
Cholinergic Receptors, Signaling, and Effects
By the conclusion of this exhaustive master guide, you will be deeply conversant with:
- The major systems and specific organs innervated by Autonomic Cholinergic systems.
- The complete lifecycle of Acetylcholine (ACh): synthesis, storage, release, and degradation, along with the specific drugs that block each step.
- The distinct tissue expression profiles and molecular signaling mechanisms of Nicotinic (N) and Muscarinic (M) receptors.
- The profound organ system effects resulting from cholinergic stimulation (toxicity) versus cholinergic antagonism, memorized via classic clinical mnemonics.
I. Introduction: The Cholinergic Neuron and Autonomic Innervation
In the vast communication network of the nervous system, Acetylcholine (ACh) is arguably the most widely utilized neurotransmitter. Neurons that synthesize, store, and release ACh are explicitly termed Cholinergic Neurons.
To master pharmacology, you must first memorize the exact anatomical locations where ACh acts as the primary messenger. ACh is NOT just a parasympathetic chemical; its reach is much broader.
Where is Acetylcholine Used?
- All Autonomic Ganglia: Both Sympathetic and Parasympathetic preganglionic fibers release ACh to stimulate nicotinic receptors on the postganglionic neuron.
- All Postganglionic Parasympathetic Fibers: These release ACh directly onto target organs (heart, gut, glands) to stimulate muscarinic receptors.
- The Adrenal Medulla: Sympathetic preganglionic fibers release ACh directly into the adrenal medulla to trigger the massive systemic release of Adrenaline/Noradrenaline into the blood.
- The Somatic Nervous System (Voluntary Muscle): Motor neurons release ACh directly onto skeletal muscle to trigger voluntary movement via Nicotinic (NM) receptors.
- The Sympathetic "Exception" (Sweat Glands): While almost all sympathetic postganglionic fibers release Noradrenaline, the sympathetic fibers innervating eccrine sweat glands uniquely release ACh to stimulate muscarinic receptors.
- The Central Nervous System (CNS): Cholinergic neurons play vital roles in the brain regarding memory, learning, and arousal. (Pathology Note: The profound loss of cholinergic neurons in the brain is a hallmark of Alzheimer's Disease).
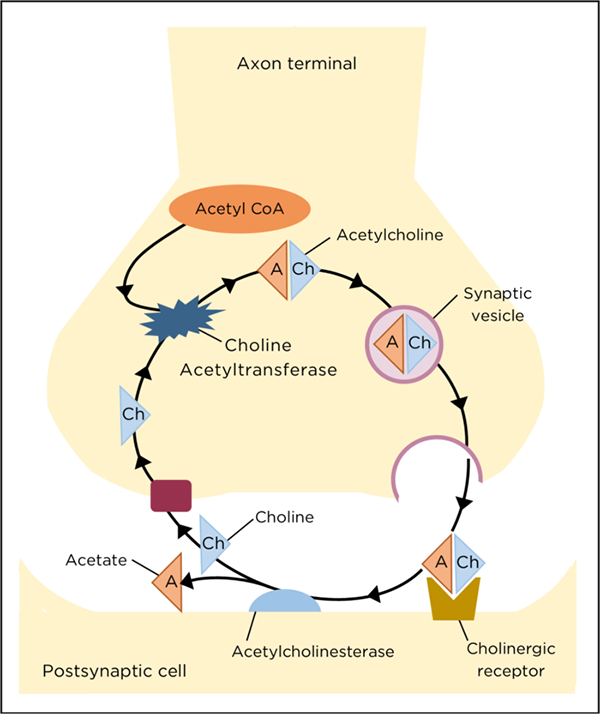
II. The Lifecycle of Acetylcholine (Neurotransmission)
The synapse is the site most amenable to pharmacological manipulation. We can design drugs to target every single stage of ACh's life. The lifecycle consists of five distinct sequential steps.
Making the Neurotransmitter
- The Ingredients: ACh is synthesized in the nerve terminal cytosol from two precursors: Choline and Acetyl Coenzyme A (Acetyl-CoA).
- The Process: Choline is transported from the extracellular fluid into the neuron by a sodium-dependent, energy-requiring active transport carrier. Because Choline has a quaternary nitrogen (carrying a permanent positive charge), it cannot diffuse passively through the membrane. Acetyl-CoA is produced by the mitochondria.
- The Enzyme: Choline Acetyltransferase (ChAT) catalyzes the reaction, merging them to form ACh.
- The Rate-Limiting Step: The active uptake of choline into the cell is the bottleneck.
- Drug Intervention: Hemicholinium is a research drug that blocks the choline transporter, starving the cell of raw materials and preventing ACh synthesis.
Packaging for the Future
- The Process: Once synthesized, free-floating ACh is rapidly packaged into presynaptic vesicles to protect it from degradation. This is an active transport process driven by the efflux of protons (H+).
- Cotransmission: A mature vesicle is not just full of ACh. It contains ACh + ATP + Proteoglycans. ATP acts as a cotransmitter at prejunctional purinergic receptors to provide negative feedback.
- Drug Intervention: Vesamicol acts as a blockade here. It inhibits the vesicular ACh transporter (VAT), preventing ACh from being loaded into vesicles. The empty vesicles are useless upon release.
The Calcium Trigger
- The Process: An action potential (electrical wave driven by Na+ channels) arrives at the nerve terminal. This electricity forces Voltage-Sensitive Calcium (Ca2+) Channels to snap open.
- The Trigger: Ca2+ rushes into the cell. Elevated intracellular calcium causes the ACh vesicles to fuse tightly with the presynaptic membrane (via SNARE proteins) and dump their contents into the synaptic cleft via exocytosis.
- Drug Intervention (Blockade): Botulinum Toxin (Botox) destroys the SNARE fusion proteins. Without fusion, ACh is trapped inside. This causes severe flaccid paralysis. (Clinically used to treat muscle spasms, excessive sweating, and wrinkles).
- Drug Intervention (Massive Release): Black Widow Spider Venom (α-Latrotoxin) forces all the stored vesicles to dump their ACh into the cleft at once, causing violent muscle cramps and spastic paralysis, followed eventually by depletion.
Action and Feedback
- Post-synaptic Binding: ACh diffuses across the microscopic synaptic cleft and binds to post-synaptic receptors (Muscarinic or Nicotinic), triggering the physiological response in the target organ.
- Pre-synaptic Modulation: ACh also binds to pre-synaptic autoreceptors, which act as a thermostat to provide negative feedback and regulate further release.
Termination
- Enzymatic Cleavage: Unlike other neurotransmitters that undergo reuptake whole, ACh action is terminated by rapid hydrolysis in the synaptic cleft.
- The Enzyme: Acetylcholinesterase (AChE) is one of the fastest enzymes in the body, cleaving ACh into Acetate and Choline in milliseconds.
- Choline Recycling: The leftover Choline is recaptured by the high-affinity sodium-coupled transporter (ChT) to be recycled into the next batch of neurotransmitter.
Chemistry Deeper: The Mechanism of Acetylcholinesterase (AChE)
Understanding how AChE destroys Acetylcholine is crucial because blocking this enzyme is a major pharmacological strategy. The degradation involves precise chemical steps within the enzyme's active site:
- Binding: ACh binds to the active site of AChE.
- Transient Intermediate: A temporary chemical bond forms involving the -OH group of Serine 203 (as well as Glutamate and Histidine residues in the catalytic triad).
- Cleavage: Choline is broken off and released, leaving the enzyme temporarily "acetylated" (holding the acetate piece).
- Deacylation: Water enters and rapidly strips the acetate off the enzyme, regenerating the naked AChE so it can instantly destroy the next ACh molecule.
III. Indirect Cholinergic Agonism (AChE Inhibitors)
If we want to stimulate the parasympathetic nervous system, we can either give a drug that acts exactly like ACh (a Direct Agonist like Carbachol or Pilocarpine), or we can use a much more devious strategy: Indirect Agonism.
Mechanism: Indirect agonists do NOT bind to the receptor. Instead, they attack and disable Acetylcholinesterase (AChE). By killing the "garbage men" of the synapse, natural ACh builds up to massive, localized concentrations, continuously hammering the receptors. The net effect is powerfully agonistic.
- Reversible Inhibitors: These drugs temporarily bind to AChE (for minutes to hours).
Examples: Physostigmine (crosses into the brain, used for anticholinergic toxicity), Neostigmine (does not cross into the brain, used heavily to treat Myasthenia Gravis to increase ACh at the muscles). - Irreversible Inhibitors: These permanently, covalently bind to the Serine residue of AChE. The enzyme is dead forever. The body must spend days synthesizing brand new enzymes.
Examples: Organophosphates (found in lethal nerve gases like Sarin, and agricultural insecticides like Parathion). This causes a terrifying, often fatal toxic cascade (The SLUDGE/DUMBELS crisis).
IV. The Cholinergic Receptors: Nicotinic (N)
ACh exerts its magic by interacting with two vastly different families of receptors. We begin with the Nicotinic receptors, named because they are activated by the plant alkaloid Nicotine (from Nicotiana tabacum).
Receptor Physiology: The Ligand-Gated Ion Channel
Nicotinic receptors are Ionotropic. They do not use slow G-proteins. The receptor itself physically surrounds a central pore. When two ACh molecules bind to the outer α-subunits, the pore snaps open instantly. Sodium (Na+) rushes in, causing rapid, localized depolarization. If enough Na+ enters, an action potential fires or a muscle violently contracts.
Dose-Dependent Phenomenon: In small doses, Nicotine stimulates autonomic ganglia. However, if massive, continuous doses are applied, the receptor becomes exhausted and locked in a desensitized state. Thus, intense stimulation is quickly followed by a total blockade of transmission.
Nicotinic Subtypes and Locations:
- NN (Nicotinic-Neuronal): Located in ALL autonomic ganglia and the Adrenal Medulla. Controls the firing of post-ganglionic nerves and adrenaline secretion.
- NM (Nicotinic-Muscle): Located on the somatic motor end-plate of voluntary skeletal muscle. Controls voluntary muscle contraction.
Nicotinic Receptor Antagonists (Blockers)
In surgery, we need to paralyze muscles so the surgeon can cut without the patient twitching. We use Neuromuscular Blocking Agents (NMBAs) which target the NM receptor. They come in two distinct flavors:
- Competitive (Non-Depolarizing) Blockers: These are bulky drugs that physically sit over the ACh binding site like a heavy cap. They do nothing but block the door.
Example: Curare derivatives, Pancuronium, Rocuronium. - Depolarizing (Destructing) Blockers: A fascinating, dangerous mechanism. The drug acts as a super-agonist. It binds and opens the channel, causing a massive initial muscle twitch (fasciculation). But unlike ACh, the drug refuses to let go. It locks the channel open. The muscle membrane becomes utterly exhausted (depolarized block / Phase I block) and physically cannot fire again until the drug washes away.
Example: Succinylcholine. It provides ultra-fast, profound paralysis for emergency intubation.
V. The Cholinergic Receptors: Muscarinic (M)
The second family is named after Muscarine, a toxin extracted from the poisonous fly agaric mushroom (Amanita muscaria). These are responsible for the classic "Parasympathetic" (Rest & Digest) organ responses.
Unlike Nicotinic receptors, Muscarinic receptors are Metabotropic (G-Protein Coupled Receptors). They do not have built-in ion channels. Instead, they snake through the membrane 7 times and rely on internal G-proteins to alter cellular chemistry. There are 5 subtypes (M1 to M5), all found in the CNS, but heavily distributed in specific peripheral organs.
| Subtype | G-Protein Pathway | Primary Locations | Clinical Effect of Stimulation |
|---|---|---|---|
| M1 (Neural/Enteric) | Gq (Excitatory) | CNS, Enteric Nervous System, Gastric Parietal Cells | CNS excitation, massive increase in Gastric Acid secretion. |
| M2 (Cardiac) | Gi (Inhibitory) | Heart (SA node, AV node, Atria), Presynaptic terminals | Cardiac Inhibition: Severe decrease in heart rate (Bradycardia) and conduction velocity. |
| M3 (Glandular/Smooth Muscle) | Gq (Excitatory) | Exocrine glands (saliva, sweat, tears), Visceral Smooth Muscle (gut, bladder, bronchi), Blood vessels (endothelium) | The Workhorse: Massive glandular secretion, powerful contraction of visceral smooth muscle (causes bronchoconstriction and urination). *Promotes Vasodilation via Nitric Oxide (NO) release from endothelium. |
| M4 (Neural) | Gi (Inhibitory) | Central Nervous System | Neuronal inhibition. |
| M5 (Neural) | Gq (Excitatory) | Central Nervous System | CNS excitation. |
Deeper: Mechanisms of Muscarinic Signal Transduction
You must understand how the G-proteins actually force these cellular changes:
- The Excitatory Pathway (M1, M3, M5 via Gq):
Activation forces the Gq protein to activate an enzyme called Phospholipase C (PLC). PLC hacks a membrane lipid into two highly potent second messengers: IP3 (Inositol 1,4,5-trisphosphate) and DAG (Diacylglycerol). IP3 rips open calcium vaults inside the cell, causing a massive increase in intracellular Ca2+. This calcium instantly triggers smooth muscle contraction (e.g., gut cramping) and glandular secretion (e.g., sweating). DAG activates Protein Kinase C to further amplify the signal. - The Inhibitory Pathway (M2, M4 via Gi):
Activation forces the Gi protein to actively inhibit Adenylyl Cyclase, violently dropping cellular cAMP levels. Simultaneously, it pushes open Potassium (K+) channels. As K+ leaks out of the cell, the cell loses positive charge, becoming severely hyperpolarized (Slow IPSP). This makes the cell incredibly difficult to fire, which is exactly why M2 stimulation puts the brakes on the heart rate.
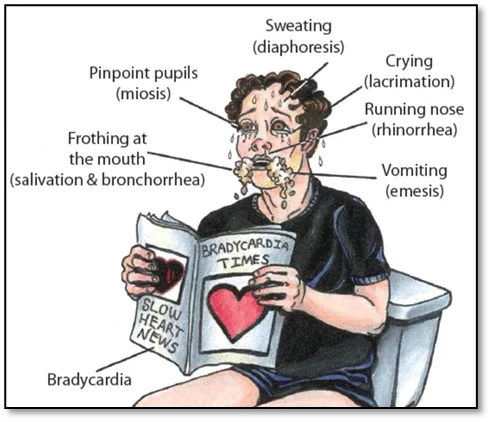
VI. Clinical Manifestations of Excessive Cholinergic Effects (Toxicity)
If a patient overdoses on a direct cholinergic agonist (like Pilocarpine) or an indirect agonist (like an Organophosphate pesticide/Sarin gas), they experience a terrifying, full-body physiological crisis. Every Muscarinic receptor fires at maximum capacity.
This is easily memorized via two classic, highly testable mnemonics: DUMBELS and the expanded BAG the PUDDLES.
- D - Defecation: Severe diarrhea (M3 gut hypermotility).
- U - Urination: Incontinence (M3 forces the detrusor muscle to squeeze).
- M - Miosis: Pinpoint pupils (M3 forces the sphincter pupillae to cramp).
- B - Bradycardia & Bronchospasm: The heart nearly stops (M2) and the lungs clamp shut (M3).
- E - Emesis: Vomiting.
- L - Lacrimation: Continuous crying/tears.
- S - Salivation & Sweating: Frothing at the mouth and dripping with sweat.
- B - Bronchoconstriction
- A - Apnea (Failure of the respiratory center)
- G - Graying/Dimming of vision
- P - Pupillary constriction (Miosis)
- U - Urination
- D - Diaphoresis (Massive sweating)
- D - Defecation
- L - Lacrimation
- E - Emesis
- S - Seizures (Due to massive CNS overstimulation).
*The ultimate cause of death in cholinergic crisis is respiratory failure (drowning in bronchial secretions while the airways are cramped shut).
VII. Effects of Muscarinic Antagonists (Anticholinergics)
To reverse a cholinergic crisis, or to treat specific diseases, we administer Muscarinic Antagonists. The prototype drug is Atropine (derived from the Deadly Nightshade plant, Atropa belladonna). By blocking M receptors, you strip away the parasympathetic "brakes," leaving the sympathetic nervous system unopposed.
The effects of an Anticholinergic overdose are legendary and captured in the most famous medical rhyme:
"Dry as a bone, blind as a bat, red as a beet, mad as a hatter, and hot as a hare."
- Dry as a bone: Complete blockade of M3 receptors causes a cessation of sweating, salivation, and lacrimation. The mouth feels like sandpaper.
- Blind as a bat: Blockade in the eye causes massive pupil dilation (Mydriasis) because the constrictor muscle is paralyzed. It also paralyzes the ciliary muscle (Cycloplegia), leading to a complete loss of visual focus and intense photophobia (sensitivity to light).
- Red as a beet: Because the body can no longer sweat to cool down, it attempts to radiate heat by undergoing reflex peripheral (cutaneous) vasodilation, making the skin flushed and bright red.
- Mad as a hatter: Severe CNS penetration of the drug leads to central muscarinic blockade, causing intense agitation, hallucinations, delirium, and eventually coma.
- Hot as a hare: The lack of sweating causes body temperature to spike dangerously (Hyperthermia), which is especially lethal in young children.
Other Critical Anticholinergic Effects:
- Tachycardia: Blocking the M2 "brakes" on the heart allows the resting heart rate to surge. (Atropine is used in emergencies to treat severe bradycardia).
- Bronchodilation: Relaxing the airways. (Drugs like Ipratropium are used in asthma and COPD inhalers to keep airways open).
- GI and Bladder Atony: The gut stops moving (causing severe constipation) and the bladder goes flaccid (causing urinary retention). (Drugs like Oxybutynin are used to treat an overactive, leaky bladder).
VIII. References and Recommended Reading
- Katzung, B. G., & Trevor, A. J. (2020). Basic & Clinical Pharmacology (15th ed.). McGraw-Hill Education. (Deep-dive into receptor pharmacology and specific drug actions).
- Brunton, L. L., Hilal-Dandan, R., & Knollmann, B. C. (2017). Goodman & Gilman's: The Pharmacological Basis of Therapeutics (13th ed.). McGraw-Hill. (Gold standard text for the molecular biochemistry of Acetylcholinesterase and G-protein signaling).
- Harvey, R. A., Clark, M. A., Finkel, R., Rey, J. A., & Whalen, K. (2011). Lippincott's Illustrated Reviews: Pharmacology (5th ed.). Lippincott Williams & Wilkins. (Excellent visual summaries of DUMBELS and Anticholinergic toxidromes).