvement and leads to successful interventions to boost compliance.
- Assessments are based on the WHO Hand Hygiene Self-Assessment Framework.
- Assessment Methods Include: Direct observation, self-reporting, and modern electronic monitoring systems.
❓ Applied Clinical Question: The Glove Myth
Case: A physician conducts a brief abdominal exam on a patient while wearing gloves. After the exam, the physician removes the gloves, throws them in the trash, and moves directly to type on the computer charting system. Based on hand hygiene adherence data, what error has occurred?
Answer: The physician has failed to perform hand hygiene after removing gloves. This is tied to a common self-reported barrier: the false belief that glove use negates the need for hand hygiene. Gloves often develop microscopic tears, and hands become moist incubators for bacteria while gloved. Hand hygiene is mandatory immediately after glove removal (WHO Moment 4).