
Embryology of the Central Nervous System (CNS) and Comprehensive Neuroanatomy
The development of the nervous system begins very early in embryonic life and represents one of the most highly complex and tightly regulated processes in human biology. By the end of this exhaustive master guide, you will be deeply conversant with:
- The step-by-step embryological formation of the CNS (Neural Plate to Vesicles).
- The clinical significance of neural tube defects (NTDs) and specific congenital anomalies.
- The gross anatomy, lateralization, and functional localization of the cerebral hemispheres.
- The comprehensive blood supply of the brain and specific stroke syndromes.
- The specialized microscopic role of glial cells, specifically astrocytes.
Part I: Early Embryology of the Central Nervous System
1. Neural Plate Formation (Week 3)
The entire central nervous system originates from a specialized layer of cells during the third week of embryonic development.
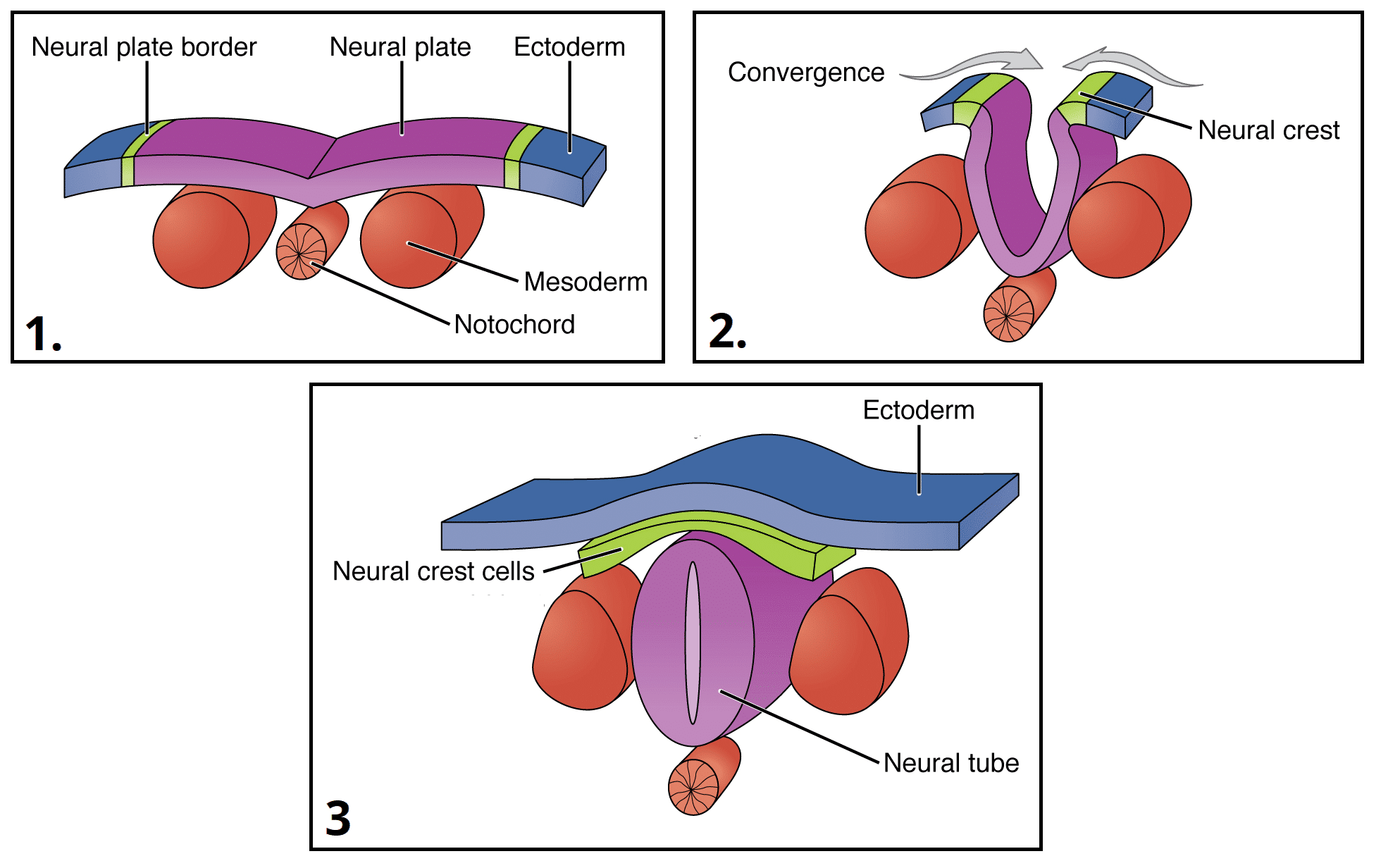
- Origin: The CNS appears as a slipper-shaped plate of thickened ectoderm called the neural plate.
- Induction: This process does not happen spontaneously; it is chemically induced by the underlying notochord (a transient, flexible, rod-like structure formed from mesoderm) and paraxial mesoderm. The notochord acts as the primary signaling center, secreting powerful molecular signaling molecules (most notably Sonic Hedgehog, SHH). These chemical gradients induce the overlying ectoderm to thicken and differentiate into the neural plate.
- Location: It forms in the mid-dorsal region of the embryo, anterior to the primitive node, running cranially from the Hensen's node (primitive node).
2. Neural Fold and Neural Tube Formation (Weeks 3-4)
Following induction, the flat neural plate must transform into a 3D tube.
- Neural Folds: The lateral edges of the neural plate elevate aggressively to form neural folds, while the center depresses, forming a longitudinal neural groove in the midline.
- Fusion: The neural folds grow toward each other, eventually meeting in the midline and fusing. Crucial Detail: This fusion does not happen all at once. It typically begins in the cervical region (around the 4th somite level) and proceeds bidirectionally like a zipper closing in two directions simultaneously:
- Cranially: Zipping up towards the head.
- Caudally: Zipping down towards the tail.
- Neural Tube: The complete fusion of the neural folds successfully transforms the neural plate into the neural tube. This hollow, fluid-filled tube will ultimately give rise to the entire CNS (the brain and the spinal cord).
The Neural Crest Cells: "The 4th Germ Layer"
As the neural folds fuse and the neural tube closes and pinches off from the surface ectoderm, a highly specialized population of cells at the very crests of the neural folds detaches. These are the neural crest cells.
They are remarkably pluripotent (capable of turning into many different cell types) and migrate extensively throughout the entire embryo. Because of their immense contribution to the body, scientists often jokingly refer to them as the 4th germ layer. They give rise to a vast array of structures, including:
- Peripheral Nervous System (PNS): Sensory ganglia (dorsal root ganglia), autonomic ganglia (sympathetic chain).
- Melanocytes: The pigment-producing cells in the skin.
- Adrenal Medulla: The inner core of the adrenal gland that secretes adrenaline.
- Craniofacial structures: Bones, cartilage, and connective tissues of the face.
- Schwann cells: The myelin-producing glial cells of the PNS.
- Meninges: The pia mater and arachnoid mater.
3. Neuropore Closure (Week 4)
Because the neural tube "zips" closed starting from the middle, the two ends remain temporarily open.
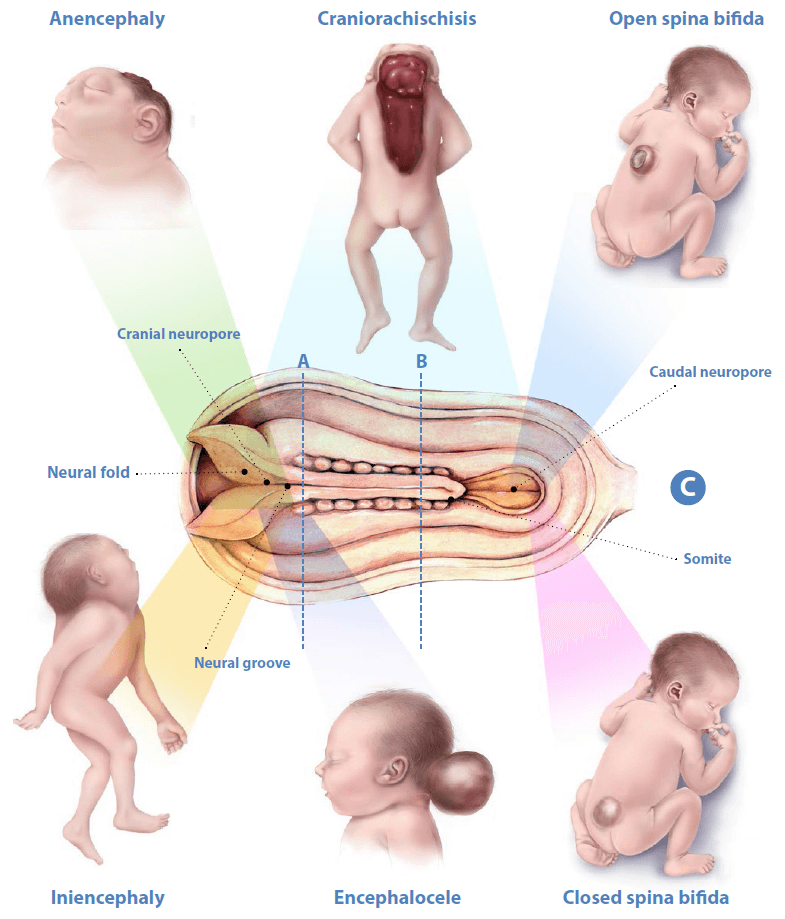
- Communication with Amniotic Cavity: Once fusion is initiated, the open, unzipped ends of the neurotube form the cranial (anterior) neuropore and the caudal (posterior) neuropore. These neuropores temporarily communicate directly with the amniotic cavity, allowing for the free exchange of amniotic fluid into the central canal.
- Closure Timing (Crucial):
- Closure of the Cranial Neuropore: Occurs at approximately the 18-20 somite stage (around Day 25). This closure is absolutely essential for normal brain and skull development.
- Closure of the Caudal Neuropore: Occurs approximately 2 days later (around Day 27). This closure is essential for normal lower spinal cord and lower vertebral development.
Clinical Significance: Neural Tube Defects (NTDs)
Failure of these neuropores to close properly at precisely the right time results in severe, often catastrophic birth defects known as NTDs. Because the tube is open, alpha-fetoprotein (AFP) and acetylcholinesterase (AChE) leak into the amniotic fluid, which can be detected via maternal blood tests or amniocentesis.
- Anencephaly: Failure of the cranial neuropore to close. This leads to the complete absence of a major portion of the brain, skull, and scalp. The developing brain is exposed to toxic amniotic fluid and degenerates. This condition is uniformly fatal, incompatible with life outside the womb.
- Spina Bifida: Failure of the caudal neuropore to close, resulting in incomplete closure of the vertebral column and exposure of the spinal cord. Severity varies drastically (discussed in detail in the Congenital Anomalies section).
Prevention: Supplementation with Folic Acid (Vitamin B9) before conception and during early pregnancy significantly reduces the incidence of NTDs. Folic acid is required for nucleotide synthesis and rapid cell division during tube closure.
Part II: Brain Vesicles and Flexures
4. Primary Brain Vesicles (Late Week 4)
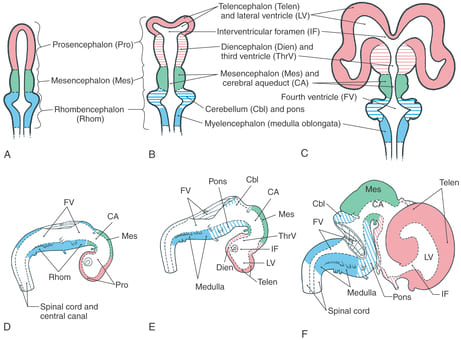
Once the cranial neuropore perfectly closes, the cephalic (cranial) end of the neural tube undergoes rapid, explosive growth and ballooning. It forms three distinct dilations known as the primary brain vesicles:
- Prosencephalon (Forebrain): The most rostral (front-most) vesicle.
- Mesencephalon (Midbrain): The middle vesicle, a relatively short connecting segment.
- Rhombencephalon (Hindbrain): The most caudal (back-most) vesicle, continuous with the future spinal cord.
5. Secondary Brain Vesicles (Week 5)
By the fifth week of gestation, rapid cellular proliferation causes the primary vesicles to further subdivide, resulting in five secondary brain vesicles:
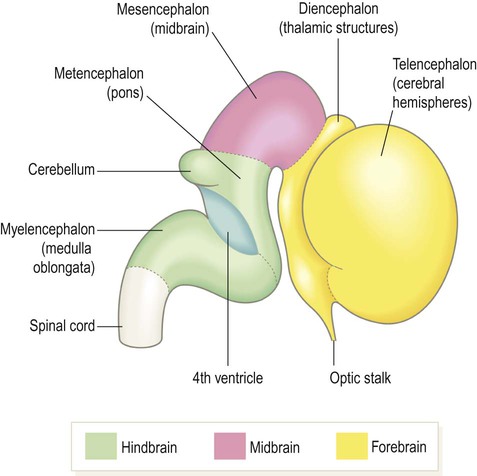
- Prosencephalon (Forebrain) divides into:
- Telencephalon: The most rostral part. It consists of a midline portion and two enormous lateral outgrowths that will aggressively expand to become the primitive cerebral hemispheres.
- Diencephalon: Forms the central core of the forebrain. It develops vital outgrowths, notably the optic vesicles (which will extend outwards to form the retina and optic nerve).
- Mesencephalon (Midbrain) remains undivided. It retains its name and basic structure.
- Rhombencephalon (Hindbrain) divides into:
- Metencephalon: Will develop into two major structures: the pons (anteriorly) and the cerebellum (posteriorly).
- Myelencephalon: The lowest brain segment, which will develop into the medulla oblongata, seamlessly blending into the spinal cord.
Summary Table of Brain Vesicle Derivatives
| Primary Vesicle (Week 4) | Secondary Vesicles (Week 5) | Adult Brain Structure Derivative |
|---|---|---|
| Prosencephalon (Forebrain) | Telencephalon | Cerebral Hemispheres (Cerebral cortex, subcortical white matter, basal ganglia) |
| Diencephalon | Thalamus, Hypothalamus, Epithalamus (Pineal gland), Optic cup | |
| Mesencephalon (Midbrain) | Mesencephalon | Midbrain (Tectum, tegmentum, cerebral peduncles) |
| Rhombencephalon (Hindbrain) | Metencephalon | Pons and Cerebellum |
| Myelencephalon | Medulla Oblongata | |
| Caudal Neural Tube | Remains undivided | Spinal Cord |
6. Brain Flexures
During this period of intense, rapid growth, the developing brain runs out of linear space within the embryonic constraints. To accommodate this massive growth, the brain tube folds and bends at specific weak points, forming flexures:
- Cephalic (Midbrain) Flexure: Occurs exactly in the midbrain region, bending the forebrain severely ventrally (forward). This explains why the human brain is angled roughly 90 degrees to the spinal cord, unlike quadrupeds like dogs or horses where it is straight.
- Cervical Flexure: Occurs at the distinct junction of the rhombencephalon (myelencephalon) and the beginning of the spinal cord.
- Pontine Flexure: Occurs in the metencephalon. This flexure bends in the opposite direction (dorsally), opening up the neural tube to create the wide, diamond-shaped floor of the fourth ventricle and giving characteristic shape to the pons and cerebellum.
7. Development of the Ventricular System
Lumen Continuity: It is critical to understand that the neural tube is hollow. The central lumen (canal) of the spinal cord is perfectly continuous with the ballooning cavities inside the brain vesicles above. This continuous, unbroken lumen ultimately forms the entire ventricular system of the adult brain, which is the internal plumbing system filled with Cerebrospinal Fluid (CSF).
Specific Luminal Derivatives:
- Lumen of the Telencephalon: Forms the immense, C-shaped Lateral Ventricles (one massive ventricle inside each cerebral hemisphere).
- Lumen of the Diencephalon: Forms the slit-like Third Ventricle in the very center of the brain.
- Lumen of the Mesencephalon: Because the midbrain doesn't expand much, its lumen narrows dramatically to form a tiny pipe called the Cerebral Aqueduct (of Sylvius).
- Lumen of the Metencephalon and Myelencephalon: Combine and widen out to form the tent-shaped Fourth Ventricle.
- Lumen of the caudal neural tube: Remains as the microscopic Central Canal of the Spinal Cord.
Flow and Connections of CSF:
CSF is constantly produced by the choroid plexus inside the ventricles and must flow outward.
- The Lateral Ventricles empty their fluid into the Third Ventricle through two small holes called the Interventricular Foramina (of Monro).
- The Third Ventricle sends fluid down into the Fourth Ventricle via the narrow Cerebral Aqueduct.
- The Fourth Ventricle allows fluid to escape into the subarachnoid space (the space surrounding the entire outside of the brain and spinal cord) via three crucial exit doors: two lateral Foramina of Luschka and one median Foramen of Magendie. Some fluid also continues straight down into the central canal of the spinal cord.
Part III: Congenital Anomalies of the CNS
Errors in the embryological steps described above lead to profound anatomical defects.
1. Spina Bifida
A neural tube defect (NTD) resulting from the incomplete closure of the caudal neural tube and/or the bony vertebrae in the spinal column protecting it. The severity exists on a massive spectrum.
- Spina Bifida Occulta: The mildest, most benign form. There is a small gap or failure of fusion in the bony vertebrae (usually L5 or S1), but the spinal cord and meninges are perfectly normal. It is usually entirely asymptomatic. Clinical Sign: A tuft of hair, a dimple, or a small birthmark on the lower back might be the only physical sign.
- Meningocele: The meninges (membranes surrounding the spinal cord) protrude outwards through the vertebral bone defect, forming a fluid-filled cystic sac visible on the baby's back. However, the spinal cord itself safely remains within the vertebral canal. This may cause minor neurological problems and is surgically repairable.
- Myelomeningocele (Meningiomyelocoele): The most severe and devastating form. Both the spinal cord tissues and nerve roots protrude through the bony opening, heavily tangling within the exposed sac. This leads to profound, permanent neurological deficits below the level of the lesion, including total leg paralysis, loss of sensation, severe bowel/bladder incontinence, secondary hydrocephalus, and severe learning difficulties.
Cause: Failure of the caudal neuropore to close completely during early embryonic development.
2. Hydrocephalus ("Water on the Brain")
An abnormal, dangerous accumulation of cerebrospinal fluid (CSF) within the brain's ventricles or subarachnoid space. Because fluid builds up, it causes increased intracranial pressure. In infants (before the skull bones fuse), this forces the head to rapidly enlarge to massive proportions.
- Causes:
- Obstruction (Non-communicating Hydrocephalus): A physical blockage prevents CSF from flowing out of the ventricles. The most common cause is aqueductal stenosis (the tiny cerebral aqueduct gets blocked), or blockages caused by expanding brain tumors or post-inflammatory adhesions.
- Impaired Absorption (Communicating Hydrocephalus): Fluid flows perfectly out of the ventricles into the subarachnoid space, but the tiny drains (arachnoid granulations) that return fluid to the blood are clogged. Commonly caused by post-meningitis scarring or subarachnoid hemorrhage.
- Overproduction: Exceedingly rare, such as a tumor of the choroid plexus (choroid plexus papilloma) aggressively secreting too much fluid.
- Symptoms (in infants): Rapid, alarming increase in head circumference, a bulging/tense fontanelle (soft spot), downward-deviating eyes ("sunsetting" sign due to pressure on midbrain cranial nerves), relentless vomiting, high-pitched crying, irritability, and seizures.
- Treatment: Prompt surgical placement of a shunt system (e.g., a ventriculoperitoneal or VP shunt) that acts as a physical tube to divert the excess pressurized CSF from the brain down into the peritoneal (abdominal) cavity where the body can safely reabsorb it.
3. Microcephaly
An abnormally small head circumference for the child's age and sex, strictly defined as being more than two standard deviations below the mean average.
- Diagnosis: Based on prenatal ultrasound biometry where the occipito-frontal diameter (OFD) and biparietal diameter (BPD) are drastically reduced, or detected immediately at birth.
- Causes: This indicates that the brain itself either failed to develop properly or suffered an insult that stopped its growth. The skull simply stops growing when the brain stops growing. Examples include:
- Genetic abnormalities: Severe chromosomal disorders (e.g., Trisomy 13 or 18) or single gene mutations.
- Prenatal TORCH infections: Intrauterine infections like Zika virus (famously causing outbreaks of microcephaly), toxoplasmosis, cytomegalovirus (CMV), and rubella.
- Exposure to toxins: Maternal heavy alcohol consumption (Fetal Alcohol Syndrome), or illicit drugs.
- Severe maternal malnutrition.
- Perinatal complications: Hypoxic-ischemic encephalopathy (severe lack of oxygen during a difficult birth).
- Complications: Mental retardation/Severe intellectual disability, associated physical anomalies, unmanageable seizures, and cerebral palsy. The prognosis varies heavily based on the root cause.
4. Macrocephaly
An abnormally large head circumference, typically defined as more than two standard deviations above the mean.
- Causes:
- Benign Familial Macrocephaly: Often a harmless, inherited genetic trait (the child simply has a large head, like the parents, with normal intelligence).
- Hydrocephalus: As discussed, fluid buildup drastically expands the unfused skull.
- Brain Tumors: Massive space-occupying lesions.
- Subdural Hematomas: Large, expanding accumulations of blood under the dura mater.
- Genetic Syndromes: Such as Sotos syndrome or Fragile X syndrome.
- Megalencephaly: The brain tissue itself is abnormally large, heavy, and overgrown.
5. Anencephaly
A completely fatal neural tube defect characterized by the absence of a major portion of the brain, skull, and scalp. The cerebral hemispheres are utterly absent, leaving the brainstem exposed or reduced to small, hemorrhagic, fibrotic masses.
- Cause: Catastrophic failure of the cranial neuropore to close completely during early embryonic development (around day 25).
- Prognosis: Always fatal. The infant is usually stillborn or survives for only a few agonizing hours or days after birth.
Part IV: Anatomy of the Cerebral Hemispheres
Growth, Shape, and Basic Structure
- Growth and Shape: The cerebral hemispheres exhibit a massive "C-shape" growth pattern. As they explosively proliferate during embryology, they expand forward, upward, backward, and finally downward, curling back over the diencephalon and brainstem like a mushroom cap.
- Longitudinal Fissure: The deep, gaping canyon that perfectly divides the entire cerebrum into the left and right halves.
- Cerebral Cortex (Grey Matter):
- The 2-4 mm thick outer layer of each hemisphere, composed primarily of billions of neuron cell bodies, dendrites, unmyelinated axons, and supportive glial cells. This is the ultimate seat of conscious thought, where all higher-level processing, memory, and voluntary action occur.
- Its highly convoluted, wrinkled surface is made up of ridges (gyri) and grooves (sulci). This wrinkling is a brilliant evolutionary design to significantly increase the total surface area, allowing a massive number of neurons to pack inside a relatively small skull.
- Contralateral Control: A fundamental rule of neuroanatomy. The left hemisphere consciously controls and feels the right half of the body, and vice-versa. This occurs because of a massive crossing-over of nerve fibers known as decussation.
- The primary motor descending pathways (the corticospinal tracts) decussate in the pyramids of the lower medulla oblongata.
- Similarly, ascending sensory pathways cross over at various levels of the spinal cord or brainstem.
Functional Divisions: The Four Lobes
The highly convoluted surface is mapped by specific deep grooves. The central sulcus and the lateral sulcus serve as massive borders, dividing each cerebral hemisphere into four distinct anatomical sections called lobes:
- Central Sulcus (Fissure of Rolando): The most important vertical groove. It divides the frontal lobe from the parietal lobe. It is crucial because it strictly separates the primary motor cortex (which lies immediately anterior to it in the precentral gyrus) from the primary somatosensory cortex (which lies immediately posterior to it in the postcentral gyrus).
- Lateral Sulcus (Sylvian Fissure): The deepest, most prominent horizontal groove. It separates the massive frontal and parietal lobes above from the temporal lobe hanging below.
- Parieto-occipital Sulcus: Not as incredibly deep on the lateral surface as the central or lateral sulci, but on the medial surface, it serves to sharply demarcate the parietal lobe from the visual occipital lobe.
"Starting from the top of the hemisphere, the upper regions of the motor and sensory areas control the lower parts of the body." This incredible mapping is known as the Homunculus (Latin for "little man").
In both the primary motor cortex and primary somatosensory cortex, every single body part is specifically mapped to an exact coordinate on the gyrus in an upside-down (inverted) fashion.
- The feet, legs, and genitals hang over the very top edge and dip into the medial longitudinal fissure.
- The trunk, arms, and hands occupy the convex lateral middle surface.
- The face, lips, tongue, and throat are located at the very bottom, near the lateral sulcus.
Furthermore, the mapping is disproportionate. Body parts that require extreme, fine-tuned motor control (like the fingers, thumb, and lips) or possess extreme sensory sensitivity have massive territories on the brain map. If you drew the man based on brain space, he would have gigantic hands, massive lips, and a tiny trunk/legs.
Part V: Cerebral Dominance (Lateralization)
Lateralization describes the tendency for one cerebral hemisphere to be heavily dedicated or "more involved" in certain highly complex functions than the other. It is incorrect to say one hemisphere is entirely "dominant" over the other for all things; rather, specific skills are highly specialized.
The "Analytical" Brain
For the vast majority of people (roughly 90-95% of right-handers and 70% of left-handers), the left hemisphere is the absolute dominant controller for Language.
- Broca's Area: Located in the inferior frontal gyrus. It is the engine essential for speech production.
Clinical Damage: Causes Broca's aphasia (expressive/non-fluent aphasia). The patient knows exactly what they want to say, but physical speech is incredibly slow, stuttering, effortful, and grammatically broken (e.g., "Walk... dog... park"). Comprehension is perfectly preserved, making this deeply frustrating for the patient. - Wernicke's Area: Located in the posterior superior temporal gyrus. It is the dictionary essential for language comprehension.
Clinical Damage: Causes Wernicke's aphasia (receptive/fluent aphasia). The patient can speak at a normal, rapid pace effortlessly, but the words are entirely random, meaningless, and nonsensical ("word salad"). Furthermore, their comprehension is totally destroyed—they cannot understand what you are saying to them.
Key Left Brain Characteristics: Logical, Analytical, Sequential Processing, Linear thought, Objective, Focuses on details, Math and science reasoning.
The "Creative & Spatial" Brain
The right hemisphere tends to be globally dominant for complex non-verbal skills, massive spatial perception, and high-level emotional interpretation.
- Emotional Functions:
- Emotional Prosody: The vital ability to understand and express the musical, emotional tone of voice. Damage leads to aprosodia (speaking like a flat robot).
- Empathy: Comprehending the emotionality of others by reading facial expressions and subtle body language.
- Wit and Humor: Understanding complex jokes, heavy irony, and satire.
- Attentional Functions:
- Spatial Attention: Crucially, the right parietal lobe directs attention to BOTH the right and left sides of external space. Damage here causes hemispatial neglect, a bizarre syndrome where a stroke patient completely ignores the entire left side of their body and universe (e.g., only eating food on the right side of the plate).
- Cognitive Functions: Spatial orientation (reading maps, mental rotation), music appreciation (processing melodies), and facial recognition (damage here causes prosopagnosia—inability to recognize familiar faces).
Key Right Brain Characteristics: Random, Intuitive, Holistic, Synthesizing, Subjective, Looks at massive wholes rather than tiny details.
Handedness and Language Dominance
- Right-handed people: ~95% have left-hemisphere dominance for language.
- Left-handed people: This group is neurologically much more diverse.
- ~70% have left-hemisphere dominance for language (exactly like right-handers).
- ~15% have right-hemisphere dominance for language.
- ~15% have bilateral (shared) language representation.
Brain Plasticity and Hemispherectomy
Neuroplasticity: The brain is not hardwired in stone. It possesses an incredible ability to reassign functions to spared areas, especially in early childhood. The earlier an injury occurs, the better the chances for the undamaged hemisphere to physically rewire and compensate for lost language functions. This capacity severely diminishes with adult age.
This is beautifully demonstrated by a Hemispherectomy—a radical neurosurgical procedure where an entire diseased cerebral hemisphere is surgically removed or totally disconnected to stop severe, intractable, life-threatening epilepsy (e.g., Rasmussen's encephalitis) in very young children. Incredibly, if done early enough, the child's remaining single hemisphere adapts to take over language, motor, and cognitive functions, allowing for a relatively highly functional life.
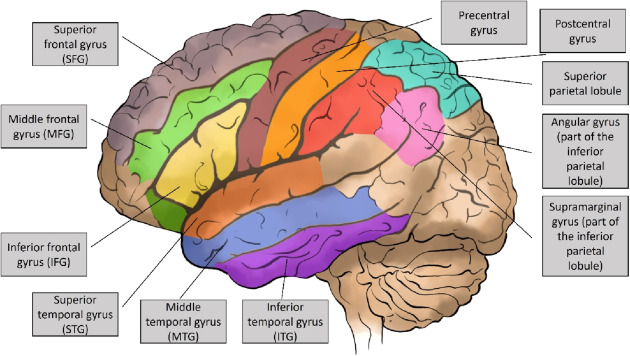
Part VI: Cortical Localization (Specific Gyri and Sulci)
Medical professionals map the brain using a strict atlas of gyri and sulci.
- AnGy - Angular Gyrus: Located in the parietal lobe. Highly involved in advanced language, complex number processing/math, spatial cognition, and memory retrieval.
- Csul - Central Sulcus: The grand divider between the frontal and parietal lobes.
- LonFis - Longitudinal Fissure: The deep midline chasm separating the left and right hemispheres.
- MFGy - Middle Frontal Gyrus: Part of the frontal lobe, heavily involved in active working memory and cognitive control.
- OGy - Occipital Gyri: The posterior pole of the brain; entirely dedicated to complex visual processing.
- PoCGy - Postcentral Gyrus: Located in the parietal lobe, immediately posterior to the central sulcus. This is the ultimate home of the primary somatosensory cortex.
- PoSul - Parieto-occipital Sulcus: The boundary dividing the parietal and occipital lobes.
- PrCGy - Precentral Gyrus: Located in the frontal lobe, immediately anterior to the central sulcus. This is the ultimate home of the primary motor cortex.
- SFGy - Superior Frontal Gyrus: Part of the upper frontal lobe, involved in deep self-awareness, introspection, and working memory.
- SMGy - Supramarginal Gyrus: Located in the parietal lobe, bridging auditory and visual signals, highly involved in language perception and empathy.
- SPLob - Superior Parietal Lobule: Part of the parietal lobe, responsible for generating spatial orientation and navigating the physical world.
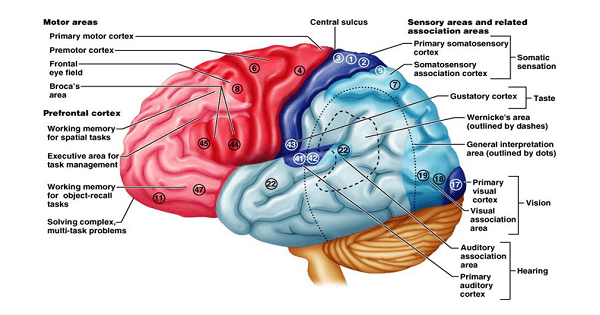
Functional Groupings
- A. Sensory Areas: Receive and interpret sensory info. The Primary Somatosensory Cortex (S1) in the postcentral gyrus receives direct touch/pain/temperature input relayed from the thalamus. Secondary sensory areas surrounding it perform complex interpretation (e.g., feeling a coin in your pocket and knowing it's a coin without looking).
- B. Motor Areas: The Primary Motor Cortex (M1) in the precentral gyrus executes the final movement command via large pyramidal Betz cells. Anterior to it is the Premotor Cortex and Supplementary Motor Area (SMA), which meticulously plan and organize complex sequences of movement before passing the blueprint to M1 to fire.
- C. Speech Areas: Broca's (production) and Wernicke's (comprehension).
- D. Association Areas: Massive tracts of cortex that integrate different senses and manage reasoning, personality, and decision making (specifically the prefrontal cortex).
Part VII: Blood Supply of the Brain (Cerebral Vasculature)
The brain is incredibly metabolically demanding. It receives a rich, redundant, high-pressure blood supply from two massive arterial systems: the Internal Carotid Arteries (anterior circulation) and the Vertebral Arteries (posterior circulation).
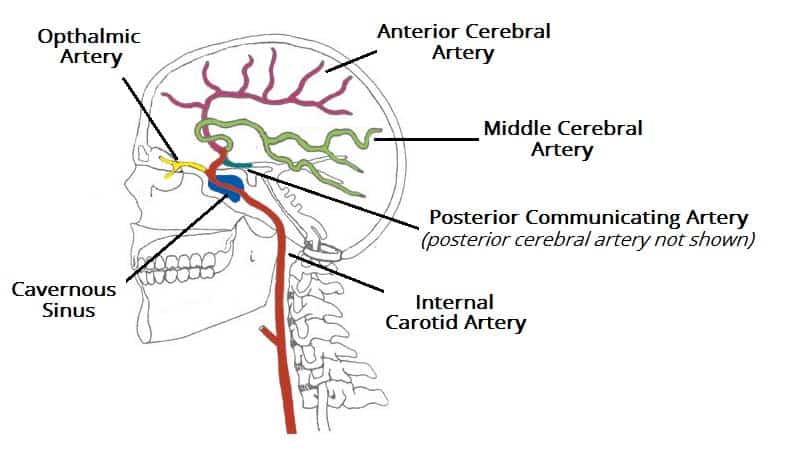
Supplies the vast majority of the anterior and lateral cerebrum.
- Ophthalmic Artery: Supplies the eye and optic nerve.
- Anterior Choroidal Artery: Supplies the choroid plexus, hippocampus, and vital internal capsule.
- Middle Cerebral Artery (MCA):
Distribution: The largest branch. It supplies the entire massive lateral surface of the frontal, parietal, and temporal lobes. This includes the motor/sensory cortices for the upper limbs and face, plus Broca's and Wernicke's language areas.
Clinical Significance: The most common artery involved in severe ischemic stroke. An MCA stroke causes massive contralateral hemiparesis (paralysis) and sensory loss heavily affecting the face and arm (much more than the leg), and devastating aphasia if on the dominant side. - Anterior Cerebral Artery (ACA):
Distribution: Runs straight up into the longitudinal fissure to supply the medial surfaces of the frontal and parietal lobes. This zone houses the motor/sensory homunculus area for the lower limbs.
Clinical Significance: An ACA stroke leads to unique contralateral weakness and sensory loss predominantly in the leg and foot, often sparing the face and arms. - Anterior Communicating Artery: A tiny but vital bridge connecting the left and right ACAs.
Supplies the brainstem, cerebellum, and posterior cerebrum.
- Vertebral Artery Branches: The posterior inferior cerebellar artery (PICA), anterior spinal artery, and posterior spinal arteries.
- Basilar Artery: The two vertebrals merge to form the giant basilar artery running up the pons. It branches into the Anterior Inferior Cerebellar Artery (AICA), Pontine arteries, and Superior Cerebellar Artery (SCA).
- Posterior Cerebral Artery (PCA):
Distribution: The terminal bifurcation of the basilar artery. It sweeps back to supply the occipital lobe (primary visual cortex), inferior temporal lobe, thalamus, and midbrain.
Clinical Significance: A PCA stroke obliterates the visual cortex, leading to contralateral homonymous hemianopia (loss of the same half of the visual field in both eyes), and sometimes profound memory deficits. - Posterior Communicating Artery: The crucial bridge that connects the posterior PCA system back forward to the anterior Internal Carotid system.
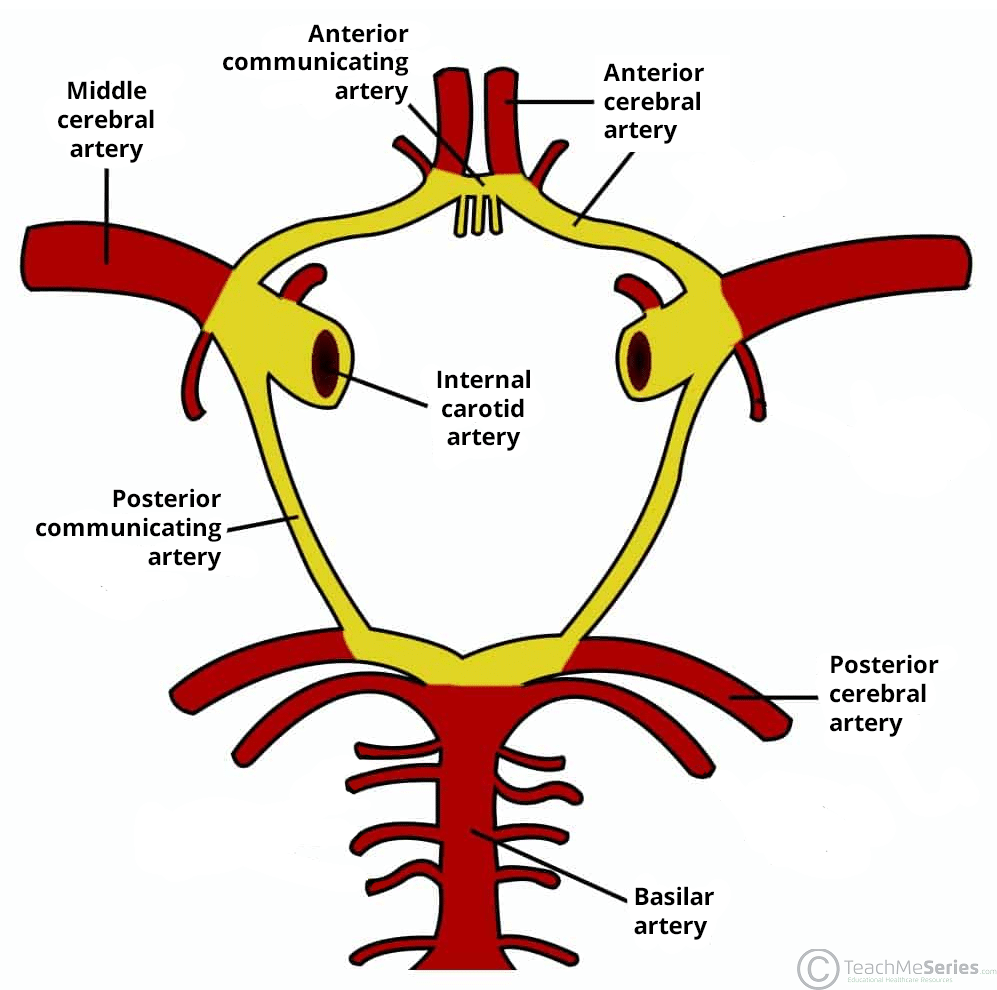
The Circle of Willis
A brilliant evolutionary safety mechanism. It is a highly redundant arterial anastomosis (a ring of communicating blood vessels) located at the very base of the brain. It is formed by the junction of the Anterior Communicating, ACA, Internal Carotid, Posterior Communicating, and PCA.
Function: If one major artery slowly becomes blocked by plaque, the Circle of Willis provides critical collateral circulation, allowing blood to detour around the blockage to keep the brain alive.
Part VIII: Astrocytes (A Crucial Glial Cell)
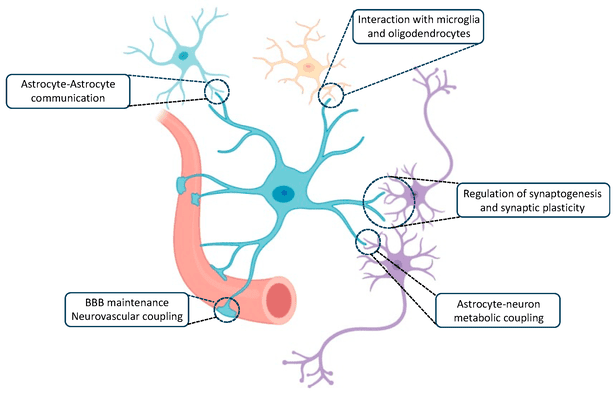
Neurons get all the glory, but they are fragile divas. They cannot survive without Glial Cells (the supporting cast). Astrocytes are star-shaped, incredibly numerous glial cells in the CNS that play a multifaceted, life-or-death role in brain health.
- 1. Create Supportive Framework: They provide a dense, physical scaffolding for neurons, occupying the spaces between them, and helping define specific, protected neuronal territories.
- 2. Create the "Blood-Brain Barrier" (BBB): A supreme function. Astrocytes extend long, specialized arms called "end feet" that tightly wrap around every single microscopic blood capillary in the brain. They physically induce the capillary endothelial cells to weld together with impermeable "tight junctions." This aggressively regulates what substances can cross from the blood into the delicate brain tissue, locking out toxins and bacteria.
- 3. Monitor & Regulate Interstitial Fluid:
- Neurotransmitter Uptake: Astrocytes act like vacuum cleaners. They rapidly suck up dangerous, excess neurotransmitters (like glutamate) from the synaptic cleft to prevent excitotoxicity (which would literally excite neurons to death).
- Ion Homeostasis (Spatial Buffering): They absorb excess Potassium (K+) from the extracellular fluid to maintain perfect electrical firing conditions.
- Metabolic Support: They store glycogen and supply neurons with vital metabolic fuel (lactate).
- 4. Secrete Chemicals: They secrete neurotrophic factors and signaling molecules that physically guide neuronal migration during fetal development and promote synaptogenesis (creating new neural connections).
- 5. Scar Tissue Formation (Gliosis): Unlike the rest of the body, the brain does not use collagen-producing fibroblasts to heal cuts. Instead, after a stroke, trauma, or infection, astrocytes rapidly multiply, enlarge, and undergo reactive astrogliosis. They produce excessive amounts of a protein called GFAP to form a dense glial scar. While this safely walls off the necrotic injury from healthy tissue, it tragically acts as a physical and chemical barrier that permanently prevents severed axons from regenerating.
References
The comprehensive material detailed in this guide is synthesized from foundational neuroembryology and neuroanatomy concepts found within the following highly regarded medical texts:
- Sadler, T. W. (2018). Langman's Medical Embryology (14th ed.). Wolters Kluwer.
- Moore, K. L., Persaud, T. V. N., & Torchia, M. G. (2019). The Developing Human: Clinically Oriented Embryology (11th ed.). Elsevier.
- Crossman, A. R., & Neary, D. (2019). Neuroanatomy: An Illustrated Colour Text (6th ed.). Elsevier.
- Snell, S. R. (2010). Clinical Neuroanatomy (7th ed.). Lippincott Williams & Wilkins.
- Kandel, E. R., Schwartz, J. H., & Jessell, T. M. (2021). Principles of Neural Science (6th ed.). McGraw-Hill Education.