
Genitourinary symptoms in palliative care are intensely private and deeply distressing. Loss of bladder control, painful urination, or blood in the urine strips patients of dignity and can cause social isolation. Many patients are too embarrassed to mention these symptoms — you must ask proactively.
Urinary symptoms are rarely just "urinary problems." They often signal spinal cord compression, advancing tumour, infection, or medication side effects. Always assess the underlying cause, not just the symptom. Physiological Context: The bladder is controlled by a delicate balance of sacral parasympathetics for emptying, and thoracolumbar sympathetics for storing. Any central or peripheral nerve lesion disrupting this balance manifests as urinary dysfunction before severe motor loss occurs.
Urinary retention is the inability to empty the bladder completely. It may be:
- Acute: sudden, painful, complete inability to pass urine. (The detrusor muscle is acutely overstretched, leading to severe visceral pain).
- Chronic: gradual, painless, with overflow incontinence. (The bladder slowly habituates to large volumes, losing its stretch-receptor sensitivity).
In palliative care, acute retention is a medical emergency — the bladder can rupture, and the patient suffers severe pain and distress.
| Cause | Explanation | Reversible? |
|---|---|---|
| Drug-induced | Anticholinergics (hyoscine, atropine), tricyclic antidepressants (amitriptyline), opioids. (Mechanism: Anticholinergics block acetylcholine at the muscarinic receptors on the detrusor muscle, preventing bladder contraction. Opioids increase urinary sphincter tone). | Usually yes — temporary, resolves when drug reduced/stopped. |
| Neurological | Spinal cord compression, cauda equina syndrome, diabetic neuropathy. | Sometimes — urgent treatment needed. |
| Faecal impaction | Hard stool in rectum physically compresses the bladder neck and urethra. | Yes — disimpact and establish bowel regimen. |
| Prostatic carcinoma | Tumour mechanically obstructs the bladder neck/prostatic urethra. | Partially — catheterisation, radiotherapy, hormones. |
| Pelvic tumours | Cervical, rectal, vaginal tumours extrinsically compress the urethra. | Partially — radiotherapy, catheterisation. |
| Urethral stricture | Scarring from previous infection or instrumentation. | Sometimes — dilatation or stenting. |
- Drugs
- Neurological (spinal cord)
- Faecal impaction
- Prostate cancer
- Pelvic tumours
- Urethral stricture
| Sign / Symptom | What It Means |
|---|---|
| Suprapubic pain and distension | Bladder is full and stretched — acute retention. |
| Restlessness and agitation | Especially in confused or non-verbal patients — may be their only way to express pain. |
| Palpable bladder | Rises from pelvis, dull to percussion, may reach umbilicus. |
| Overflow incontinence | Small, frequent leaks of urine around a full bladder — chronic retention. |
| Reduced or absent urine output | Despite normal fluid intake. |
| Post-void residual | If catheterised, large volume of urine drained (>500 ml suggests retention). |
In a confused patient who suddenly becomes agitated, always check for urinary retention before assuming delirium. A full bladder is agonizingly painful and easily treated. Do not sedate an agitated patient until you have palpated their suprapubic region!
| No. | Action | Details & Expansion / Rationale |
|---|---|---|
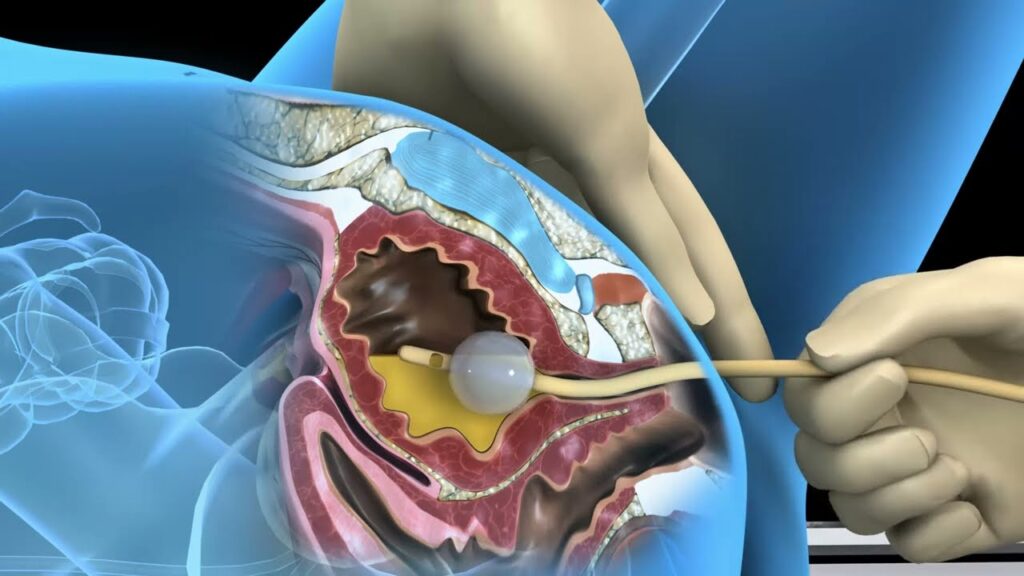
| 1 | Catheterise the patient | This is the first and most important step. |
| 2 | Use a Foley catheter | 14–16 French for adults; silicone if long-term. (Silicone reduces encrustation and tissue irritation compared to latex). |
| 3 | Drain bladder slowly | If >1000 ml, drain in stages (200–300 ml every 15 minutes) to prevent bladder collapse and haematuria. |
| 4 | Secure catheter | To inner thigh to prevent traction and urethral trauma. (Traction can cause pressure necrosis of the urethral meatus). |
| 5 | Monitor urine output | Document volume, colour, clarity. Watch for Post-Obstructive Diuresis (excessive urine output following relief of chronic obstruction leading to dehydration). |
| Cause | Treatment |
|---|---|
| Drug-induced | Review and reduce/stop offending drug (anticholinergics, TCAs, opioids). |
| Faecal impaction | Manual disimpaction; laxatives; regular bowel regimen. |
| Prostatic carcinoma | Radiotherapy; hormonal therapy (e.g., goserelin); alpha-blockers (e.g., tamsulosin) if available. (Alpha-blockers relax the smooth muscle of the bladder neck). |
| Spinal cord compression | Urgent dexamethasone 16 mg; radiotherapy; neurosurgical referral. (Dexamethasone profoundly reduces tumor edema compressing the cord). |
| Pelvic tumours | Radiotherapy; chemotherapy; consider suprapubic catheter if urethral obstruction is complete. |
- Use Foley catheters: Self-retaining with balloon; prevents displacement.
- Avoid inflating/deflating the bulb repeatedly: Damages the balloon valve; increases infection risk.
- Avoid inserting different sizes repeatedly: Traumatises the urethra; causes stricture formation.
- Bladder washouts: Use chlorhexidine 0.05% daily for infection prevention; weekly for maintenance. Use saline for removing debris, deposits, and clots.
- Train carers: Teach family to perform bladder washouts at home using boiled, cooled water.
- Pre-medication for anxious patients: Oral or rectal diazepam 2–5 mg or morphine 5 mg 30 minutes before catheterisation to relax the pelvic floor sphincter muscles.
When draining a very full bladder (>1000 ml), never drain it all at once. Rapid decompression causes a sudden drop in intravesical pressure, leading to tearing of the engorged submucosal blood vessels (causing severe haematuria) and potentially triggering vagally-mediated hypotension. Drain in stages over 30–60 minutes.
Dysuria is pain, burning, or discomfort during urination. In palliative care, it is often severe and distressing, especially when combined with urinary retention or incontinence.
- Urinary tract infection (UTI): Most common cause; especially in catheterised patients and women.
- Bladder or prostatic carcinoma: Tumour invades bladder mucosa or obstructs outflow, exposing sensory nerve endings to acidic urine.
- Calculi (stones): Sharp edges physically abrade, irritate and obstruct the mucosal lining.
- Retained blood clots: Post-surgery, post-biopsy, or from bleeding tumour. Clots act as foreign bodies causing painful bladder spasms.
- Infiltration by adjacent tumours: Rectal, vaginal, or cervical cancer growing directly into the bladder wall.
- Radiation cystitis: Late effect of pelvic radiotherapy — bladder lining is inflamed due to obliterative endarteritis (blood vessel scarring leading to chronic mucosal ischemia).
- Chemical irritation: From certain drugs (e.g., cyclophosphamide causing hemorrhagic cystitis) or highly concentrated urine.
| Question | Purpose & Clinical Logic |
|---|---|
| "Where is the pain?" | Urethral (at the start of urination) vs. suprapubic (during/after, indicating bladder spasm) vs. flank (kidneys, indicating pyelonephritis/obstruction). |
| "Is there blood in the urine?" | Suggests tumour, stones, or severe infection. |
| "Any fever or chills?" | Suggests systemic infection (UTI progressing to pyelonephritis or urosepsis). |
| "Are you passing clots?" | Suggests active bleeding source in bladder or upper tract. |
| "Is the pain constant or only on urination?" | Constant = invasive tumour involving pelvic nerves; On urination = UTI, stones, clots irritating the mucosa during contraction. |
- Most causes of dysuria: Catheterise to relieve obstruction, allow bladder washouts, and manage incontinence.
- UTI without retention: May not need catheter — treat infection and monitor. (Catheters introduce *more* bacteria, so avoid if bladder is emptying normally).
- Bladder carcinoma with pain: Catheter allows drainage, washouts, and instillation of local medications.
| Drug | Dose | Indication |
|---|---|---|
| Ibuprofen | 400 mg four times daily | Generalised bladder pain from inflammation. (Prostaglandin inhibitor. Inflammation drives bladder spasms, NSAIDs break this cycle). |
| Opioids | Morphine as per WHO ladder | Severe pain — do not withhold strong analgesia in palliative settings. |
| Topical lignocaine gel | Instilled into urethra before catheterisation | Local anaesthesia for procedure. Also physically lubricates to prevent micro-tears. |
Bladder pain from carcinoma is often severe and constant. Do not hesitate to escalate to strong opioids. The patient deserves comfort. Bladder spasms may also respond to antispasmodics (like hyoscine butylbromide) in addition to analgesia.
- Washouts: Chlorhexidine 0.05% (Daily for infection prevention), Saline (As needed to remove debris, deposits, clots), Boiled/cooled water (As needed for home washouts by trained carers).
- Permanent Catheterisation Indications: Recurrent retention (Patient cannot empty bladder reliably), Severe intractable dysuria (Catheter bypasses painful urethra), Incontinence causing skin breakdown (Protects skin, reduces nursing burden), Terminal phase (Comfort and dignity for patient and family).
| Type | Mechanism | Common in Palliative Care? |
|---|---|---|
| Stress incontinence | Leakage on coughing, sneezing, laughing — due to weak pelvic floor muscles. | Less common. |
| Urge incontinence | Sudden intense urge, cannot reach toilet in time — due to overactive bladder (detrusor instability). | Moderate. |
| Overflow incontinence | Bladder overfills and passively leaks — chronic retention. (The pressure inside exceeds sphincter resistance). | Very common. |
| Functional incontinence | Cannot reach toilet due to immobility or confusion (urinary tract functions normally, but physical/cognitive barriers exist). | Very common. |
| Reflex incontinence | Spinal cord injury above S2 — bladder empties automatically without sensation. | Moderate. |
- Causes: Urinary retention with overflow (Most common), Neurological disease (Cord compression, stroke, dementia), Weak pelvic floor, Infection (UTI causes urgency/frequency), Medications (Diuretics, sedatives, muscle relaxants), Immobility, Confusion.
- Assessment Actions:
- Check for retention (Palpate bladder; check post-void residual if catheterised).
- Bladder diary (Record frequency, volume, leaks, triggers).
- Urine dipstick / microscopy (Rule out infection).
- Medication review (Are they on loop diuretics before bed?).
- Mobility assessment (Can the patient physically reach the toilet?).
- A. Treat Underlying Cause: Retention = Catheterise; UTI = Antibiotics (e.g., Septrin, nitrofurantoin); Faecal impaction = Disimpact/bowel regimen; Medication-induced = Review and adjust.
- B. Non-Pharmacological: Regular toileting schedule (Every 2–3 hours), Bedside commode/urinal, Incontinence pads (Change frequently to prevent moisture-associated skin damage), Barrier cream (Zinc oxide or aqueous cream to protect perineal skin from acidic urine burns), Fluid management (Reduce evening fluids).
- C. Pharmacological:
- Oxybutynin (2.5–5 mg BD–TDS): For Urge incontinence. It is an anticholinergic that stops detrusor spasms.
- Tolterodine (2 mg BD): Alternative to oxybutynin with fewer systemic side effects (like dry mouth).
- Desmopressin (Nasal spray/tablet): For Nocturia. It is an ADH analogue that directly reduces nighttime urine production by the kidneys.
Anticholinergics (like oxybutynin) relax the bladder muscle. If a patient has an undiagnosed outlet obstruction (like an enlarged prostate) and you give them oxybutynin, you will completely paralyse the bladder and cause acute urinary retention. Always ensure the bladder empties adequately before starting these drugs!
Haematuria is the presence of blood in the urine. It ranges from microscopic (only seen on dipstick) to gross (visible to the naked eye) to massive (with clots causing retention).
Key Statistic: Haematuria occurs in approximately 10% of patients nearing the end of life.
| Cause | Explanation |
|---|---|
| Bladder carcinoma | Most common — tumour is highly friable, neovascularized, and bleeds easily. |
| Prostatic carcinoma | Tumour invades the delicate mucosa of the urethra or bladder neck. |
| Radiation cystitis | Late effect of pelvic radiotherapy — radiation damages local tissue causing fragile, abnormal blood vessels (telangiectasias) that rupture easily. |
| UTI | Severe inflammation breaks down mucosal integrity causing bleeding. |
| Calculi | Stones physically abrade and cut the bladder or urethral lining. |
| Coagulopathy | Low platelets, anticoagulants (Warfarin/Heparin), liver failure (decreased clotting factors). |
| Trauma | Traumatic catheterisation, harsh bladder washouts. |
- Amount: Streaks? Frank blood? Clots?
- Timing: At start of urination (indicates urethral source), throughout (indicates bladder/kidney source), or at end (indicates prostatic source).
- Associated symptoms: Dysuria, frequency, fever, pain, clot retention.
- Medications & Coagulation: Anticoagulants? Aspirin? Platelet count, INR if available.
- Reassurance: Explain that small amounts are common in advanced disease.
- Increase fluid intake: Dilutes urine, prevents clot formation, and reduces mucosal irritation.
- Monitor & Review: Watch for increase in bleeding or clot formation. Stop anticoagulants if medically safe.
- Catheterise & Washout: Use a Three-way catheter if available (allows continuous normal saline irrigation to flush out clots and prevent retention).
- Silver nitrate solution: Bladder washout to chemically cauterize bleeding vessels.
- Tranexamic acid: 1 g IV or oral. (Mechanism: An antifibrinolytic drug. It competitively inhibits plasminogen activation, preventing the breakdown of fibrin, thus stabilizing the clot over the bleeding tumour).
- Crushed tranexamic acid: 500 mg applied directly to the bleeding wound (if bleeding from an external exophytic tumour).
- Radiotherapy: Palliative external beam radiation effectively shrinks bleeding tumours and stops hemorrhage.
- Action: Call for emergency help (life-threatening). Large-bore IV access for fluids/blood transfusion. Monitor vital signs for Shock (Tachycardia, hypotension).
- Intervention: Continuous saline irrigation via three-way catheter. Silver nitrate instillation. Embolisation (interventional radiology to block the specific bleeding vessel). Surgery is rarely appropriate in palliative care.
If a patient with bladder cancer has haematuria with clots and suddenly cannot pass urine, accompanied by severe pain, this is clot retention — a surgical emergency. Catheterise immediately (using a large bore catheter, e.g., 20-22 Fr) and irrigate aggressively with a 50cc Toomey syringe to manually suck out the obstructing clots.
| Symptom | Key Feature | Most Common Cause | First-Line Management | Nursing Priority | Red Flag |
|---|---|---|---|---|---|
| Urinary Retention | Painful, distended bladder; no urine passed | Drugs, faecal impaction, prostate CA, cord compression | Catheterise immediately | Drain slowly if >1000 ml; check for spinal cord compression | Acute retention = emergency |
| Dysuria | Burning pain on urination | UTI, bladder carcinoma, stones | Catheterise; analgesia (ibuprofen → opioids); washouts | Pre-medicate before catheterisation; do not withhold strong analgesia | Haematuria + dysuria = tumour or stones |
| Urinary Incontinence | Involuntary urine loss | Overflow from retention, immobility, confusion, UTI | Treat cause; regular toileting; pads; barrier cream | Check for retention first; protect skin | Overflow incontinence = chronic retention |
| Haematuria (mild) | Blood-streaked urine | Bladder cancer, UTI, radiation cystitis | Reassurance; fluids; monitor; review anticoagulants | Monitor for worsening; dark containers | Increasing frequency or amount |
| Haematuria (severe) | Frank blood, clots | Bladder cancer, coagulopathy | Catheterise; irrigation; tranexamic acid; silver nitrate | Clot retention = emergency; irrigate gently | Shock (tachycardia, hypotension) |
- Drugs (Anticholinergics, TCAs, opioids)
- Neurological (Spinal cord compression)
- Faecal impaction (Rectum compresses bladder)
- Prostate / Pelvic tumours (Obstruct bladder neck)
- Foley catheter (Use self-retaining type)
- Avoid repeated inflation/deflation (Damages balloon)
- Slow drainage (If bladder very full)
- Train carers (For home bladder washouts)
- Catheterise (Relieve retention, allow irrigation)
- Assess amount and cause (Document; investigate if new onset)
- Tranexamic acid (Promote clotting via antifibrinolysis)
- Continuous irrigation (For clots)
- Haemostasis (Silver nitrate, radiotherapy, embolisation)
Q1: A patient on morphine and hyoscine suddenly becomes agitated and restless. On examination, the bladder is palpable 3 finger-breadths above the pubic symphysis. What is the likely diagnosis, and what is your first action?
Answer: Acute urinary retention caused by the anticholinergic (hyoscine) and opioid (morphine) effects. First action: Catheterise immediately to relieve the retention. Then review medications — consider reducing or stopping the anticholinergic.
Q2: A patient with known prostate cancer has not passed urine for 12 hours and complains of severe lower abdominal pain. What are your management steps?
Answer: 1) Catheterise immediately (Foley). 2) Drain slowly if >1000 ml. 3) Treat underlying cause (radiotherapy/hormonal therapy). 4) Review meds. 5) Monitor output.
Q3: A patient with bladder cancer has painful urination and visible blood. What analgesic would you start with, and when would you escalate?
Answer: Start with ibuprofen 400 mg QDS (prostaglandin inhibitor, reduces bladder inflammation). If insufficient, do not hesitate to escalate to opioids (morphine) — bladder cancer pain is often severe and requires strong analgesia.
Q4: A dying patient has blood-streaked urine. The family is very distressed. What do you tell them?
Answer: Reassure them that mild haematuria is common in advanced disease, especially with bladder tumours or catheters. Explain you are monitoring the amount, ensuring comfort, and will intervene if bleeding increases. Nursing action: Use dark-coloured containers to reduce visual distress.
Q5: Why should you drain a very full bladder slowly rather than all at once?
Answer: Rapid decompression causes: 1) Bladder mucosal damage and haematuria (tearing of engorged vessels). 2) Hypotension due to sudden shift of fluid. 3) Atrial stretch reflex causing cardiac arrhythmias. Drain in 200–300 ml stages every 15 minutes.
Q6: A patient with a catheter has not passed urine for 4 hours and complains of suprapubic pain. What do you check first?
Answer: Check catheter patency first — the catheter may be blocked by a blood clot, kink, or sediment. Flush gently with saline. If blocked and cannot be cleared, replace it. Never assume retention without checking the catheter first.
- Urinary retention is an emergency — catheterise immediately; do not wait for tests.
- Always check for retention in a confused or agitated patient — it may be the only symptom.
- Drain a very full bladder slowly — in stages to prevent haematuria and hypotension.
- Drug-induced retention (anticholinergics, opioids, TCAs) is usually reversible — review medications.
- Spinal cord compression causes retention with neurological signs — urgent dexamethasone and referral.
- Dysuria from bladder cancer requires strong analgesia — do not withhold opioids.
- Bladder washouts with chlorhexidine prevent infection; saline clears debris and clots.
- Train family carers to perform home bladder washouts with boiled, cooled water.
- Pre-medicate with diazepam or morphine before catheterisation for anxious patients.
- Haematuria in 10% of terminal patients — reassure for mild cases; act fast for clots or shock.
- Silver nitrate bladder washouts reduce bleeding from radiation cystitis or fragile tumours.
- Dark containers reduce panic — a simple but powerful nursing intervention.
- Incontinence is not just "old age" — always check for retention, infection, and faecal impaction.
- Skin protection is essential in incontinence — barrier cream, regular changing, pads.
In genitourinary care, the catheter is both a medical device and a symbol of lost dignity. Insert it with gentleness, explain every step, secure it discreetly, and care for it meticulously. A well-managed catheter restores comfort and allows the patient to focus on living, not on their bladder. Your skill with a catheter is your compassion made visible.
- Watson, M., Lucas, C., Hoy, A., & Back, I. (2009). Oxford Handbook of Palliative Care. Oxford University Press.
- Ferrell, B. R., & Coyle, N. (2010). Oxford Textbook of Palliative Nursing. Oxford University Press.
- World Health Organization (WHO) Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents.
- Clinical guidelines on genitourinary symptom management in end-of-life care.
Quick Quiz
Genitourinary Symptoms Quiz
Palliative Care - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Genitourinary Symptoms Quiz
Palliative Care
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.