
Acids, Bases, pH, and Biological Buffer Systems
By the conclusion of this exhaustive master guide, you will be deeply conversant with:
- Acids, Bases, and pH: The rigorous chemical definitions of acids and bases (proton donors and acceptors) and their behavior in aqueous physiological solutions.
- The pH Scale: The mathematical (logarithmic) foundation of pH and its immense clinical significance in human physiology.
- Biological Buffers: The chemical architecture of buffer systems (weak acids and conjugate bases) and why they are absolutely crucial in living systems.
- The Three-Tiered Defense Strategy: How chemical buffers, the respiratory system, and the renal system collaborate to maintain strict acid-base homeostasis.
- Clinical Imperatives: The profound sensitivity of biochemical reactions to pH, interpreting Acidosis vs. Alkalosis, and understanding the pathophysiology of severe acid-base derangements (e.g., Diabetic Ketoacidosis, COPD, Renal Failure).
I. The Foundation: Acids, Bases, and the Dynamic Cellular Environment
The environment within and around our cells is not a static, motionless void; it is a highly dynamic, volatile "chemical soup" where countless millions of enzymatic and metabolic reactions occur simultaneously every fraction of a second. Just as a baker must meticulously and precisely control the temperature of an oven to ensure bread rises without burning, the "chemical temperature" of our biological systems—specifically its acidity or basicity—must be meticulously maintained within an incredibly narrow, unforgiving range.
This exquisite control, measured by pH, is paramount for the continuation of life. Even microscopic, seemingly minor deviations can lead to catastrophic, cascading clinical consequences. The delicate tertiary and quaternary folding structures of proteins, the active sites of enzymes, and the electrical gradients of nerve cell membranes are exquisitely sensitive to pH changes. This relentless maintenance of a stable internal pH is the absolute cornerstone of physiological homeostasis.
II. The Chemistry of Acidity and Basicity: It's All About the Proton (H⁺)
At the absolute heart of acidity and basicity lies one tiny, yet profoundly powerful, subatomic particle: the hydrogen ion (H⁺). Because a standard hydrogen atom consists of just one proton and one electron, stripping away its electron leaves behind a naked proton. Therefore, a hydrogen ion (H⁺) is essentially just a free-floating proton. The precise concentration of these free H⁺ ions in a biological solution is the ultimate, sole determinant of whether that solution is acidic, neutral, or basic (alkaline).
According to the Brønsted-Lowry definition, an acid is any substance that, when dissolved in an aqueous (water-based) solution, releases or donates hydrogen ions (H⁺), thereby forcefully increasing the concentration of free H⁺ in that solution.
- Strength: A strong acid dissociates almost 100% completely in water, releasing violently nearly all its H⁺ ions. A weak acid only partially dissociates, creating a gentle equilibrium.
- Strong Acid Example: Hydrochloric Acid (HCl) in your stomach. It is crucial for digestion and sterilizing ingested food. It undergoes complete dissociation:
HCl(aq) → H⁺(aq) + Cl⁻(aq) - Weak Acid Example 1: Carbonic Acid (H₂CO₃). A crucial weak acid in your blood. It partially dissociates:
H₂CO₃(aq) ⇌ H⁺(aq) + HCO₃⁻(aq)(The double arrow ⇌ indicates reversibility). - Extra Example (Metabolic): Lactic Acid. Produced during anaerobic respiration (e.g., sprinting, or in septic shock). It rapidly dissociates, threatening to drop blood pH aggressively.
A base (or alkali) is any substance that, when dissolved in an aqueous solution, decreases the concentration of H⁺ ions. It does this either by aggressively "accepting/binding" free H⁺ ions out of the fluid, or by releasing hydroxide ions (OH⁻) which then hunt down and neutralize H⁺.
- Strength: A strong base dissociates almost completely. A weak base only partially accepts H⁺ or releases OH⁻ ions.
- Strong Base Example: Sodium Hydroxide (NaOH). It dissociates completely:
NaOH(aq) → Na⁺(aq) + OH⁻(aq)
The released OH⁻ then rapidly combines with H⁺ to neutralize it into harmless water:OH⁻ + H⁺ → H₂O(l). - Weak Base Example 1: Bicarbonate (HCO₃⁻). The absolute most important weak base in human blood plasma. It readily accepts a free H⁺ ion to "soak up" excess acid:
HCO₃⁻(aq) + H⁺(aq) ⇌ H₂CO₃(aq) - Extra Example (Metabolic): Ammonia (NH₃). Produced by protein breakdown in the liver. It accepts a proton to become the Ammonium ion (NH₄⁺), which the kidneys then excrete into the urine.
The Crucial Importance of "Aqueous Solution"
The definition of acids and bases in medical biochemistry relies entirely on their behavior in aqueous solutions (where water is the universal solvent). Water itself is not entirely inert; it can slightly, spontaneously dissociate: H₂O(l) ⇌ H⁺(aq) + OH⁻(aq). In pure, distilled water, the concentrations of H⁺ and OH⁻ are perfectly equal, making it mathematically neutral. Acids disturb this delicate balance by increasing H⁺, and bases disturb it by decreasing H⁺.
III. The pH Scale: A Precise and Powerful Ruler for Acidity
While discussing "hydrogen ion concentration" (denoted as [H⁺]) is chemically precise, it is medically cumbersome. Writing out concentrations like 0.00000004 moles/Liter in a fast-paced ICU is dangerous and prone to error. To simplify this, scientists developed the pH scale—a brilliant mathematical shorthand that transforms these unwieldy microscopic numbers into an easy-to-use, visible linear scale.
What Does pH Stand For?
pH literally translates to the "potential of Hydrogen" or the "power of Hydrogen." It is a numerical scale that rigorously quantifies the concentration of hydrogen ions (H⁺) in a solution.
The pH is defined mathematically as the negative base-10 logarithm of the hydrogen ion concentration (measured in moles per liter, M):
pH = −log₁₀[H⁺]
Why a logarithm? The log₁₀ function compresses massive variations in numbers into a small, manageable scale. Why the negative sign? Because H⁺ concentrations are tiny fractions (like 10⁻⁷), the negative sign flips the mathematical result into the positive, whole numbers we easily recognize on the standard scale.
The pH Scale Range and Interpretations (0 to 14)
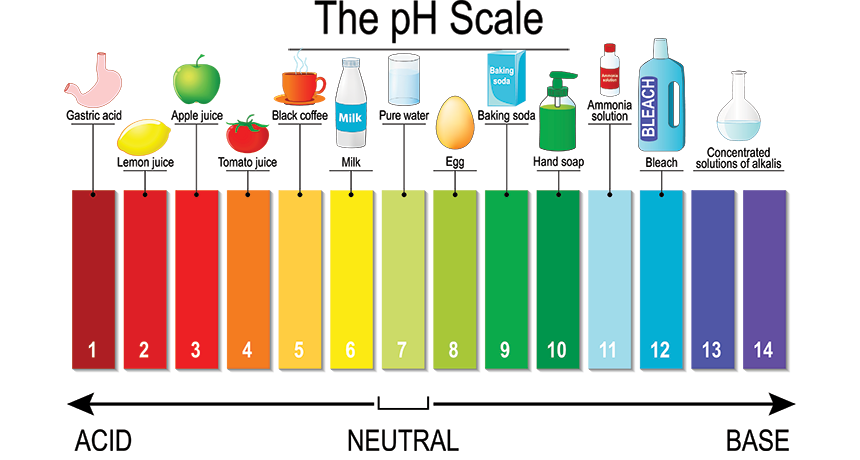
- Acidic (pH < 7): The lower the pH number, the exponentially higher the [H⁺] concentration.
Clinical/Real-World Examples: Gastric (Stomach) acid (pH 1.5 - 3.5), Lemon juice (pH 2.0), Vaginal secretions (pH 3.8 - 4.5), Urine (pH 6.0). - Neutral (pH = 7): The absolute concentration of H⁺ perfectly equals the concentration of OH⁻.
Clinical/Real-World Examples: Pure distilled water, human tears, cerebrospinal fluid (highly close to neutral). - Basic/Alkaline (pH > 7): The higher the pH number, the exponentially lower the [H⁺] concentration.
Clinical/Real-World Examples: Pancreatic juice (pH 8.0 - 8.3) to neutralize stomach acid, Baking soda, household ammonia (pH 11.0), Bleach (pH 13.0).
The Logarithmic Nature: A Crucial Detail for Healthcare Professionals
This is perhaps the single most important concept regarding the pH scale. It is logarithmic, NOT linear. This means that a change of exactly 1 pH unit represents a 10-fold (ten times) change in the actual, physical concentration of H⁺ ions.
Applying the Mathematical Principle:
- A solution with a pH of 5 is exactly 10 times more acidic than a solution with a pH of 6.
- A solution with a pH of 4 is exactly 100 times more acidic (10 × 10) than a solution with a pH of 6.
- A solution with a pH of 3 is exactly 1,000 times more acidic (10 × 10 × 10) than a solution with a pH of 6.
Biological and Clinical Significance: Small pH Changes, MASSIVE Impact
Because of this logarithmic nature, even a seemingly microscopic numerical change in pH (e.g., moving from 7.4 to 7.1) represents an enormous, life-threatening alteration in the actual concentration of H⁺ ions. This has profound implications for human physiology:
- Enzyme Function: Proteins and metabolic enzymes are exquisitely sensitive to pH. Even a change of 0.1 to 0.2 pH units alters the electrical charges on the amino acids, significantly decreasing enzyme activity. Extreme changes cause irreversible denaturation (unfolding and destruction) of the protein.
- Blood pH - A Tightrope Walk: The pH of human arterial blood is violently and tightly regulated between 7.35 and 7.45. A drop from 7.4 to 7.1 means the blood is more than twice as acidic; this is a critical medical emergency (severe acidosis) leading to cardiac arrest.
- Electrolyte Balance (Potassium Shifts): Changes in pH force cells to swap ions to survive. In severe Acidosis, cells absorb the excess H⁺ from the blood, but to maintain electrical neutrality, they must kick Potassium (K⁺) out into the bloodstream. This causes fatal Hyperkalemia, which triggers lethal cardiac arrhythmias.
- Oxygen Transport (The Bohr Effect): The affinity (grip strength) of hemoglobin for oxygen is directly altered by pH. Acidosis causes hemoglobin to lose its grip on oxygen (shifting the oxygen-dissociation curve to the right), which impairs overall oxygen uptake in the lungs.
- Central Nervous System (CNS) Function: Both severe extremes are neurotoxic. Acidosis severely depresses the CNS, leading to lethargy, confusion, coma, and respiratory failure. Alkalosis severely overstimulates the CNS and peripheral nerves, leading to muscle tetany, extreme nervousness, and fatal seizures.
IV. The Physiology of Buffers: The Body's Chemical "Shock Absorbers"
Our bodies are relentless, 24/7 biochemical factories, constantly generating massive amounts of acidic or basic byproducts (like lactic acid, sulfuric acid from protein breakdown, and carbon dioxide). If these volatile metabolic waste products were allowed to accumulate unchecked, the pH of our internal fluids would plummet instantly, and all life-sustaining reactions would halt. This catastrophic scenario is prevented entirely by ingenious, ubiquitous chemical systems known as Buffers.
What is a Buffer? The Analogy
A buffer is a highly specialized chemical system designed specifically to resist significant changes in pH when an external acid or a base is added to the solution. Think of buffers as the heavy-duty suspension system in an ambulance. When the ambulance hits a massive pothole (a sudden influx of metabolic acid), the suspension completely absorbs the kinetic impact, keeping the ride inside completely smooth and stable (keeping the pH stable). Without chemical buffers, every single metabolic acid load would send the human body into an immediate pH crisis.
The Chemical Architecture of a Buffer System
A functional buffer system is always composed of a specific pair of interacting molecules: a weak acid and its corresponding conjugate weak base. (Note: You cannot use strong acids like HCl as buffers because they do not reverse their reactions). This precise pairing allows the system to neutralize BOTH incoming excess acid and incoming excess base.
- When an Acid (H⁺) is Added: The weak base component instantly binds to the incoming, dangerous excess H⁺ ions, physically taking them out of the free solution, trapping them, and preventing a sharp drop in pH.
- When a Base (OH⁻) is Added: The weak acid component immediately sacrifices and releases its own stored H⁺ ions into the solution to replace the ones that were consumed by the base, preventing the pH from spiking upward.
Buffer Capacity: The Dangerous Limitations of the System
It is vital for healthcare professionals to understand that buffers are not infinite; they have a strict mathematical limitation known as Buffer Capacity. This refers to the total amount of acid or base a buffer can successfully neutralize before its components are entirely depleted and the pH shifts dramatically.
Once the buffer molecules are "used up," the buffer "breaks." This is exactly why severe metabolic conditions like Diabetic Ketoacidosis (DKA) are so rapidly life-threatening. The diabetic body produces so much acidic "ketone body" waste that the entire blood buffer system becomes completely exhausted. Once the buffer breaks, the blood pH plummets fatally.
V. The Three Primary Biological Buffer Systems
Now that we understand the critical importance of maintaining a stable pH, we will delve into the three specific, intricate buffer systems that allow the human body to achieve this remarkable feat. These systems are strategically located and exquisitely designed to work in absolute concert, forming an impenetrable defense network.
The Predominant Regulator of Extracellular Fluid (ECF)
This is arguably the absolute most significant buffer system in the blood plasma and interstitial fluid. Its sheer power stems from its massive abundance, the ease with which its components can be regulated, and its intimate physiological connections to BOTH the respiratory (lungs) and renal (kidneys) systems.
- Weak Acid Component: Carbonic Acid (H₂CO₃)
- Conjugate Weak Base Component: Bicarbonate Ion (HCO₃⁻)
- The Dynamic Equilibrium:
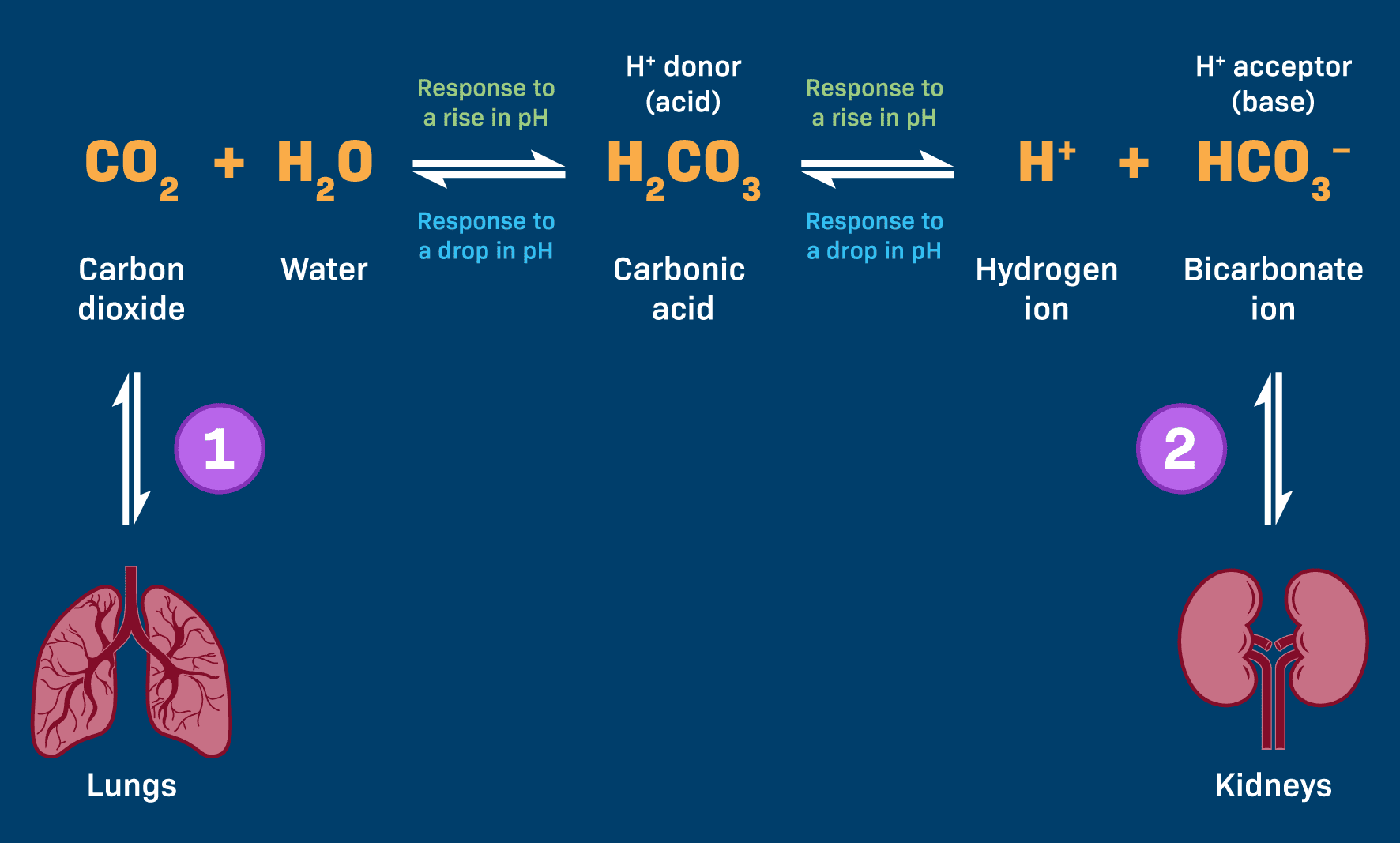
CO₂(g) + H₂O(l) ⇌ H₂CO₃(aq) ⇌ H⁺(aq) + HCO₃⁻(aq)
How it Counteracts pH Changes:
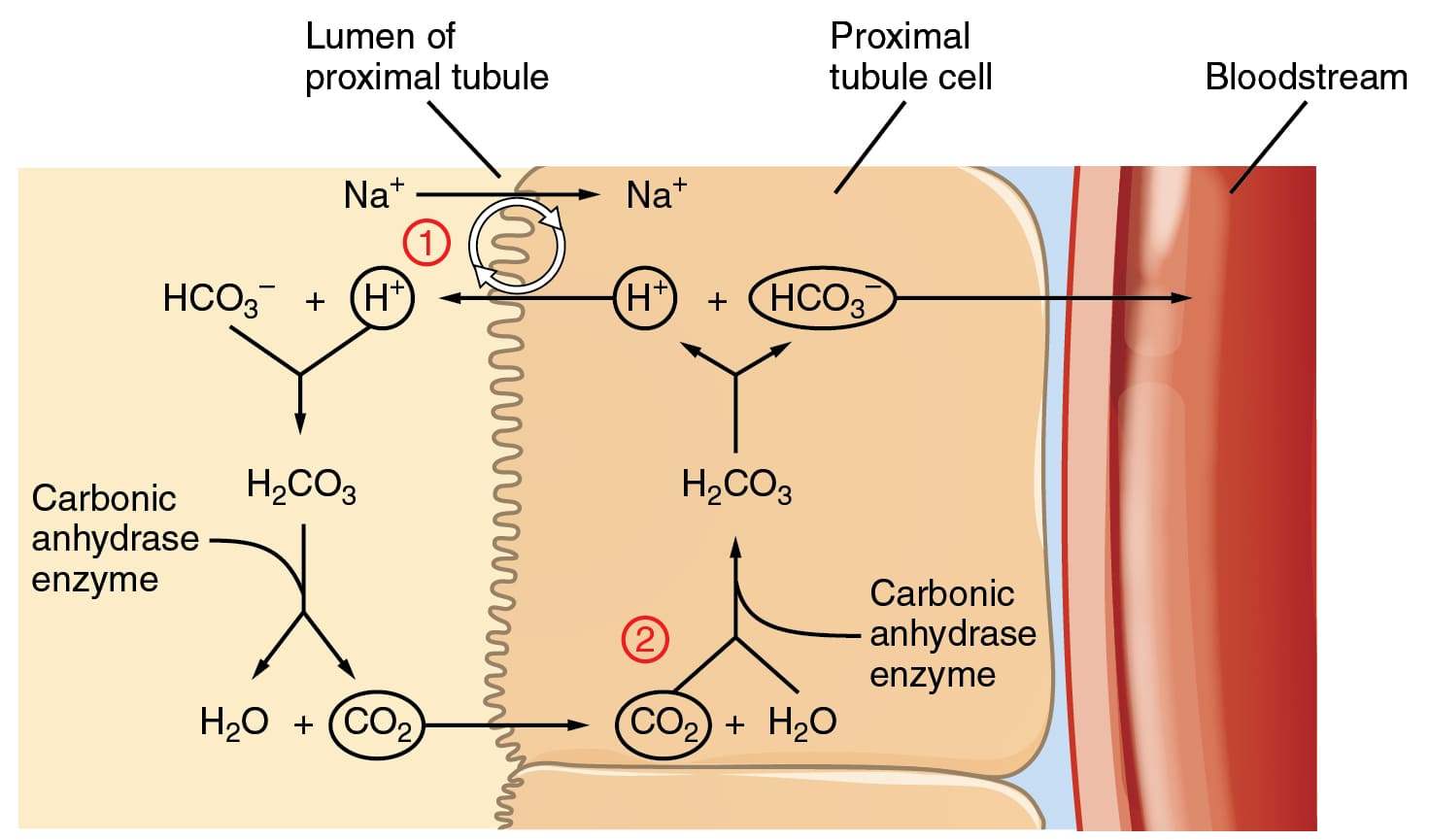
- If Blood Becomes Too ACIDIC (Excess H⁺): The abundant bicarbonate ions (HCO₃⁻) act as molecular proton acceptors, aggressively binding to the excess H⁺ to form carbonic acid (a much weaker, safer acid).
HCO₃⁻ + H⁺ → H₂CO₃
Respiratory Compensation: The H₂CO₃ is unstable and breaks down into CO₂ and Water. The lungs immediately hyperventilate (breathe rapidly) to "blow off" this excess CO₂, literally exhaling the acid out of the body! - If Blood Becomes Too BASIC (Deficit of H⁺): The carbonic acid (H₂CO₃) component dissociates, intentionally releasing its trapped H⁺ ions into the blood to replenish the dangerous deficit.
H₂CO₃ → H⁺ + HCO₃⁻
Renal Compensation: The kidneys will actively excrete the excess bicarbonate into the urine to stop the blood from becoming too alkaline.
2. The Phosphate Buffer System
The Guardian of Intracellular Fluid and Urine
While less quantitatively significant than the bicarbonate system in the blood plasma, the phosphate buffer system plays a vital, highly specialized role deep inside the cells (Intracellular Fluid) and within the kidney tubules (Urine).
- Weak Acid Component: Dihydrogen Phosphate (H₂PO₄⁻)
- Conjugate Weak Base Component: Monohydrogen Phosphate (HPO₄²⁻)
- The Dynamic Equilibrium:
H₂PO₄⁻ ⇌ H⁺ + HPO₄²⁻
Clinical Significance: Inside the cell, phosphate concentrations are extremely high (due to ATP and nucleic acids), providing a massive protective shield for cellular machinery. In the kidneys, the phosphate buffer system acts as "Titratable Acidity." It binds to the massive amounts of H⁺ pumped into the urine by the kidneys, allowing the body to excrete vast amounts of fatal acid without letting the urine pH drop low enough to physically burn and destroy the urinary tract tissue.
The Most Abundant Buffer System in the Body
Proteins are the most abundant macromolecules in the human body, accounting for an astonishing 75% of the body's total chemical buffering capacity. Their raw power comes from their abundance and the unique, amphoteric chemical groups in their amino acid building blocks.
The Components (Amino Acids): Proteins are zwitterions (they possess both positive and negative charges).
- Amino Groups (−NH₂): These act as basic groups. They can eagerly accept free H⁺ ions when the cellular environment becomes dangerously acidic.
−NH₂ + H⁺ ⇌ −NH₃⁺ - Carboxyl Groups (−COOH): These act as acidic groups. They can willingly donate their stored H⁺ ions when the environment becomes dangerously basic.
−COOH ⇌ −COO⁻ + H⁺
A single, massive protein molecule (like albumin in the plasma) contains hundreds of these reactive groups, allowing it to buffer massive swings over a very wide range of pH values.
VI. Deeper: CO₂ Transport, Hemoglobin, and The Chloride Shift
Let us break down the highly critical, multi-step process of carbon dioxide transport and pH buffering in the blood—an absolutely vital physiological concept for medical and nursing students. This mechanism illustrates precisely what happens in the deep body tissues and within a blood capillary, focusing on the miraculous interplay between the bicarbonate buffer system, the red blood cell, and Hemoglobin.
Step-by-Step Explanation of the "Hamburger Phenomenon"
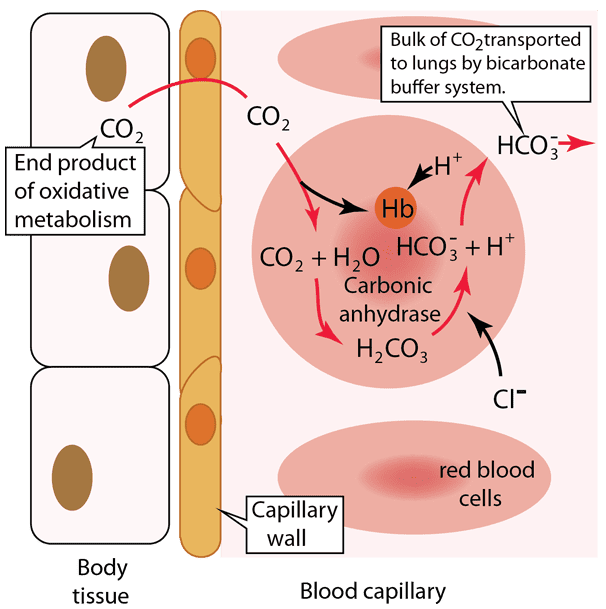
- Step 1: Carbon Dioxide Production in Body Tissues
Cellular respiration (generating ATP for survival) constantly produces carbon dioxide (CO₂) as a toxic metabolic waste product. This newly formed CO₂ quickly diffuses out of the tissue cells because its concentration is higher inside the cells than in the blood. It crosses the capillary wall and enters the blood plasma. - Step 2: Carbon Dioxide Enters the Red Blood Cell (Erythrocyte)
Once in the blood plasma, a massive portion (about 70-75%) of the CO₂ instantly diffuses directly inside the red blood cells. This safe, internal environment is where the magic of the bicarbonate buffer system largely happens. - Step 3: Formation of Carbonic Acid and Bicarbonate (The Role of Carbonic Anhydrase)
Inside the red blood cell, the incoming CO₂ immediately reacts with intracellular water (H₂O). This reaction is normally slow, but it is supercharged by the presence of a powerful, fast-acting enzyme called Carbonic Anhydrase (CA). Carbonic anhydrase rapidly catalyzes the chemical fusion of CO₂ and H₂O into carbonic acid (H₂CO₃). The H₂CO₃ is highly unstable and instantly dissociates (breaks down) into a dangerous hydrogen ion (H⁺) and a protective bicarbonate ion (HCO₃⁻).
Clinical Note: Certain diuretic drugs, like Acetazolamide, specifically target and paralyze this Carbonic Anhydrase enzyme to alter fluid and acid balance in the kidneys and eyes! - Step 4: Buffering of Hydrogen Ions by Hemoglobin (The Isohydric Shift)
The newly created hydrogen ions (H⁺) are highly acidic and lethal if left alone. This is where Hemoglobin (Hb), the protein responsible for oxygen transport, steps in as an exceptionally important protein buffer. Hemoglobin possesses special histidine amino acid residues that eagerly bind to these H⁺ ions, physically trapping them and preventing them from dropping the blood pH.
The Bohr/Haldane Interplay: Crucially, deoxygenated hemoglobin (found in the oxygen-starved deep tissues) has a much greater affinity for trapping H⁺ than oxygenated hemoglobin does. This guarantees that hemoglobin acts as a powerful buffer exactly where the acid is being generated! - Step 5: Bicarbonate Ion Transport into Plasma (The Chloride Shift)
As bicarbonate ions (HCO₃⁻) rapidly accumulate inside the red blood cell, they must be moved out into the blood plasma to travel to the lungs. They exit through a special membrane transporter (the Band 3 protein). However, if massive amounts of negative HCO₃⁻ left the cell, the electrical charge of the cell would collapse. To maintain strict electrical neutrality, as every negatively charged HCO₃⁻ ion moves OUT, one negatively charged Chloride ion (Cl⁻) is forced INTO the red blood cell. This famous, rapid exchange is known globally as the Chloride Shift (or Hamburger Phenomenon).
Summary of Reversal in the Lungs:
When these red blood cells finally travel through the venous system and reach the lungs, the entire process violently reverses. Oxygen floods in and binds to Hemoglobin. Hemoglobin then forcefully evicts the trapped H⁺ ions. The HCO₃⁻ rushes back into the red blood cell (pushing Chloride back out), recombines with the H⁺ to form H₂CO₃, which Carbonic Anhydrase then shatters back into H₂O and CO₂ gas. The CO₂ diffuses across the alveolar membrane and is exhaled into the atmosphere.
VII. The Three-Tiered Defense Strategy: Maintaining Homeostasis
These buffer systems do not operate in isolation; they collaborate in a highly synchronized, multi-tiered physiological defense strategy to prevent death by acidosis or alkalosis.
- First Line of Defense: Chemical Buffer Systems (Rapid & Immediate)
The bicarbonate, phosphate, and protein buffer systems floating in the blood and cells provide immediate, instantaneous buffering within milliseconds to seconds. They are always active, chemically neutralizing any sudden H⁺ excess or deficit. They "absorb the initial shock" and buy critical time for the massive physiological organs to boot up and respond. - Second Line of Defense: The Lungs (Intermediate)
The respiratory system acts as a rapid-response physiological buffer, responding within minutes to hours. Specialized chemoreceptors in the brainstem (Medulla) sense the falling pH and immediately command the lungs to adjust the rate and depth of ventilation:- Hyperventilation: Increased breathing rapidly blows off more CO₂ gas, effectively vacuuming carbonic acid directly out of the blood to increase pH and correct Acidosis.
- Hypoventilation: Decreased, shallow breathing purposely retains CO₂ gas, intentionally increasing carbonic acid to decrease the pH and correct Alkalosis.
- Third Line of Defense: The Kidneys (Long-Term & Ultimate Correction)
The renal system constitutes the most powerful, definitive, and precise regulators of pH in the human body, though they require hours to days to reach maximum effect. They achieve absolute, long-term maintenance of acid-base balance by:- Bicarbonate Management: Reabsorbing 100% of filtered bicarbonate back into the blood, or actively excreting it into the toilet if the patient is alkalotic.
- Acid Excretion: Specialized "Intercalated Cells" in the kidney tubules actively pump toxic, excess H⁺ directly into the urine, where it is safely trapped by phosphate and ammonia buffers.
- De Novo Bicarbonate Generation: The ultimate lifesaver. Through a process called ammoniagenesis (breaking down the amino acid glutamine), the kidneys can actually manufacture brand new, virgin bicarbonate ions and inject them into the bloodstream to replace the ones completely destroyed during massive acid attacks (like in diabetic ketoacidosis).
VIII. Clinical Imperatives: Why Healthcare Workers MUST Master Acid-Base Balance
The control of pH is not abstract chemistry; it is a direct, daily matter of life and death on the hospital ward. The strict maintenance of blood pH between 7.35 and 7.45 is absolutely non-negotiable for human survival.
Diagnosing and Managing Acidosis & Alkalosis via ABG
Nurses and physicians frequently draw and interpret Arterial Blood Gas (ABG) tests, which definitively measure the patient's exact blood pH, PCO₂ (the respiratory/lung acid component), and HCO₃⁻ (the metabolic/kidney base component). Understanding the buffer systems is mandatory to identify the primary disturbance and evaluate if the body is actively trying to compensate.
- Acidosis (pH < 7.35): Occurs from a massive influx of acid or massive loss of base.
- Respiratory Acidosis: Caused by retaining too much CO₂. (e.g., A patient with severe COPD, asthma, or an opioid overdose causing them to stop breathing).
- Metabolic Acidosis: Caused by systemic acid buildup or bicarbonate loss. (e.g., Severe infectious Sepsis causing lactic acid buildup, Diabetic Ketoacidosis, severe prolonged diarrhea losing bicarbonate from the bowels, or late-stage Renal Failure).
- Alkalosis (pH > 7.45): Occurs from too much base or massive loss of acid.
- Respiratory Alkalosis: Caused by blowing off too much CO₂. (e.g., A patient suffering a severe panic attack/anxiety hyperventilating, or improper mechanical ventilator settings).
- Metabolic Alkalosis: Caused by a massive loss of stomach acid. (e.g., A patient suffering from severe, intractable vomiting or gastric suctioning).
Understanding Severe Disease Pathophysiology
- Diabetic Ketoacidosis (DKA): A terrifying complication of Type 1 Diabetes. Because the body lacks insulin to use glucose, it violently burns fat for energy, producing massive amounts of highly acidic "ketone bodies" (acetoacetic acid and beta-hydroxybutyric acid) at an overwhelming rate. This completely consumes and destroys the blood's bicarbonate buffer reserve, leading to severe, fatal metabolic acidosis.
Clinical Sign: The patient will exhibit Kussmaul Respirations—deep, rapid, desperate gasping breaths as the respiratory system (the Second Line of Defense) attempts to blow off massive amounts of CO₂ to save the dropping pH. - Chronic Obstructive Pulmonary Disease (COPD): A respiratory disease where alveolar destruction traps air in the lungs. Impaired, shallow ventilation leads to chronic, relentless CO₂ retention in the blood, resulting in a permanent state of Respiratory Acidosis. To compensate, the kidneys (Third Line of Defense) will retain massive amounts of Bicarbonate over several days to buffer the retained CO₂.
- Acute Renal Failure (ARF): The kidneys simply shut down and stop filtering blood. The impaired kidneys can no longer excrete the daily load of metabolic acids, nor can they regenerate new bicarbonate. This leads to a rapid, progressive, and lethal Metabolic Acidosis, often requiring emergency dialysis to save the patient.
- Aspirin Toxicity (Salicylate Poisoning): In massive overdoses, aspirin directly stimulates the brain's respiratory center, causing initial hyperventilation (Respiratory Alkalosis). However, as the drug severely disrupts cellular metabolism, massive amounts of lactic acid and ketoacids are generated, quickly plunging the patient into a severe, combined Metabolic Acidosis.
The Ultimate Clinical Goal: Protecting Enzymes and Proteins
Ultimately, recognizing and treating these conditions is about one thing: preserving the architecture of the cell. Buffers and medical interventions ensure that the optimal pH range for every single enzyme, receptor, and structural protein in the body is rigorously maintained, allowing these crucial biological catalysts to perform the functions of life without denaturing and collapsing.
IX. Recommended References & Evidence-Based Guidelines
- Guyton, A.C., & Hall, J.E.: Textbook of Medical Physiology (Chapters on Acid-Base Regulation and Respiratory Physiology).
- Nelson, D.L., & Cox, M.M.: Lehninger Principles of Biochemistry (Chapters on Water, pH, and Biological Buffers).
- Rodwell, V.W., et al.: Harper's Illustrated Biochemistry.
- Costanzo, L.S.: Physiology (Renal and Acid-Base Physiology sections for high-yield clinical board review).
- Kasper, D.L., et al.: Harrison's Principles of Internal Medicine (For the deep clinical pathophysiology of DKA, Sepsis, and Renal Failure).