
Axial and Appendicular Systems
The human skeleton is a living tissue that goes far beyond simple scaffolding. It is divided into two major functional parts: the Axial Skeleton and the Appendicular Skeleton. Together, these two divisions provide the support, protection, mineral storage, blood cell production (hematopoiesis), and leverage necessary for movement.
- Axial Skeleton: Focuses on protection and support of the vital organs (brain, spinal cord, heart, lungs).
- Appendicular Skeleton: Focuses on locomotion and environmental manipulation (walking, grasping, lifting).
PART I: The Axial Skeleton (The Body's Central Axis)
The axial skeleton forms the longitudinal axis of the body. In brief, it comprises the head and trunk. Its primary purpose is to encase and protect the body's most vital, fragile organs.
Composition (Exactly 80 bones):
- Skull (22 bones + 7 associated bones): Protects the brain and forms the face. (The 7 associated bones include the 6 auditory ossicles for hearing and the 1 hyoid bone in the neck).
- Vertebral Column (26 bones): Protects the spinal cord and supports the weight of the head and trunk.
- Thoracic Cage (25 bones): Includes the 24 ribs and 1 sternum to protect the heart and lungs.
A. The Skull
The skull is an incredibly complex bony structure that forms a protective cavity for the brain, provides the head with its shape, and anchors the facial muscles. It is formed by 22 major bones joined tightly by immovable fibrous joints called sutures (Coronal, Sagittal, Lambdoid, and Squamous sutures). It consists of two main parts: the Cranium and the Face.
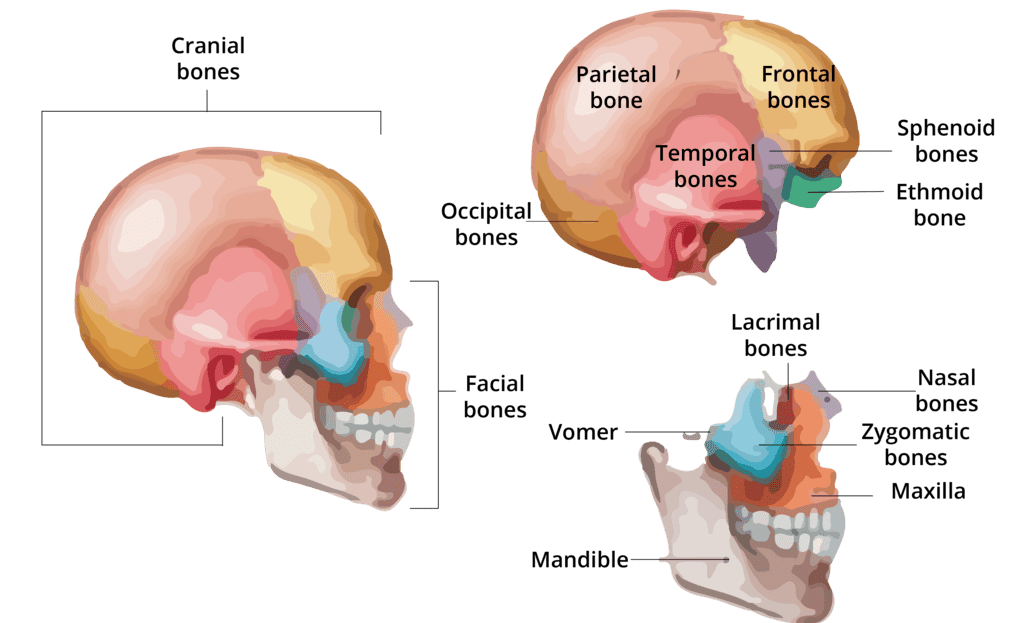
The cranium (neurocranium) is the bony vault that houses and protects the brain.
- Frontal Bone (1): Forms the forehead, the roofs of the orbits (eye sockets), and contains the frontal sinuses.
- Parietal Bones (2): Form the massive superior and lateral walls of the cranium. They meet at the top of the head at the sagittal suture.
- Temporal Bones (2): Form the inferolateral aspects of the skull and parts of the cranial base.
Clinical Detail: They house the middle/inner ear (organs of hearing and balance) and feature the Mastoid Process (attachment for neck muscles) and the Styloid Process. - Occipital Bone (1): Forms the posterior wall and most of the base of the skull.
Key Feature: Contains the massive Foramen Magnum, the large hole through which the brainstem connects to the spinal cord. It also features Occipital Condyles that rest on the first vertebra. - Sphenoid Bone (1): The central "keystone" bone of the cranium; it physically articulates with all other cranial bones. Shaped like a bat or butterfly.
Key Feature: Contains a saddle-shaped depression called the Sella Turcica, which securely holds the pituitary gland. - Ethmoid Bone (1): Forms the anterior part of the cranial floor, the medial wall of the orbits, and the roof of the nasal cavity.
Key Feature: Contains the Cribriform Plate (full of tiny holes for olfactory nerves responsible for smell) and the Crista Galli.
These bones form the framework of the face, contain cavities for sensory organs (eyes, mouth, nose), and provide attachment sites for facial expression muscles.
- Mandible (1): The lower jawbone; the largest, strongest, and ONLY freely movable bone of the skull. Forms the Temporomandibular Joint (TMJ).
- Maxillae (2): The upper jawbones; they form the anterior hard palate and hold the upper teeth in alveolar margins. They are the facial "keystone" bones.
- Zygomatic Bones (2): The cheekbones; they form the prominences of the cheeks and the inferolateral margins of the orbits.
- Nasal Bones (2): Form the bony bridge of the nose (the rest of the nose is cartilage).
- Lacrimal Bones (2): Tiny, fingernail-sized bones forming part of the medial walls of the orbits; contain the lacrimal fossa which houses the tear ducts.
- Palatine Bones (2): L-shaped bones that form the posterior part of the hard palate (roof of the mouth).
- Vomer (1): A plow-shaped bone that forms the inferior part of the nasal septum (dividing the left and right nostrils).
- Inferior Nasal Conchae (2): Scroll-like bones projecting from the lateral walls of the nasal cavity. They rapidly warm, moisten, and filter inhaled air.
Clinical & Nursing Considerations: The Skull
- Cleft Palate: Occurs when the two Maxillae bones and/or Palatine bones fail to fuse embryologically, leaving an opening between the mouth and the nasal cavity. Causes severe feeding and speech difficulties in infants.
- TMJ Dislocation: The mandible can easily dislocate anteriorly (forward) if the mouth is opened too wide (e.g., a massive yawn), leaving the patient unable to close their mouth.
- Orbital Blowout Fracture: A punch to the eye pushes the eyeball backward, breaking the fragile floor of the orbit (made mostly of the maxilla), potentially trapping eye muscles.
B. The Vertebral Column (Spine)
The vertebral column serves as the main structural mast of the body, protects the delicate spinal cord, and provides attachment points for the ribs, pelvic girdle, and back muscles. It is a flexible, curved structure composed of 26 irregular bones in adults (formed from 33 vertebrae in infants, some of which fuse later).
Functions of the Vertebral Column:
- Support: Transmits the immense weight of the head and trunk directly down to the lower limbs.
- Protection: Completely surrounds and protects the delicate, irreplaceable spinal cord within the vertebral canal.
- Movement: Provides attachment points for muscles, allowing extensive trunk bending and neck rotation.
- Shock Absorption: Intervertebral discs act as hydraulic shock absorbers during running and jumping.
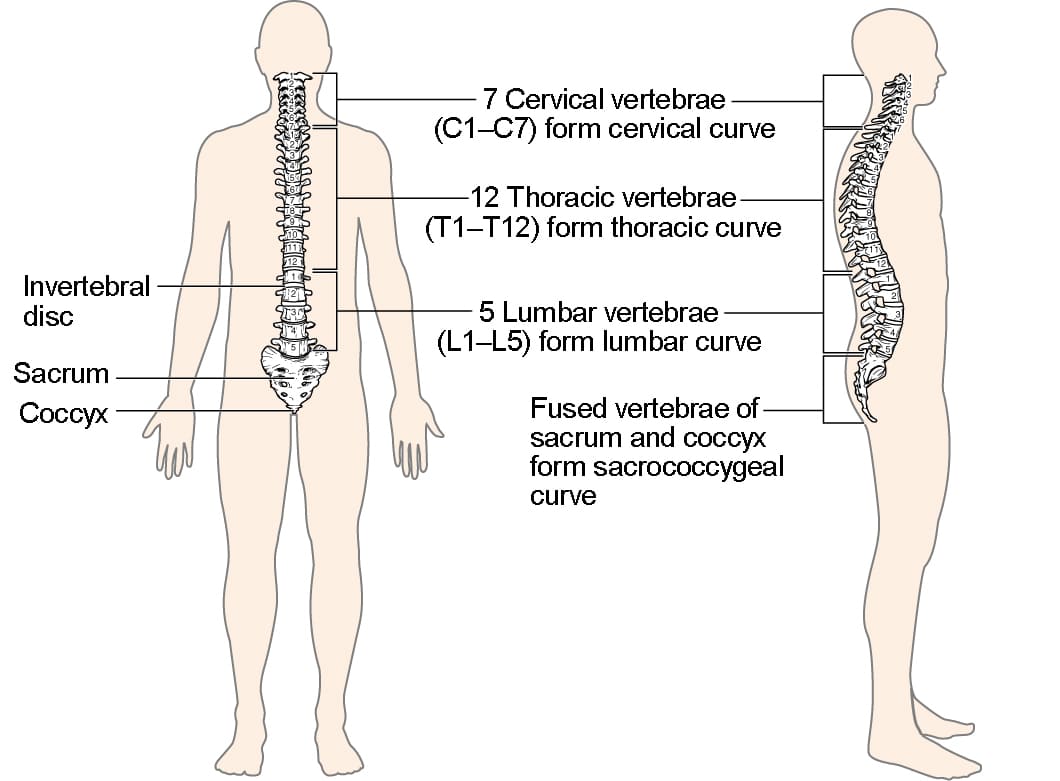
Regions and Curvatures
The spine is divided into five regions and features four natural, S-shaped curves that increase its resilience and flexibility. Without these curves, the spine would easily snap under pressure.
| Vertebral Region (Bones) | Curvature Type | Clinical / Pathological Notes |
|---|---|---|
| Cervical (C1-C7): 7 vertebrae in the neck. | Concave posteriorly (Secondary curve - develops when a baby lifts its head). | Highly mobile, susceptible to "whiplash" injury in car accidents. |
| Thoracic (T1-T12): 12 vertebrae in the chest. | Convex posteriorly (Primary curve - present at birth). | Kyphosis (Hunchback) is an exaggerated thoracic curve, common in elderly women with osteoporosis. |
| Lumbar (L1-L5): 5 vertebrae in the lower back. | Concave posteriorly (Secondary curve - develops when a baby starts walking). | Lordosis (Swayback) is an exaggerated lumbar curve, common in pregnant women or severe obesity. |
| Sacrum (1 bone): 5 fused vertebrae. | Convex posteriorly (Primary curve). | Forms the sturdy posterior wall of the pelvis. |
| Coccyx (1 bone): 3-5 fused vertebrae. | N/A | The "tailbone." Highly painful if bruised or fractured by falling hard on the buttocks. |
Note: Scoliosis is an abnormal lateral (side-to-side) curvature of the spine, usually occurring in the thoracic region.
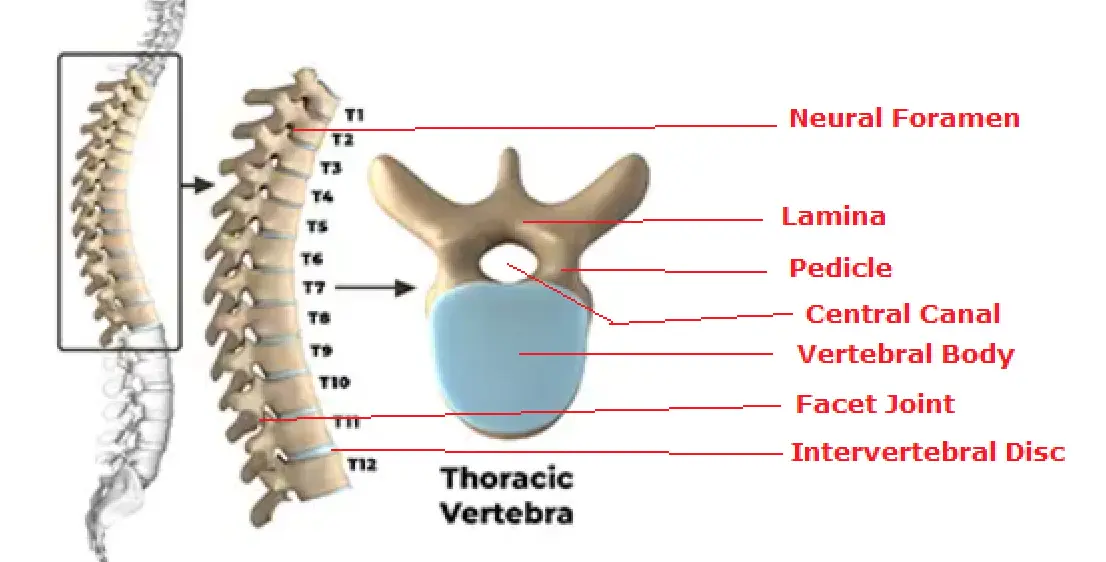
General Structure of a Vertebra and Discs
Most vertebrae share a common structural plan:
- Vertebral Body (Centrum): The anterior, massive, weight-bearing disc of bone.
- Vertebral Arch: Encloses the posterior space to form the vertebral foramen. Successive vertebral foramina line up to form the long vertebral canal for the spinal cord.
- Processes: Projections that serve as levers for muscle attachment (Spinous process, Transverse processes) and joint articulation (Superior/Inferior articular processes).
Located between adjacent vertebral bodies, these act as shock absorbers. Each is composed of an inner gelatinous core (Nucleus Pulposus) providing elasticity, and an outer tough collar of fibrocartilage (Anulus Fibrosus) holding it together.
Pathology: A "Herniated" or "Slipped" Disc occurs when the tough outer Anulus Fibrosus tears, allowing the jelly-like Nucleus Pulposus to squeeze out. This jelly presses directly on the adjacent spinal nerves, causing agonizing pain, numbness, and sciatica shooting down the leg.
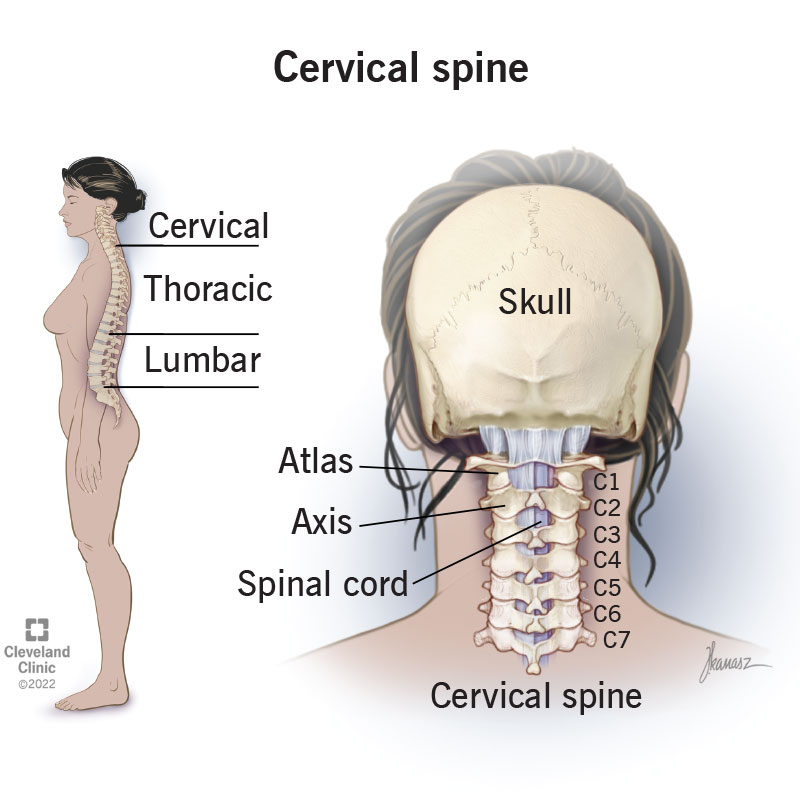
Regional Characteristics of Vertebrae
- Cervical Vertebrae (C1-C7): The smallest, lightest vertebrae. Their unique, identifying feature is the presence of Transverse Foramina (holes in the transverse processes) which protect the vertebral arteries traveling up to the brain. Most have a bifid (split) spinous process.
- C1 (Atlas): Lacks a body entirely. It is a ring of bone that holds up the skull. It allows you to nod your head "YES".
- C2 (Axis): Has a vertical bony peg called the Dens (odontoid process) that sticks up into the Atlas. It acts as a pivot, allowing you to shake your head "NO".
- Thoracic Vertebrae (T1-T12): Distinguished by their articulation with the ribs. They have Costal Facets on their bodies and transverse processes to connect to ribs. They have a heart-shaped body and a long, slender spinous process that points sharply downward like a giraffe's snout.
- Sacrum and Coccyx: The Sacrum forms the posterior wall of the pelvis, articulating with the ilium (Sacroiliac joint). The Coccyx provides slight support for pelvic floor muscles.
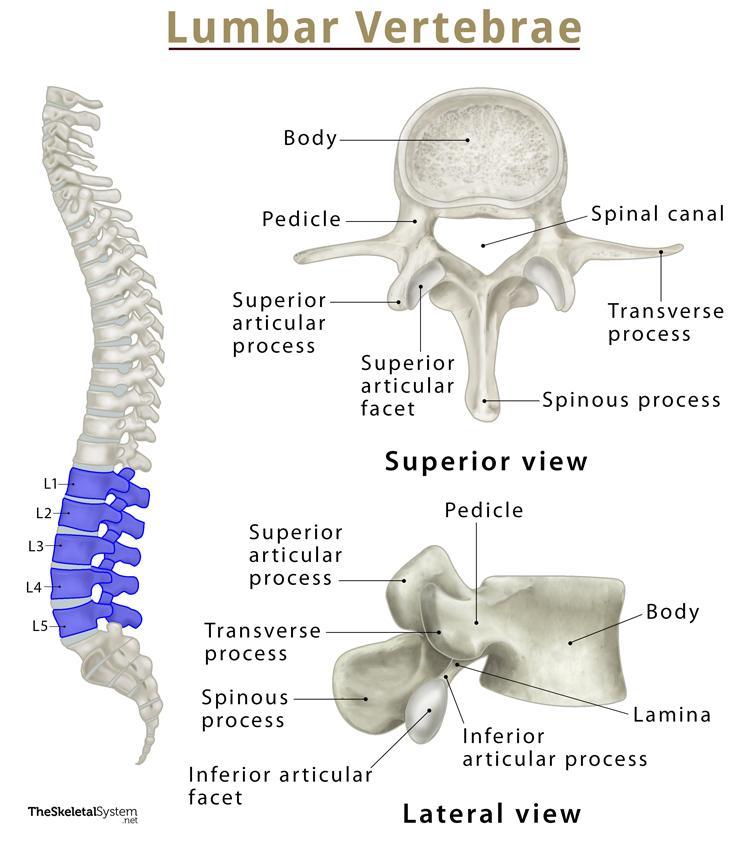 Lumbar Vertebrae (L1-L5): The largest, blockiest, and strongest vertebrae, designed to bear the immense weight of the upper body. They have a massive, kidney-shaped body and a short, thick, hatchet-like spinous process that projects straight backwards.
Lumbar Vertebrae (L1-L5): The largest, blockiest, and strongest vertebrae, designed to bear the immense weight of the upper body. They have a massive, kidney-shaped body and a short, thick, hatchet-like spinous process that projects straight backwards.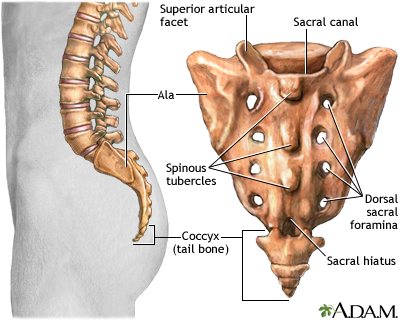
C. The Thoracic Cage (Bony Thorax)
The thoracic cage forms the protective, flexible "rib cage" around the vital organs of the chest. It includes the sternum anteriorly, the ribs laterally, and the twelve thoracic vertebrae posteriorly.
Functions of the Thoracic Cage:
- Protection: Encloses and fiercely protects the heart, lungs, and great major blood vessels (aorta/vena cava).
- Support: Provides the only skeletal attachment points for the shoulder girdles and upper limbs.
- Respiration: The flexible costal cartilages allow the rib cage to expand and compress like a bellows, acting as a biological vacuum pump for breathing.
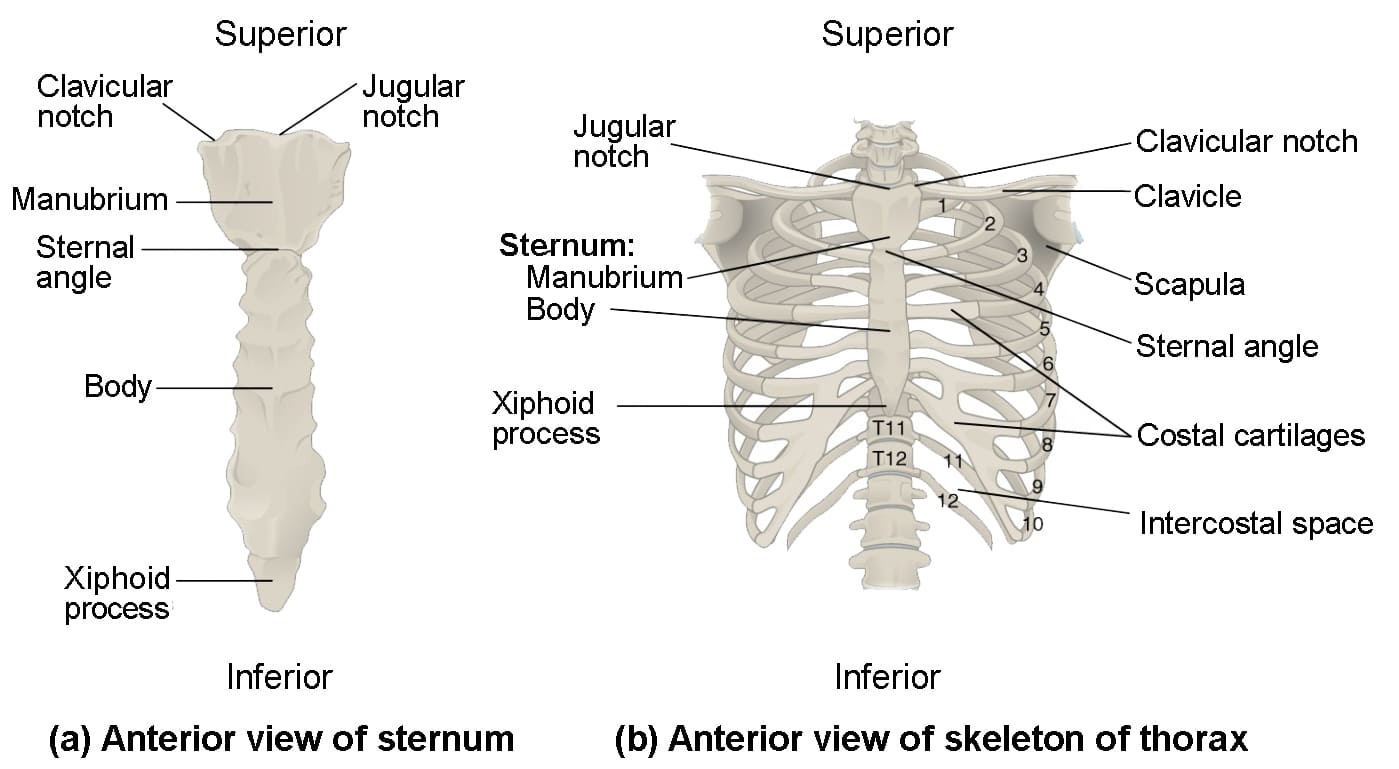
1. The Sternum (Breastbone)
A flat, dagger-like bone in the anterior midline of the thorax, composed of three fused parts:
- Manubrium: The superior "knot" of the tie. It articulates with the clavicles and the first two pairs of ribs. Features the palpable Jugular (Suprasternal) Notch at the top.
- Body (Gladiolus): The middle and largest bulk of the sternum, articulating with ribs 2-7.
- Xiphoid Process: The inferior-most, tiny sword-like projection. It is hyaline cartilage in youth but ossifies in adults. It serves as an attachment point for the diaphragm and some abdominal muscles.
Clinical Note (Sternal Angle / Angle of Louis): The palpable horizontal ridge where the manubrium meets the body. It is a critical clinical landmark for nurses and doctors because it marks exactly where the 2nd rib attaches, allowing clinicians to accurately count ribs downward to place stethoscopes for listening to heart valves or performing ECGs.
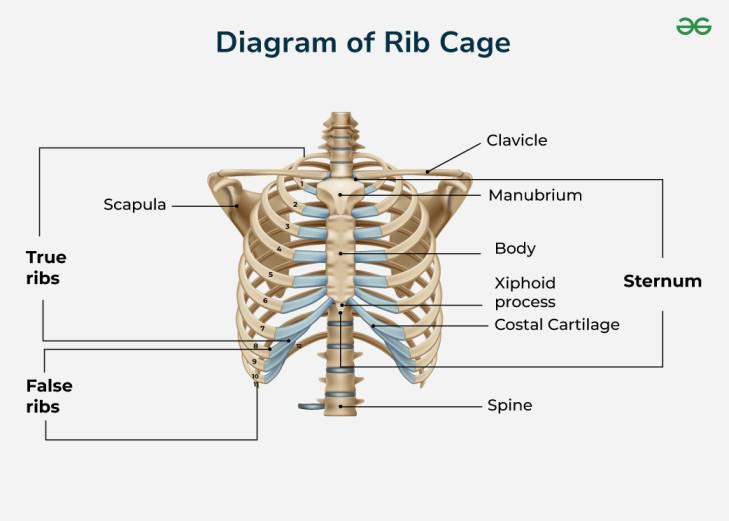
2. The Ribs (12 pairs)
All 24 ribs attach posteriorly to the thoracic vertebrae and curve inferiorly and anteriorly toward the front of the body.
- True Ribs (Pairs 1-7): Also called vertebrosternal ribs. They attach directly to the sternum via their own individual bars of hyaline costal cartilage.
- False Ribs (Pairs 8-12):
- Pairs 8-10 (Vertebrochondral ribs): Attach indirectly to the sternum by fusing their costal cartilage to the cartilage of the 7th rib above them.
- Pairs 11-12 (Floating Ribs): They have no anterior attachment at all. Their anterior tips embed freely into the lateral body wall muscles.
- Head: The posterior wedge that articulates with the vertebral body.
- Neck & Tubercle: The tubercle articulates with the transverse process of the vertebra.
- Shaft (Body): The main, curved, flat portion of the rib.
- Costal Groove: A highly important deep groove on the inferior (bottom) border of the inside of the rib. It houses and protects the delicate intercostal nerve, artery, and vein. (Nursing Note: During a thoracentesis / chest tube insertion, the needle is ALWAYS passed over the TOP of a rib to avoid severing these vessels hidden in the groove below).
PART II: The Appendicular Skeleton
The appendicular skeleton encompasses the limbs (appendages) and the girdles that physically anchor those limbs to the axial skeleton. It is designed for maximum mobility.
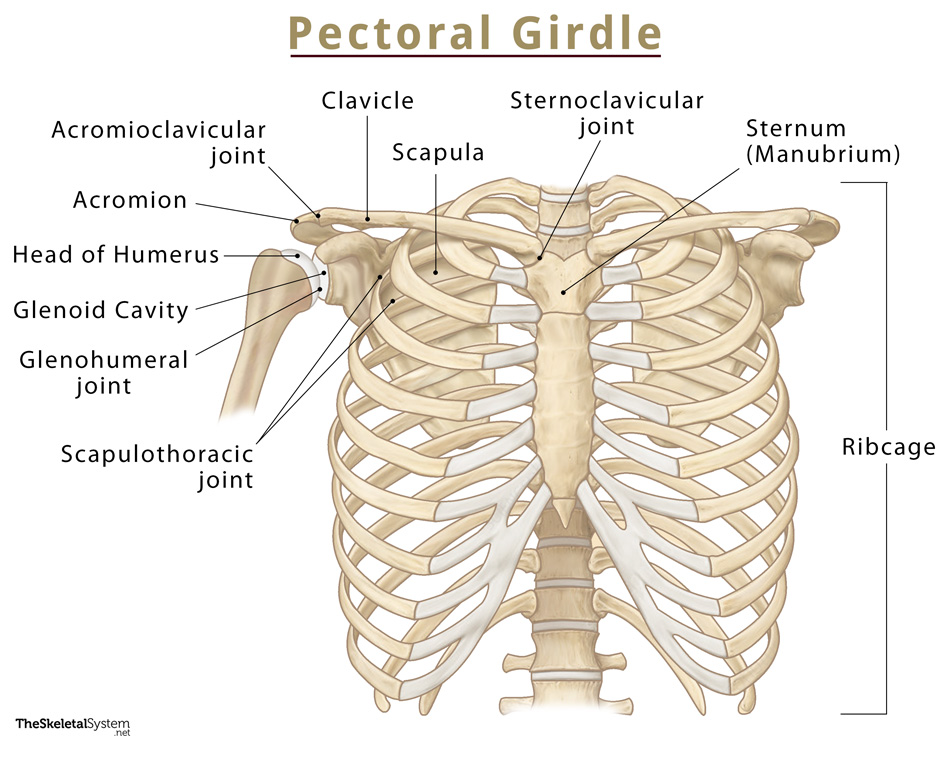
A. The Pectoral (Shoulder) Girdle
The pectoral girdle consists of two bones on each side of the body: the clavicle (collarbone) and the scapula (shoulder blade). These bones attach the upper limbs to the axial skeleton.
Functions and Biomechanics:
The pectoral girdle is exceptionally light and allows the upper limb a degree of mobility seen nowhere else in the body. This extreme flexibility comes at the cost of stability (which is why shoulder dislocations are incredibly common). Mobility is maximized because:
- The only bony attachment to the axial skeleton is the tiny sternoclavicular joint.
- The socket of the shoulder joint (glenoid cavity) is exceedingly shallow and poorly reinforced.
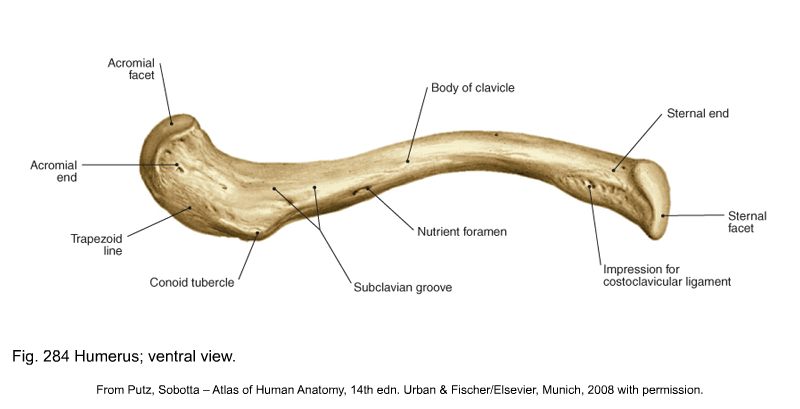
1. The Clavicle (Collarbone)
A slender, S-shaped bone lying horizontally across the superior thorax. It acts as a strut or brace, holding the heavy scapula and arm away from the narrow upper trunk to ensure the arm swings freely.
- Sternal (medial) end: Blocky and round. Articulates with the manubrium of the sternum (Sternoclavicular joint).
- Acromial (lateral) end: Flattened. Articulates with the acromion of the scapula (Acromioclavicular joint).
Clinical Note - FOOSH Injury: The clavicle is highly sensitive to force. When a person falls on an outstretched hand (FOOSH), the massive force travels up the arm and snaps the clavicle. It almost always fractures outward at its middle third, keeping the broken bone fragments from piercing the vital subclavian artery lurking just beneath it.
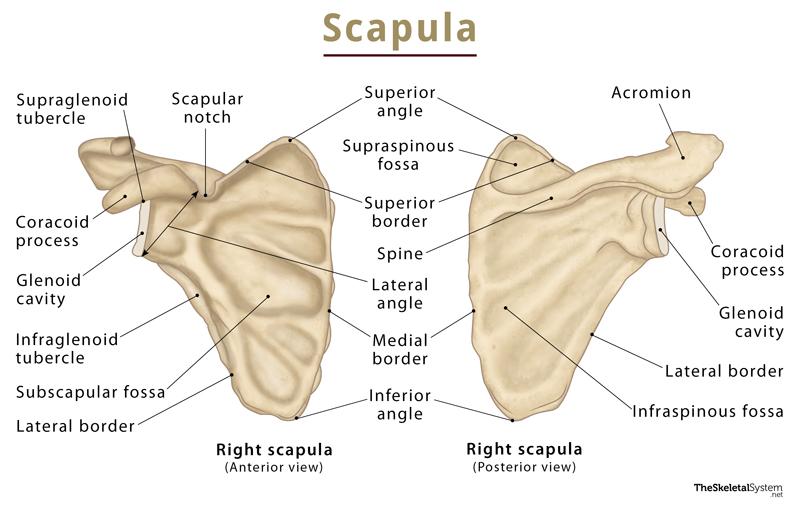
2. The Scapula (Shoulder Blade)
A thin, triangular flat bone resting on the posterior aspect of the rib cage (ribs 2 through 7). It provides immense surface area for muscle attachment.
- Spine & Acromion: The Spine is a prominent ridge on the posterior surface that you can easily feel. It ends laterally in the enlarged, flattened Acromion (the bony tip of your shoulder).
- Glenoid Cavity (Fossa): A shallow, pear-shaped depression on the lateral angle. It articulates with the head of the humerus to form the glenohumeral (shoulder) joint.
- Coracoid Process: A hook-like process projecting anteriorly, resembling a bent finger. It serves as a vital anchor point for the biceps muscle and ligaments.
- Fossae (Depressions): Feature three major depressions for the massive rotator cuff muscles: the Supraspinous Fossa (above the spine), Infraspinous Fossa (below the spine), and Subscapular Fossa (the entire anterior surface facing the ribs).
B. The Upper Limbs
Each upper limb consists of 30 exact bones, highly adapted for dexterity, reaching, and manipulation. They are divided into the arm, forearm, and hand.
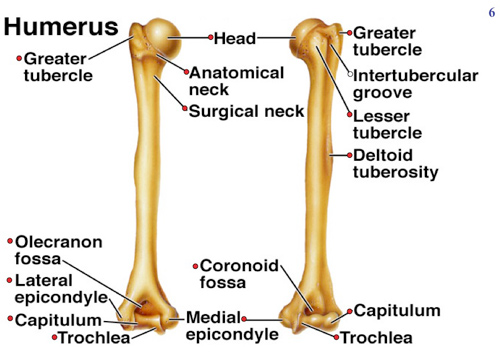
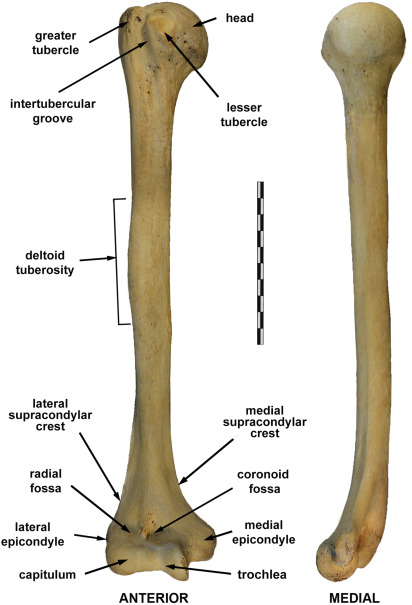
1. The Arm (Brachium): The Humerus
The humerus is the single bone of the upper arm, extending from the shoulder to the elbow. It is the longest and largest bone of the upper limb.
- Proximal End: Features the smooth, hemispherical Head which fits into the glenoid cavity. Just below it is the Anatomical Neck. Adjacent are the Greater and Lesser Tubercles (sites of rotator cuff attachment), separated by the intertubercular sulcus. Below the tubercles is the Surgical Neck, named because it is the most frequently fractured part of the humerus.
- Shaft: Includes the roughened Deltoid Tuberosity midway down for deltoid muscle attachment, and the posterior Radial Groove where the radial nerve wraps around the bone.
- Distal End: Forms the elbow joint. It features two specialized articular surfaces: the medial spool-shaped Trochlea (articulates with the ulna) and the lateral ball-like Capitulum (articulates with the radius). It also features prominent Medial and Lateral Epicondyles (the "funny bone" nerve runs behind the medial epicondyle) and fossae (Olecranon, Coronoid, Radial) that accommodate the forearm bones during flexion and extension.
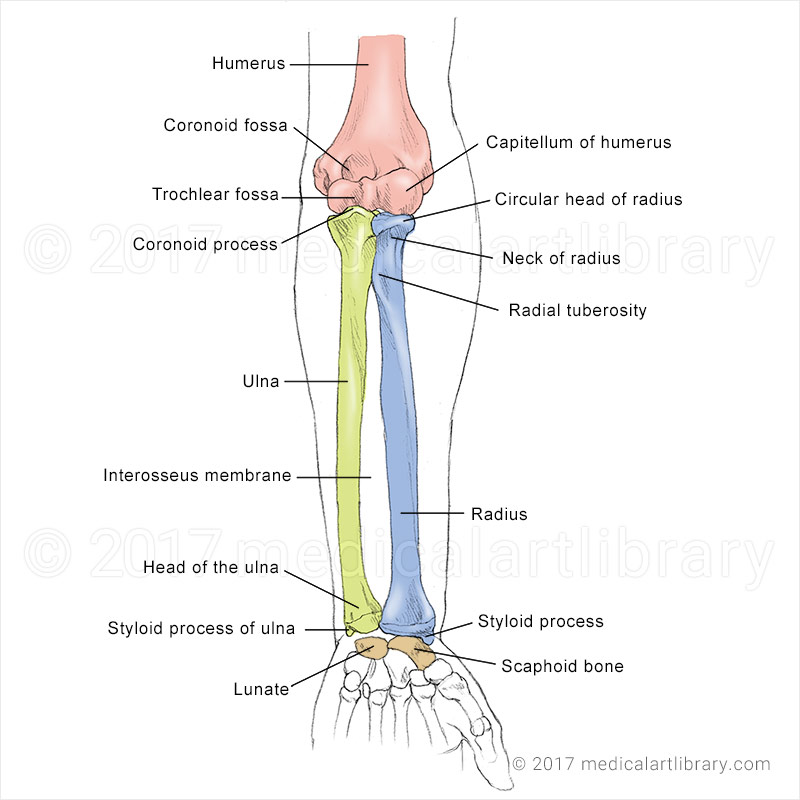
2. The Forearm (Antebrachium): Radius and Ulna
The forearm contains two parallel bones connected lengthwise by a flexible, ligamentous Interosseous Membrane. In the anatomical position (palms facing forward), the Radius is lateral (thumb side) and the Ulna is medial (pinky side).
- Ulna (Medial Bone): The longer bone, solely responsible for forming the hinge joint of the elbow.
- Proximal end: Features the massive, hook-like Olecranon Process (the literal "point" of the elbow you rest on a table) and the Coronoid Process. Together they form the deep Trochlear Notch, which perfectly grips the trochlea of the humerus like a wrench.
- Distal end: Small and narrow, featuring a Head and a pointed Styloid Process.
- Radius (Lateral Bone): The primary bone responsible for the wrist joint and forearm rotation (pronation/supination).
- Proximal end: Features a flat, nail-head shaped Head that swivels against the humerus and ulna. Below it is the Radial Tuberosity (anchors the biceps brachii).
- Distal end: Broad and massive, featuring a pointed Styloid Process on the thumb side.
Clinical Note (Colles' Fracture): A common fracture of the distal end of the radius, often caused by trying to break a fall with hands flat on the ground. The wrist is forced upward, displacing the radius backwards into a "dinner fork" deformity.
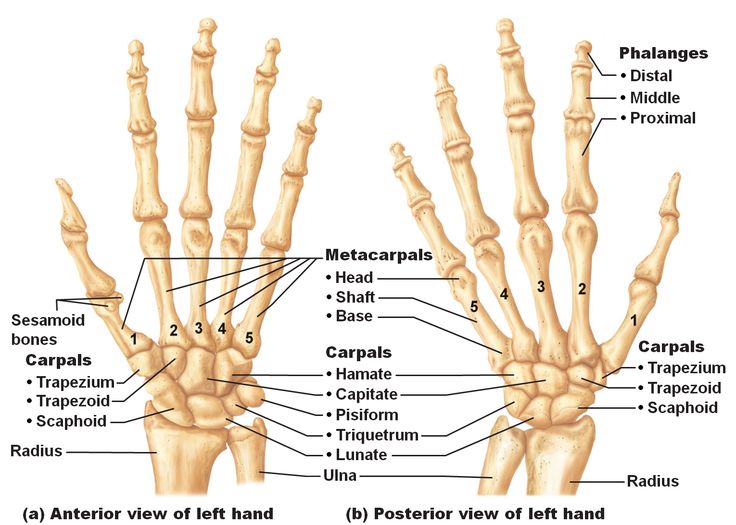
3. The Hand (Manus)
Each hand contains 27 specialized bones, divided into three regions:
| Region | Bone Details | Specific Bones & Features |
|---|---|---|
| Carpus (Wrist) | 8 small Carpal bones arranged in two rows of 4. They slide over each other providing incredible wrist flexibility. |
Proximal Row (lateral to medial): Scaphoid, Lunate, Triquetrum, Pisiform. Distal Row (lateral to medial): Trapezium, Trapezoid, Capitate, Hamate. Mnemonic Some Lovers Try Positions That They Can't Handle. Clinical: The Scaphoid is the most frequently fractured carpal bone (falling on the palm). It has poor blood supply and suffers avascular necrosis. |
| Metacarpus (Palm) | 5 long bones numbered I to V starting from the thumb. | Their bases articulate with the carpals. Their bulbous distal heads form your "knuckles" when you clench your fist. |
| Phalanges (Fingers) | 14 miniature long bones forming the digits. |
Thumb (Pollex - Digit I): Has only two phalanges (Proximal and Distal). Fingers (Digits II-V): Each has three phalanges (Proximal, Middle, and Distal). |
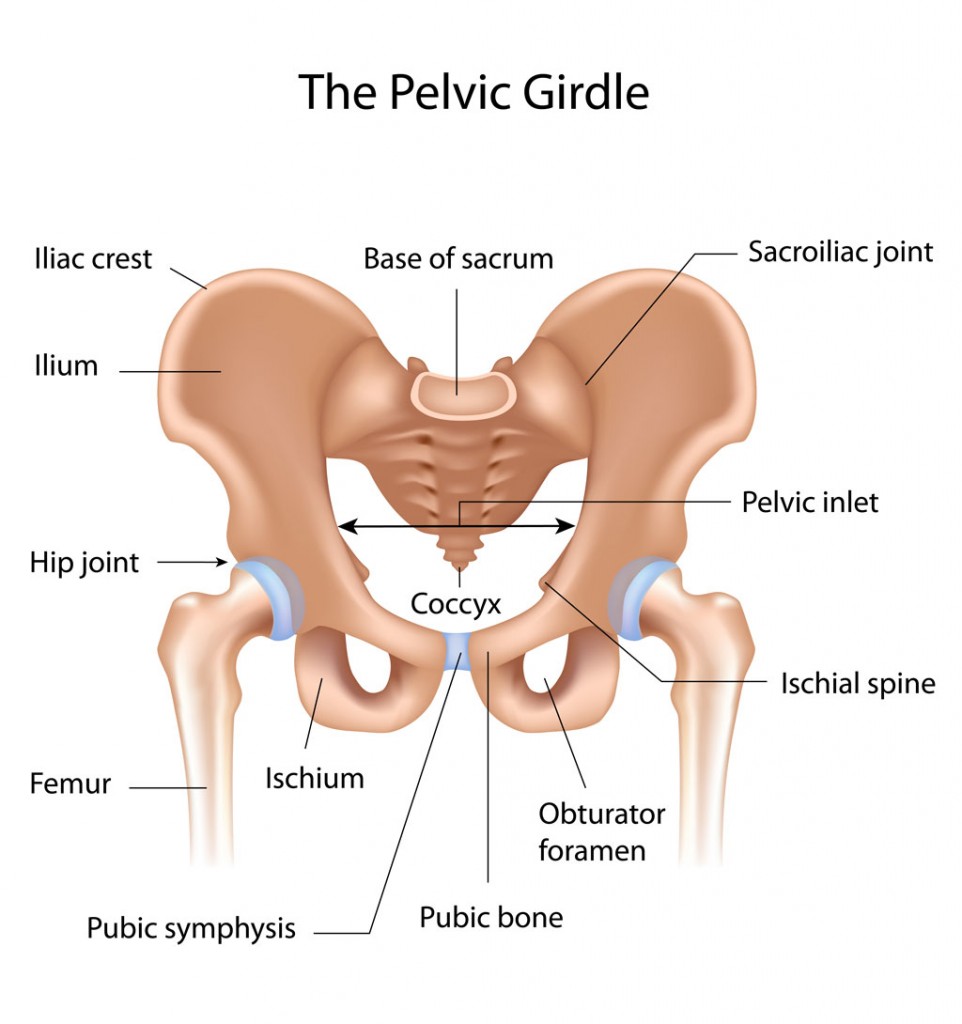
C. The Pelvic Girdle (Hip Girdle)
The pelvic girdle is a massive, robust, heavy basin-shaped structure. It is formed by two Ossa Coxae (hip bones or innominate bones), which articulate strongly with the sacrum posteriorly and with each other anteriorly.
Functions of the Pelvic Girdle:
- Support: Transmits the entire massive weight of the upper body directly down to the lower limbs.
- Protection: A deep bony cradle that encloses and fiercely protects the pelvic organs (urinary bladder, reproductive organs, lower colon).
- Stability over Mobility: Unlike the shoulder, the hip joint socket is extremely deep and heavily reinforced by ligaments, sacrificing mobility for absolute stability.
1. Bones of the Pelvic Girdle: The Os Coxa
Each os coxa is a large, irregularly shaped bone formed by the embryological fusion of three separate bones: the Ilium, Ischium, and Pubis. They fuse perfectly at the Acetabulum, the deep hemispherical socket that holds the head of the femur.
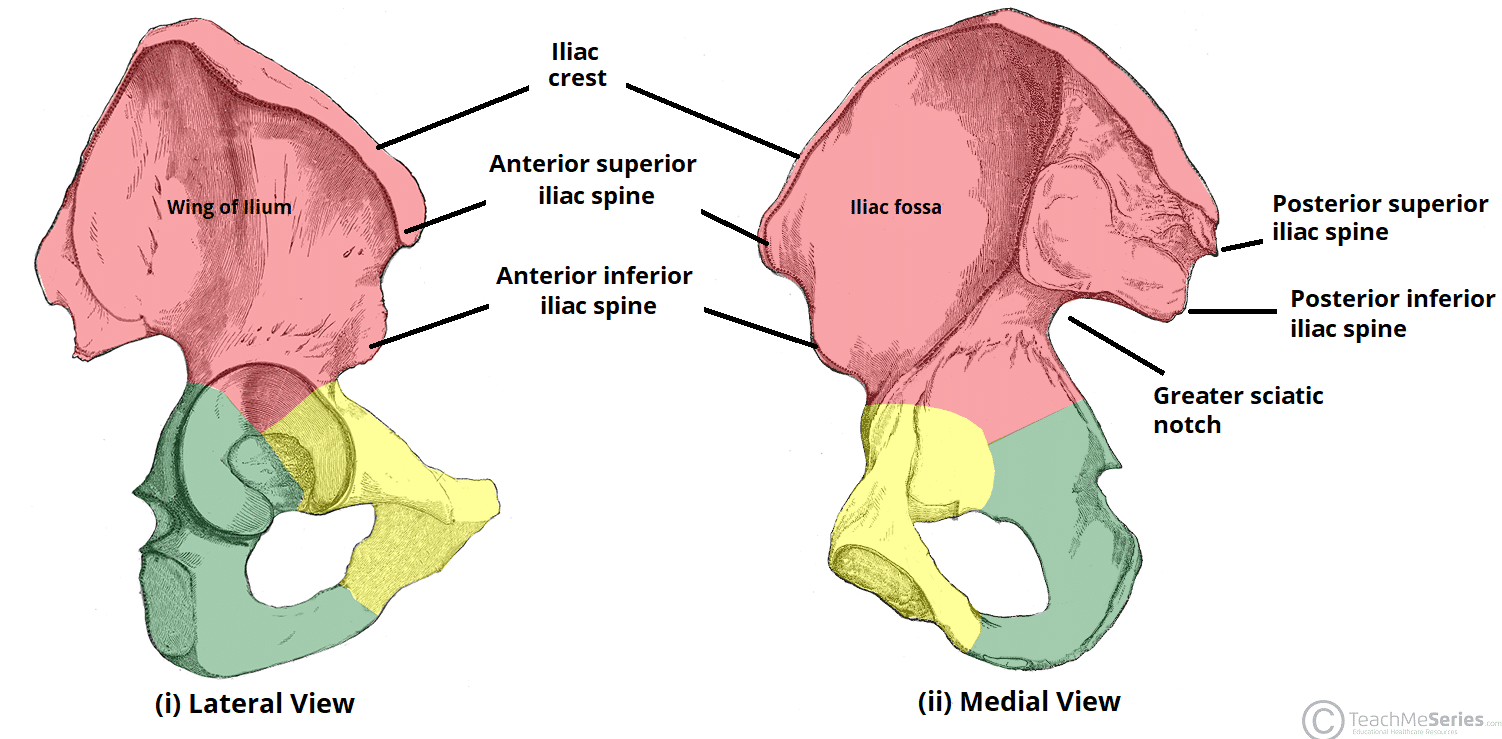
- a. Ilium: The largest, flaring, superior bone forming the upper flank (the part you rest your hands on).
- Iliac Crest: The thickened superior margin of the ilium.
- ASIS & PSIS: Anterior and Posterior Superior Iliac Spines. Crucial anatomical landmarks for taking bone marrow biopsies or identifying muscle attachments.
- Greater Sciatic Notch: A deep indentation through which the massive sciatic nerve passes to reach the thigh.
- Auricular Surface: A roughened ear-shaped area that tightly articulates with the sacrum to form the Sacroiliac joint.
- b. Ischium: Forms the posteroinferior, L-shaped part of the hip bone.
- Ischial Tuberosity: The massive, roughened, lowest projection of the pelvis. These are your "sit bones." When you sit on a hard chair, this bone bears all your weight.
- Ischial Spine: A sharp projection pointing medially into the pelvic cavity.
- c. Pubis: Forms the V-shaped anteroinferior part of the hip bone.
- Pubic Symphysis: The anterior joint where the two pubic bones meet, joined by a thick disc of fibrocartilage.
- Pubic Arch: The inverted V-shape angle formed below the pubic symphysis.
2. Important Features of the Pelvis as a Whole
- Obturator Foramen: A massive opening inferior to the acetabulum, formed by the ischium and pubis. While large in bone, in life it is almost entirely sealed shut by a fibrous membrane, allowing only a few small nerves and vessels to pass.
- Pelvic Brim (Inlet): A continuous oval ridge that divides the pelvis into two halves.
- Greater (False) Pelvis: The broad, shallow area superior to the brim. It acts as part of the abdominal cavity, supporting intestines.
- Lesser (True) Pelvis: The deep bowl inferior to the brim. It surrounds the pelvic cavity proper and entirely defines the birth canal in women.
The female pelvis is evolutionarily modified to strictly accommodate childbearing and fetal passage.
- Overall Structure: Male pelvis is thick, heavy, and narrow. Female pelvis is light, thin, wider, and shallower.
- Pelvic Inlet (Brim): Male is heart-shaped. Female is a wider, spacious oval.
- Pubic Arch/Angle: Male is acute (V-shaped, 50-60 degrees). Female is broad and round (U-shaped, 80-90 degrees).
- Coccyx: Male points rigidly forward. Female is straighter and more flexible, pointing inferiorly to open the birth canal.
D. The Lower Limbs
Each lower limb carries the entire weight of the erect body and is subjected to exceptional forces during running and jumping. Therefore, its 30 bones are significantly thicker, heavier, and stronger than upper limb bones.
1. The Thigh: Femur and Patella
- a. Femur (Thigh Bone): The single bone of the thigh. It is the longest, thickest, strongest, and heaviest bone in the body, accounting for about 1/4 of a person's total height.
- Proximal End: Features the perfectly spherical Head which drives deep into the acetabulum. The head contains a small central pit (Fovea Capitis) where a vital stabilizing ligament attaches. The head is carried on a constricted Neck. Just below the neck are the massive Greater and Lesser Trochanters for major thigh and gluteal muscle attachment.
- Shaft: Bows slightly forward. Features a prominent posterior vertical ridge called the Linea Aspera (the "rough line") where massive hamstring/quadriceps tendons anchor.
- Distal End: Widens into massive, wheel-like Medial and Lateral Condyles that articulate with the tibia to form the knee joint. Between them anteriorly is the smooth Patellar Surface where the kneecap glides.
Clinical Note - "Broken Hip": When elderly individuals (especially those with osteoporosis) are said to have a "broken hip," they have almost always actually fractured the Neck of the Femur, not the pelvic bone itself. The neck is the weakest point of the femur.
- b. Patella (Kneecap): A triangular sesamoid bone (a bone embedded entirely within a tendon) enclosed in the quadriceps tendon. It protects the knee joint anteriorly and drastically improves the mechanical leverage of the thigh muscles pulling on the leg.
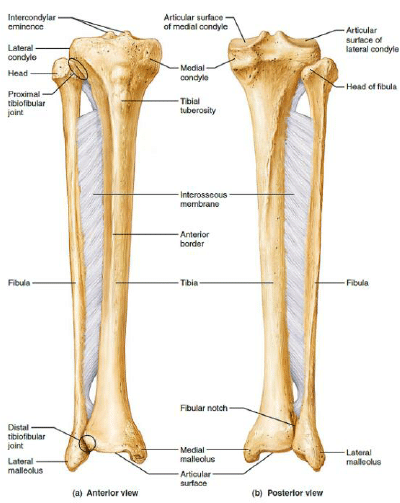
2. The Leg: Tibia and Fibula
The leg consists of two parallel bones connected by an interosseous membrane. However, unlike the forearm, these two bones cannot cross over each other (no rotation).
- a. Tibia (Shin Bone): The massive, medial, primary weight-bearing bone of the lower leg. It receives the entire weight of the body from the femur and transmits it to the foot.
- Proximal end: Features broad, flat Medial and Lateral Condyles. Just below them anteriorly is the massive Tibial Tuberosity, which anchors the patellar ligament. (Pathology: Inflammation here in growing teenagers is known as Osgood-Schlatter disease).
- Shaft: Features a sharp anterior crest (your shin) which is unprotected by muscle and highly sensitive to kicks.
- Distal end: Forms the inner bulge of the ankle, the Medial Malleolus.
- b. Fibula (Lateral Bone): A thin, stick-like bone on the outside of the leg. It bears NO body weight whatsoever, but is vital for muscle attachment and lateral ankle stabilization.
- Proximal end: The Head articulates with the side of the tibia.
- Distal end: Expands to form the prominent outer bulge of the ankle, the Lateral Malleolus. (Pathology: A Pott's Fracture involves the severe breaking of both the medial and lateral malleoli, often from forceful ankle twisting).
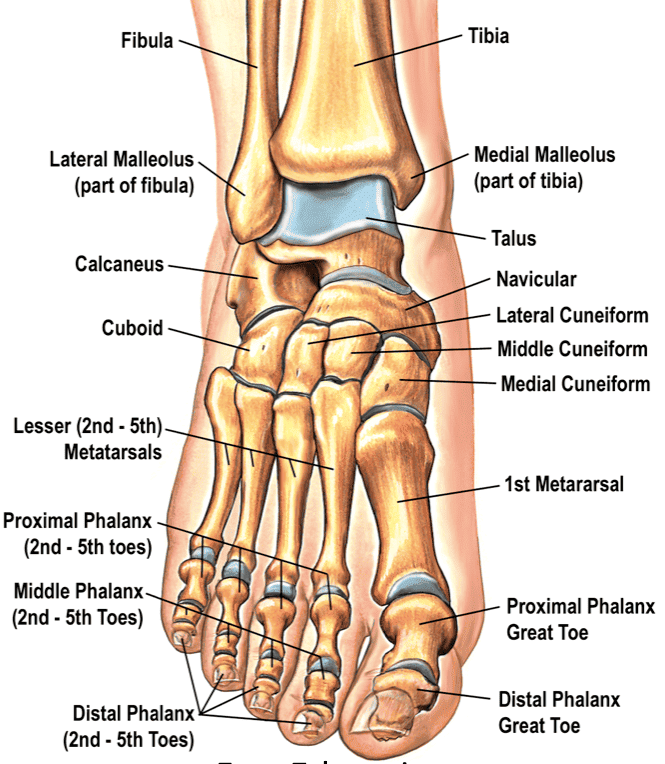
3. The Foot
The 26 bones of the foot have two critical functions: to support the crushing weight of the entire body, and to act as a flexible lever to propel the body forward during walking/running.
| Region | Bone Details | Specific Bones & Features |
|---|---|---|
| Tarsus (Ankle/Posterior Foot) | 7 irregularly shaped bones forming the back half of the foot. Weight is carried heavily here. |
Talus: The uppermost bone. It articulates with the tibia and fibula to form the true ankle joint. It is the only foot bone that directly receives body weight from the leg. Calcaneus: The massive heel bone. The talus rests upon it. It bears the brunt of walking and anchors the thick Achilles (calcaneal) tendon. Others: Cuboid (lateral), Navicular (medial), and three Cuneiforms (Medial, Intermediate, Lateral). |
| Metatarsus (Midfoot) | 5 long bones making up the sole of the foot. | Numbered I to V from medial (big toe) to lateral (pinky toe). The enlarged head of Metatarsal I forms the "ball" of the foot. |
| Phalanges (Toes) | 14 miniature bones forming the digits. |
Big Toe (Hallux - Digit I): Has two massive phalanges (Proximal and Distal). Other Toes (Digits II-V): Each has three tiny phalanges (Proximal, Middle, Distal). |
4. The Arches of the Foot
The foot is not flat on the ground. The bones are uniquely arranged into three interlocking, springy arches supported by heavily strained ligaments and muscle tendons. These arches allow the foot to bear weight while providing "give" (like a leaf spring in a truck suspension) to absorb shock and bounce back during walking.
- Medial Longitudinal Arch: The highest arch, curving well above the ground on the inside of the foot. (When this arch collapses, the patient suffers from "flat feet" or pes planus).
- Lateral Longitudinal Arch: A very low arch on the outside of the foot.
- Transverse Arch: Runs obliquely across the midfoot from one side to the other.
List of References & Recommended Reading
- Moore, K. L., Dalley, A. F., & Agur, A. M. (2018). Clinically Oriented Anatomy (8th ed.). Lippincott Williams & Wilkins.
- Standring, S. (2020). Gray's Anatomy: The Anatomical Basis of Clinical Practice (42nd ed.). Elsevier.
- Tortora, G. J., & Derrickson, B. (2017). Principles of Anatomy and Physiology (15th ed.). Wiley.
- Marieb, E. N., & Hoehn, K. (2018). Human Anatomy & Physiology (11th ed.). Pearson.
- Netter, F. H. (2018). Atlas of Human Anatomy (7th ed.). Elsevier.