
Introduction to the Musculoskeletal System
By the end of this comprehensive guide, you will be deeply conversant with:
- The structural and functional components of the musculoskeletal system.
- The microscopic and macroscopic anatomy of bone tissue (including cells, composition, and markings).
- The intricate, step-by-step biological processes of bone formation (ossification), growth, and fracture healing.
- A detailed clinical understanding of congenital bone malformations and dysplasias.
1. Overview of the Musculoskeletal System
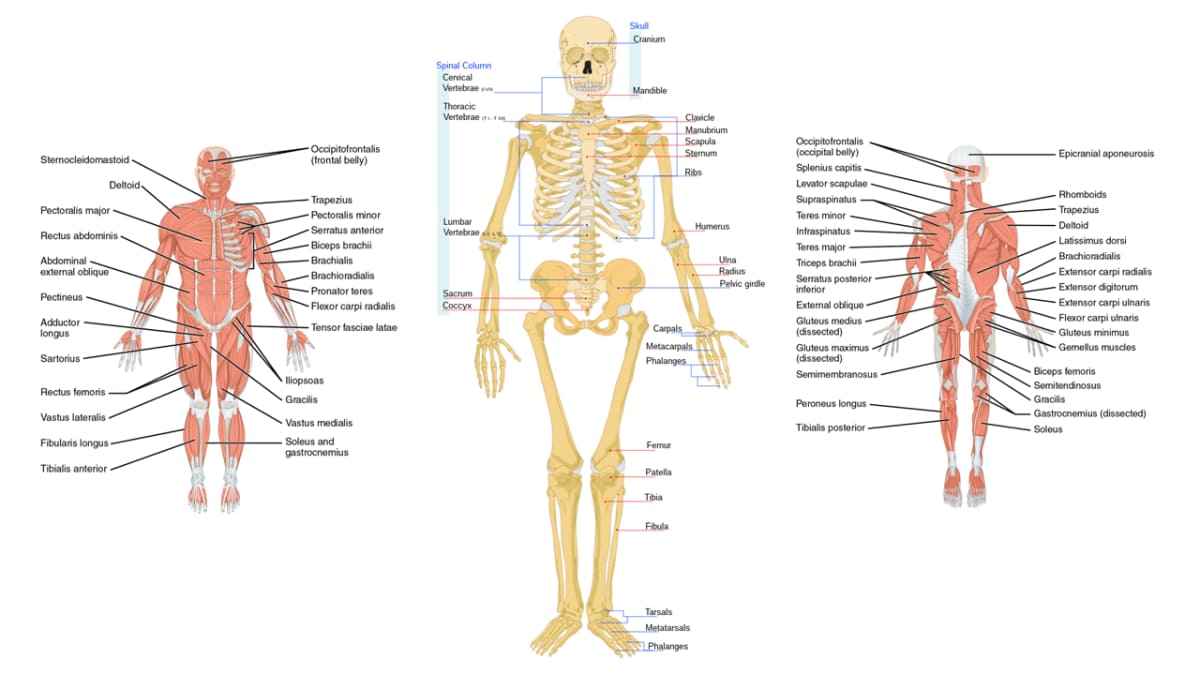
The Human Skeletal system is the remarkable body system composed of bones, cartilage, tendons, ligaments, and other connective tissues that perform essential, life-sustaining functions for the human body. Altogether, the skeleton makes up about 20% of a person's total body weight.
Far from being a dry, static scaffold (like the skeletons seen in Halloween decorations), the musculoskeletal system is highly dynamic, richly vascularized, and constantly remodeling itself to adapt to the physical stresses placed upon it.
Components of the Musculoskeletal System
The rigid organs that form the body's structural framework. The human skeleton is composed of around 270 bones at birth (many of which fuse together during growth, such as the sacrum and cranial bones). The adult human skeleton is composed of exactly 206 bones, which are made of highly specialized connective tissue featuring a mineralized matrix.
A soft, gel-like, avascular connective tissue that protects joints, facilitates smooth movement, and provides flexible support. Detail: It comes in three main types:
- Hyaline Cartilage: The most abundant (covers joint surfaces, nose, trachea).
- Fibrocartilage: The toughest (intervertebral discs, pubic symphysis).
- Elastic Cartilage: The most flexible (external ear, epiglottis).
Strong, tough bands of elastic connective tissue that connect BONE to BONE. They support and strengthen joints, limiting their movement to prevent dislocation and injury. The human body has approximately 900 ligaments.
Clinical Note: An injury where a ligament is overstretched or torn is medically termed a Sprain (e.g., an ankle sprain).
Strong, fibrous bands of dense regular connective tissue that attach MUSCLE to BONE. They act as cables, transmitting the mechanical force generated by muscle contractions to the bones to produce movement. The body has approximately 4,000 tendons.
Clinical Note: An injury where a tendon or muscle is overstretched or torn is termed a Strain.
Specialized contractile tissue attached to bones via tendons. Their voluntary, ATP-driven contraction generates the mechanical force required for all conscious movement, posture maintenance, and heat generation (shivering). The body has about 650 distinct skeletal muscles.
2. Functions of the Musculoskeletal System
The coordinated, harmonious action of these components provides the body with several critical, life-preserving functions.
- Support: The skeleton forms the rigid internal framework that supports the body's weight against gravity and provides its distinct shape. Without it, we would collapse into a shapeless mass of tissue.
- Movement: Bones act as rigid levers, joints act as pivots, and muscles provide the motor force, allowing for locomotion, breathing, and complex manipulation of the environment.
- Protection: The skeleton physically shields delicate, vital internal organs from traumatic injury.
- Examples: The heavily fused cranial bones protect the brain; the rib cage protects the heart and lungs; the vertebrae protect the spinal cord.
- Mineral Storage and Buffering: Bones act as the body's "bank vault" and critical reservoir for essential minerals, predominantly storing 99% of the body's Calcium and 85% of its Phosphate. Bones continuously deposit or release these minerals into the blood to maintain strict systemic electrolyte homeostasis.
- Hematopoiesis (Blood Cell Production): Red bone marrow, found within the spongy bone of certain bones (like the sternum, pelvis, ribs, and the heads of the femur and humerus in adults), is the exclusive site responsible for producing all red blood cells, white blood cells, and platelets.
- Fat Storage: Yellow bone marrow, found primarily in the central medullary cavity of the long bones, stores triglycerides (fat) acting as a significant reserve of chemical energy.
- Endocrine Regulation (Extra Detail): Bone cells release a hormone called Osteocalcin, which helps regulate blood sugar and fat deposition, proving bone is also an endocrine organ!
3. The Microscopic Structure of Bone
Bones are the basic unit of the human skeleton. They are highly vascular, living tissues continuously remodeled throughout life to prevent micro-damage accumulation.
A. Composition of Bone
Bone tissue is a remarkably engineered "composite material." Just like reinforced concrete used in buildings, bone relies on two contrasting materials (organic and inorganic) working together to give it its unique, shatter-resistant properties.
1. Organic Components (~35% of bone mass)
Composed of living cells and Osteoid (the unmineralized, organic matrix). The osteoid is primarily made of highly organized Type I collagen fibers suspended in a ground substance of proteoglycans.
- FUNCTION: Provides profound flexibility, resilience, and tensile strength (resistance to being twisted or pulled apart).
- Analogy: The flexible steel rebar inside a concrete pillar.
- Clinical Path: If a patient lacks normal collagen (as seen in Osteogenesis Imperfecta), the bone loses its flexibility and shatters like glass.
2. Inorganic Components (~65% of bone mass)
Primarily consisting of Hydroxyapatite (a heavily crystallized complex of calcium phosphate) and other tightly packed mineral salts like magnesium, sodium, and fluoride.
- FUNCTION: Provides extreme hardness and compressional strength (ability to withstand heavy crushing weight).
- Analogy: The hard, rock-solid concrete poured over the steel rebar.
- Clinical Path: If a patient lacks calcium/Vitamin D (causing Rickets in children or Osteomalacia in adults), the bone lacks hardness and literally bows/bends under the weight of the body.
B. Types of Bone Tissue: Compact vs. Spongy
At the macroscopic and microscopic level, bone organizes itself into two main structural architectures to balance strength with weight.
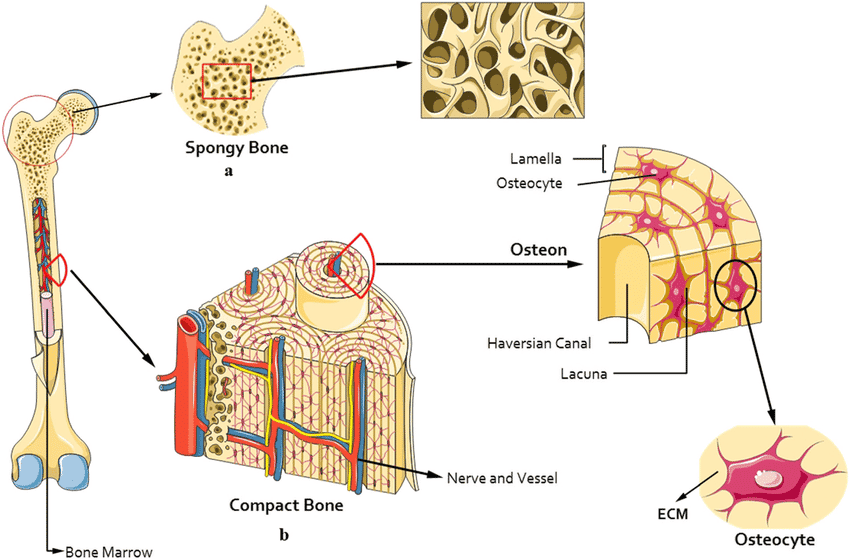
- Compact Bone (Cortical Bone): The dense, solid outer layer.
- Structure: It is highly organized into repeating structural cylinders called Osteons (Haversian systems). Think of them as a bundle of microscopic straws packed tightly together.
- Each osteon consists of concentric tree-ring-like layers called lamellae surrounding a central Haversian canal, which houses the blood vessels and nerves.
- Function: Provides immense strength, protection, and bears the heavy weight of the body. It forms the hard outer shell of all bones and the thick shafts of long bones.
- Spongy Bone (Cancellous / Trabecular Bone): The internal, lightweight tissue.
- Structure: It lacks osteons entirely. Instead, it consists of an irregular, honeycomb-like latticework of thin, branching columns of bone called Trabeculae.
- The open spaces between the trabeculae are not empty; they are packed with red bone marrow (the site of hematopoiesis).
- Function: It allows the skeleton to be remarkably strong but light enough for us to move easily. It also diffuses stress forces. It is found in the bulbous ends of long bones and making up the core of flat bones (like the skull).
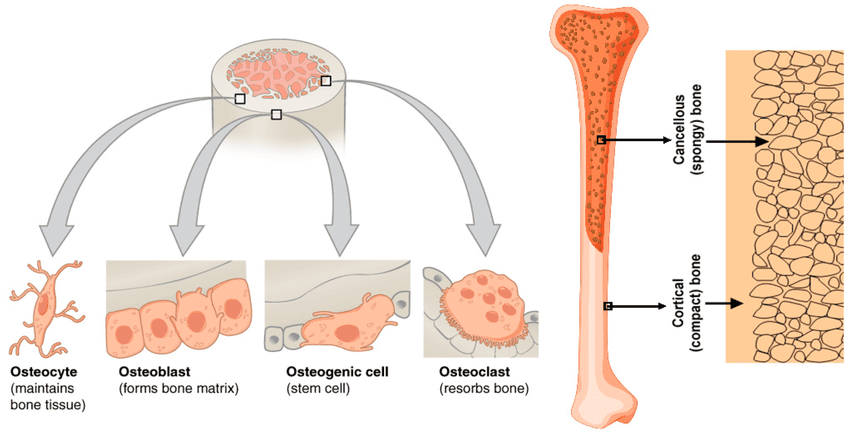
C. The Four Types of Bone Cells
Bone is maintained by a specialized workforce of four cell types acting as a continuous "Bone Remodeling Unit."
Function: The stem cells of the bone. These are unspecialized mesenchymal stem cells that undergo rapid cell division and differentiate (mature) into osteoblasts. They are crucial for bone growth and fracture repair.
Function: The "Bone-Builders" (Remember: OsteoBlasts Build). They synthesize and secrete the soft, organic osteoid matrix and then actively initiate its calcification by pulling calcium from the blood.
Function: Mature, bone-maintaining cells. When an osteoblast gets completely trapped in its own hardened matrix (inside a tiny cave called a lacuna), it becomes an osteocyte. They act as the "managers" or mechanosensors, detecting stress on the bone and signaling osteoblasts or osteoclasts to remodel the area accordingly.
Function: The "Bone-Resorbers" or demolition crew (Remember: OsteoClasts Chew). Derived from white blood cell (macrophage) lineages, these are massive, multi-nucleated cells that secrete highly concentrated hydrochloric acid and powerful lysosomal enzymes to dissolve the bone matrix. This releases trapped calcium back into the bloodstream.
4. The Gross Anatomy of Bone
Now that we've explored bone at the microscopic level, let's examine its larger, more observable features, including its classification, overall structure, and the critical bone markings.
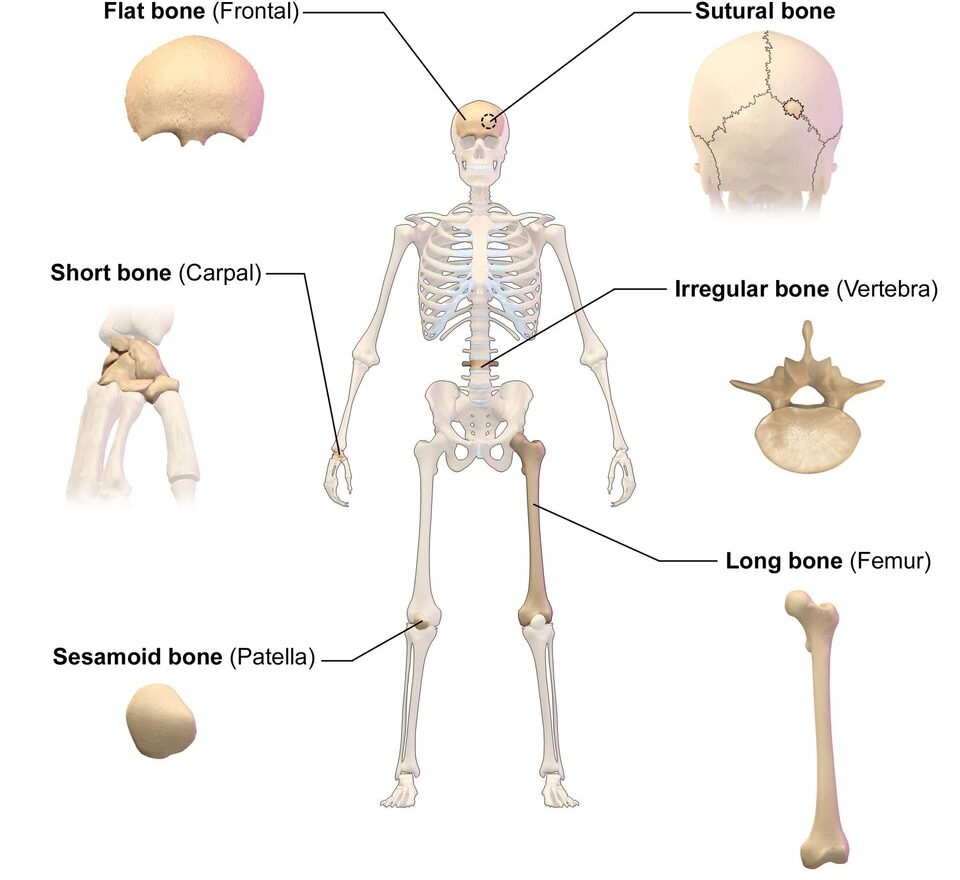
A. Classification of Bones by Shape
- Long Bones: Longer than they are wide. They have a distinct shaft and two ends. They act as levers for gross movement. Examples: Femur (thigh), Humerus (arm), Tibia, Fibula, Phalanges (fingers).
- Short Bones: Roughly cube-shaped; they contain mostly spongy bone and provide stability with limited motion. Examples: Carpals (wrist bones), Tarsals (ankle bones).
- Flat Bones: Thin, flattened, and often slightly curved. They serve as expansive shields providing severe protection, and offer broad surfaces for muscle attachment. Examples: Cranial bones (protecting the brain), Sternum (breastbone), Ribs, Scapulae (shoulder blades).
- Irregular Bones: Complex, bizarre, and varied shapes that don't fit the other categories. Examples: Vertebrae (spinal bones), Hip bones (Os coxae), Sphenoid bone.
- Sesamoid Bones: Small, sesame-seed-shaped bones exclusively embedded within large tendons. They alter the angle of muscle pull and protect the tendon from excessive frictional stress. Examples: Patella (kneecap), Pisiform (in the wrist).
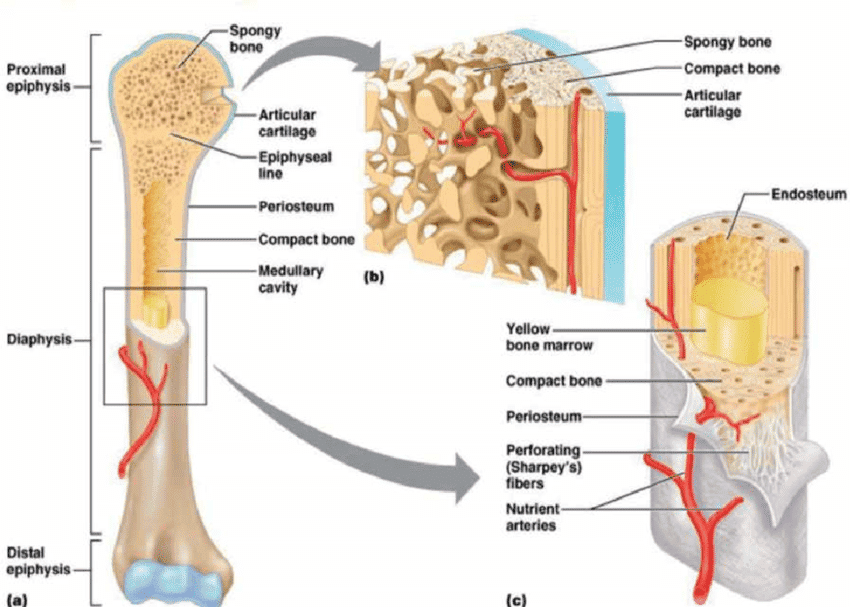
B. Structure of a Long Bone
A typical long bone (like the femur) is the classic model used to study bone anatomy. It consists of specific anatomical regions:
- Diaphysis: The main, long, cylindrical shaft of the bone. It is composed of a thick collar of compact bone surrounding a central hollow space called the medullary cavity (which holds yellow fat marrow).
- Epiphysis: The expanded, bulbous ends of a long bone (proximal and distal). They consist of a thin outer layer of compact bone hiding a massive interior of spongy bone filled with red marrow.
- Metaphysis: The transitional region where the diaphysis and epiphysis meet. In growing children, this contains the epiphyseal plate (a layer of hyaline cartilage allowing the bone to grow longer). In adults, this cartilage ossifies and becomes the epiphyseal line.
- Articular Cartilage: A slick, thin layer of hyaline cartilage covering the epiphysis precisely where it forms a joint with another bone. It absorbs shock and massively reduces friction.
- Periosteum & Endosteum:
- The Periosteum is the tough, double-layered outer membrane covering the entire bone (except at the joints). It is richly supplied with nerve fibers and blood vessels. It is physically anchored to the bone by extremely strong collagen fibers known as Sharpey's fibers.
- The Endosteum is the delicate, thin inner membrane lining the hollow medullary cavity and the trabeculae of spongy bone. Both membranes contain osteoblasts and osteoclasts for remodeling.
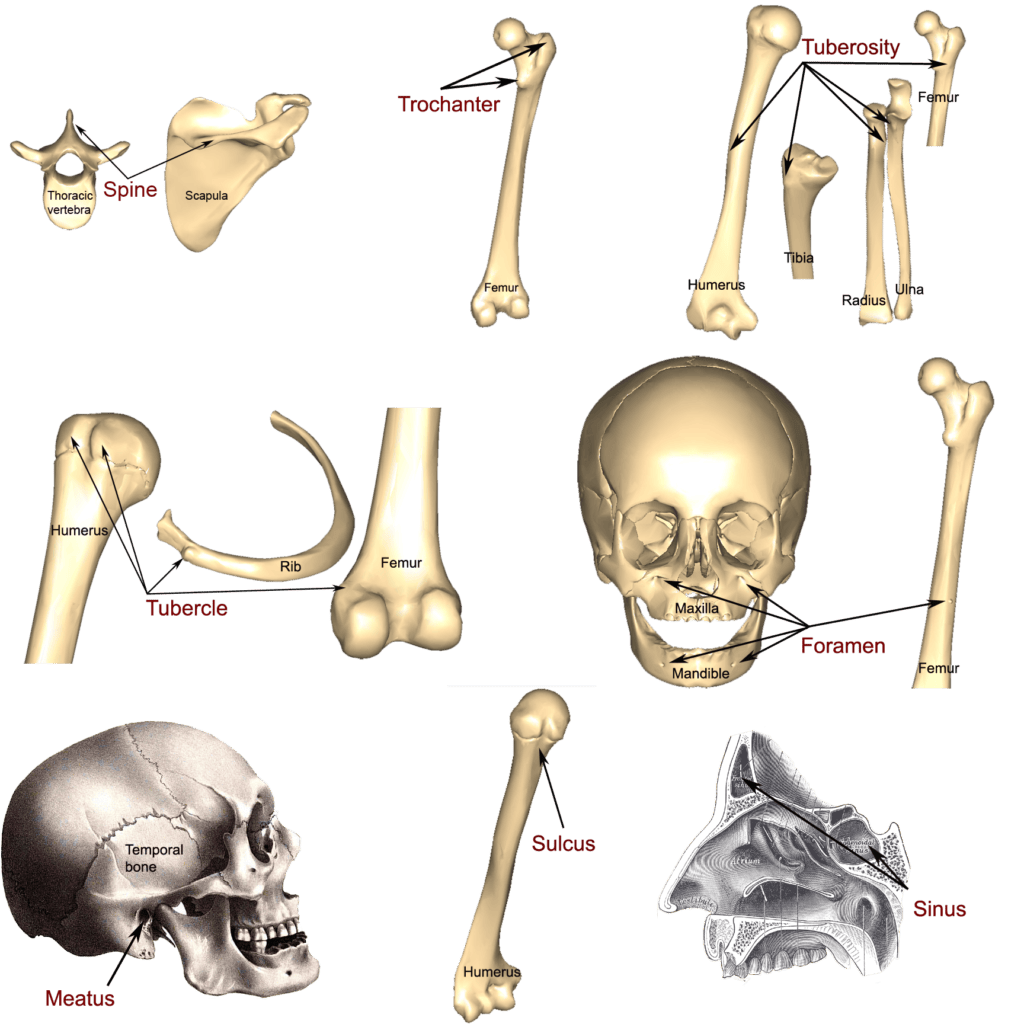
C. Bone Markings (Surface Features)
Bones are rarely perfectly smooth. Bone markings are characteristic projections, depressions, and openings on bone surfaces that serve as points of articulation (joint formation), attachment anchors for muscles and ligaments, or protective passageways for nerves and blood vessels.
1. Projections (Features that Bulge Outward)
| Marking | Description | Classic Example |
|---|---|---|
| Head | Prominent, rounded, ball-like articular surface. | Head of femur, Head of humerus |
| Condyle | Rounded, knuckle-like articular projection. | Occipital condyles, Femoral condyles |
| Epicondyle | Raised area situated directly above a condyle. | Medial epicondyle of the humerus |
| Process | Any generic bony prominence. | Mastoid process, Zygomatic process |
| Spine | Sharp, slender, often pointed projection. | Ischial spine, Spine of the scapula |
| Tubercle | Small, rounded projection or nodule. | Greater tubercle of the humerus |
| Tuberosity | Large, rounded, often roughened projection. | Tibial tuberosity, Deltoid tuberosity |
| Trochanter | Very large, blunt, irregularly shaped process (only found on the femur). | Greater and Lesser trochanter of femur |
| Crest | Narrow, prominent, ridge-like border of bone. | Iliac crest (the "hip bone" you feel on your side) |
| Line | Slight, elongated ridge (less prominent than a crest). | Superior nuchal line, Linea aspera |
| Ramus | Arm-like bar or branch of bone. | Ramus of the mandible (jawbone) |
2. Depressions and Openings (Indentations or Holes)
| Marking | Description | Classic Example |
|---|---|---|
| Fossa | Shallow, basin-like depression, often serving as an articular surface. | Mandibular fossa, Glenoid fossa |
| Fovea | Small pit or tiny depression. | Fovea capitis (on the head of the femur) |
| Sulcus (Groove) | A furrow or channel-like depression for a tendon, nerve, or blood vessel. | Intertubercular sulcus (bicipital groove) |
| Foramen | Round or oval hole right through a bone for nerve/vessel passage. | Foramen magnum (where the spinal cord exits the skull), Mental foramen |
| Meatus | Canal-like, tube-shaped passageway. | External auditory meatus (the ear canal) |
| Fissure | Narrow, slit-like, cleft opening. | Superior orbital fissure (in the back of the eye socket) |
| Sinus | Hollow, air-filled cavity within a bone, lined with mucous membrane. | Frontal, Maxillary, and Paranasal sinuses |
| Facet | Smooth, nearly flat, slightly concave or convex articular surface. | Articular facets of vertebrae |
5. Bone Formation (Ossification / Osteogenesis)
Ossification, also known as osteogenesis, is the remarkable biological process of creating new bone tissue. All bone tissue inherently originates from mesenchyme, a specialized embryonic connective tissue derived from the mesoderm layer of the embryo. Mesenchymal stem cells are multipotent; they can differentiate into both chondroblasts (cartilage-formers) and osteoblasts (bone-builders).
The Two Strategies for Bone Formation
The human body employs two totally distinct methods to construct the skeleton, differing primarily in their initial steps.
- Intramembranous Ossification: The simpler, more direct method where bone is formed directly within a fibrous sheet or "membrane" of mesenchymal tissue. No cartilage template is used.
- Forms: Primarily the flat bones of the skull and face (frontal, parietal, occipital, temporal bones), the mandible, and parts of the clavicle (collarbone).
- Endochondral Ossification: A much more complex, indirect method. A miniature model made entirely of hyaline cartilage is created first. This squishy cartilage model then serves as a scaffold that is systematically destroyed and replaced by hard bone tissue.
- Forms: Almost all other bones from the base of the skull downward, including long bones (femur, humerus), vertebrae, and ribs.
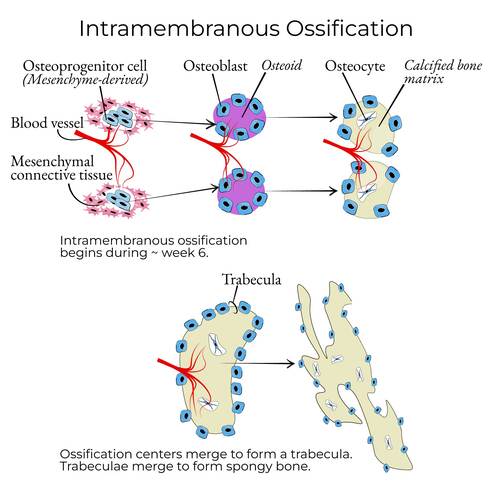
A. Intramembranous Ossification: A Step-by-Step Guide
This process occurs during fetal development (around week 8) and continues into infancy, primarily forming the protective flat bones of the skull.
Step 1: Mesenchymal Cells Condense
In the precise location where a new bone is needed, mesenchymal stem cells begin to cluster closely together and multiply, signaling the start of bone formation.
Analogy: "First, all the mesenchymal stem cells get a text message: 'Party at the skull-in-progress! Be there!' So they all cluster together in one spot."
Step 2: Differentiation and Osteoid Secretion
These clustered mesenchymal cells transform (differentiate) into osteoblasts, officially forming an ossification center. They immediately begin secreting osteoid, the unmineralized, organic collagen matrix that acts as the soft framework for the bone.
Analogy: "These cells change jobs. They become our bone-builders, the Osteoblasts. And what do they do? They start secreting this gooey stuff called osteoid. Think of it as the rebar and mesh before you pour the concrete."
Step 3: Calcification and Trapping of Osteocytes
Calcium salts from the surrounding blood are deposited into the osteoid in a matter of days, making it hard and rigid (calcification). Some osteoblasts become completely surrounded by their own calcified matrix, getting trapped in small spaces called lacunae. Once trapped, they mature into osteocytes, whose new job is to maintain the bone tissue.
Analogy: "Now the concrete truck arrives! Calcium hardens that osteoid. Some of the osteoblast workers are a bit slow and get trapped in their own concrete! They just change jobs again and become Osteocytes—the site managers."
Step 4: Formation of Spongy Bone
The ossification process radiates outward haphazardly, forming tiny, interconnected rods of bone called trabeculae. This creates the characteristic honeycomb structure of spongy (cancellous) bone. Blood vessels weave through the spaces to provide nutrients, and the remaining mesenchymal cells trapped in these spaces differentiate into red bone marrow.
Analogy: "This process keeps spreading out, creating a network of tiny bone struts called trabeculae. It looks like a sponge, which is why we call it spongy bone. Blood vessels sneak into the gaps, and the leftover mesenchyme turns into red bone marrow."
Step 5: Formation of Compact Bone and Periosteum
The surrounding mesenchyme on the outside condenses to form the fibrous periosteum (a protective outer membrane). The spongy bone layer just deep to the periosteum is then heavily remodeled by osteoblasts into a dense, strong layer of compact bone, creating a "sandwich" structure with spongy bone locked in the middle (called diploë in the skull).
Analogy: "Finally, the mesenchyme on the outside forms a tough wrapper called the periosteum. The spongy bone right underneath gets remodeled into super-dense compact bone. So you end up with a bone sandwich: two layers of hard compact bone with a spongy, marrow-filled center."
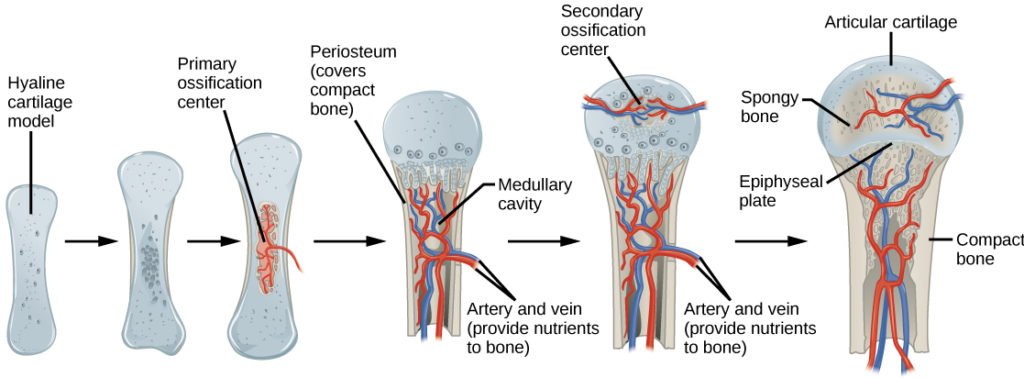
B. Endochondral Ossification: Building on a Cartilage Model
This more intricate, multi-stage process is responsible for the formation and longitudinal growth of most bones in the body, particularly the long bones of the limbs. It crucially relies on a hyaline cartilage model as a precursor.
Step 1: The Hyaline Cartilage Model is Formed
Mesenchymal cells differentiate into chondroblasts, which actively produce a miniature, scaled-down model of the future bone made entirely of hyaline cartilage. This model is surrounded by a fibrous connective tissue membrane called the perichondrium.
Analogy: "First, the body makes a perfect, wobbly model of the bone out of hyaline cartilage. It’s the exact shape of the final bone, just… squishier."
Step 2: Hypertrophy and Calcification in the Center
In the exact center of the diaphysis (the shaft), the cartilage cells (chondrocytes) swell immensely (hypertrophy). This swelling alters their chemical environment and causes the surrounding cartilage matrix to calcify, making it rigid and impenetrable to nutrients.
Analogy: "The cartilage cells right in the middle of the shaft get big and swollen. They get so big they make the area around them hard and chalky. It calcifies."
Step 3: The Periosteal Bone Collar Forms (Primary Ossification Center)
The perichondrium is vascularized by a blood vessel, which triggers the cells to transform into osteoblasts. The perichondrium is now officially the periosteum. These new osteoblasts secrete a thin, rigid cylinder of bone completely around the diaphysis, called the subperiosteal bone collar. This marks the establishment of the Primary Ossification Center.
Analogy: "The outer wrapping sees what’s happening and turns into a periosteum. Its osteoblasts build a thin collar of bone around the middle of the shaft. This is our primary ossification center."
Step 4: Invasion of the Periosteal Bud
Because the calcified cartilage matrix blocks nutrient diffusion, the central, swollen chondrocytes starve to death. As they die, their matrix deteriorates, leaving massive empty cavities. A complex of blood vessels, nerves, red marrow elements, osteoprogenitor cells, and osteoclasts—collectively known as the periosteal bud—invades these central cavities.
Analogy: "The cartilage cells in the middle can't get any food, and they die. Then, the cavalry arrives! A blood vessel called the osteogenic bud drills its way in, bringing the Osteoclasts (demolition team) and more Osteoblasts (construction team)."
Step 5 & 6: Spongy Bone Formation and Medullary Cavity
The invading osteoclasts break down the dead, calcified cartilage. The trailing osteoblasts lay down true new bone matrix on the remaining cartilage remnants, forming early spongy bone. As this primary ossification center rapidly expands towards the ends (epiphyses) of the bone, osteoclasts strictly in the very center resorb the newly formed bone, hollowing it out to carve out the vast medullary (marrow) cavity.
Analogy: "The osteoclasts clear out the dead cartilage, and the osteoblasts build spongy bone. The demolition crew is very efficient, hollowing out the very center of the shaft to create the medullary cavity. It’s a constant cycle of building and carving."
Step 7: Secondary Ossification Centers Appear
Shortly before or after birth, a nearly identical process occurs in the epiphyses (the ends of the bone). Epiphyseal blood vessels invade the swollen, calcified cartilage ends, and spongy bone is formed, creating Secondary Ossification Centers. This transforms the cartilage ends into solid bone, though a layer of articular cartilage remains on the joint surface, and the epiphyseal plate remains between the diaphysis and epiphysis.
Analogy: "After the baby is born, this whole process starts all over again at the ends of the bone, the epiphyses. These are the secondary ossification centers."
6. Bone Growth and Remodeling
A. How Bones Grow in Length (Longitudinal Growth)
The continuous increase in the length of long bones during childhood and adolescence is driven exclusively by the Epiphyseal Growth Plate, a thin, highly active layer of hyaline cartilage caught between the diaphysis and each epiphysis.
This plate is organized into five distinct, microscopic zones of relentless activity (Mnemonic: Real People Have Career Options):
- Zone of Reserve (Resting) Cartilage: Inactive, small chondrocytes that anchor the growth plate securely to the bony epiphysis.
- Zone of Proliferation: Chondrocytes undergo rapid, furious mitosis, forming tall stacks of new cells (like stacks of coins) that literally physically push the epiphysis away from the diaphysis, adding length to the bone.
- Zone of Hypertrophy & Maturation: Older chondrocytes stop dividing and enlarge significantly, leaving large interconnecting spaces.
- Zone of Calcification: The surrounding matrix calcifies, choking off nutrients, and the hypertrophied chondrocytes die.
- Zone of Ossification (Osteogenic zone): Osteoclasts dissolve the dead, calcified cartilage spicules, and osteoblasts swarm in to lay down new spongy bone on the remaining scaffolding, permanently extending the bony diaphysis.
Hormonal Control: During childhood, this process is heavily stimulated by Growth Hormone (GH) and Thyroid Hormones. At the end of puberty, a massive surge of sex hormones (Estrogen and Testosterone) initially causes a rapid growth spurt, but ultimately induces "epiphyseal closure." The cartilage growth completely stops, the plate is entirely replaced by bone (leaving a faint epiphyseal line), and longitudinal growth permanently ceases.
B. How Bones Grow in Width (Appositional Growth)
Bones must also grow in width to become thicker and stronger to support the increasing weight of the growing body. This is called appositional growth, and it can occur throughout life (especially in response to heavy weightlifting). It is a carefully balanced process of addition and subtraction:
- On the Outside (Addition): Osteoblasts in the inner layer of the periosteum secrete new bone matrix onto the external bone surface, increasing the bone's outer diameter.
- On the Inside (Subtraction): Simultaneously, osteoclasts in the endosteum actively resorb (destroy) bone from the inner surface that lines the medullary cavity.
This beautifully coordinated action allows the bone to massively increase in diameter and overall strength without the walls becoming excessively thick, dense, and unmanageably heavy.
7. Bone Healing (Fracture Repair)
Bone healing is a remarkable biological process that follows a highly predictable, four-step sequence to restore the integrity of a broken bone. Unlike soft tissue repair (which often results in weaker scar tissue), bone healing has the unique ability to regenerate true, original bone tissue, often making the healed site stronger than before the break.
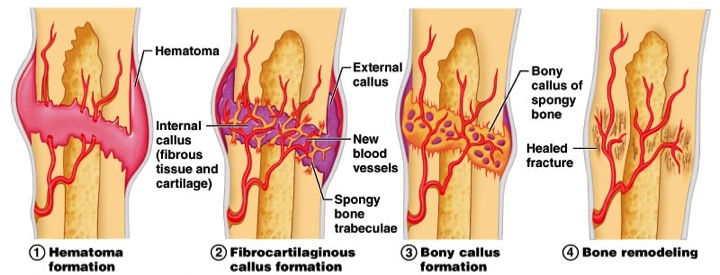
The Four Stages of Fracture Repair
(Inflammatory Stage - Hours to Days)
Immediately after a fracture, torn blood vessels within the bone and periosteum hemorrhage violently, forming a massive, pooling clot of blood called a hematoma at the fracture site. The area becomes intensely swollen, painful, and inflamed. Bone cells deprived of blood nutrition quickly die. Inflammatory cells (macrophages) and osteoclasts flood the area to aggressively clean up the dead cellular debris.
Clinical Note: Giving NSAIDs (like Ibuprofen) too early can actually delay fracture healing, because this initial inflammatory surge is absolutely required to trigger the healing cascade!
(Soft Callus Formation - Days to Weeks)
Within a few days, new capillary blood vessels grow into the clotted hematoma. Fibroblasts from the periosteum invade and produce dense collagen fibers to physically bridge the gap between the broken ends. Simultaneously, chondroblasts secrete a thick, rubbery cartilage matrix. This entire mass of repair tissue—a mix of collagen and cartilage—is known as the fibrocartilaginous (soft) callus, which acts as an internal, natural splint to stabilize the bone ends.
(Hard Callus - Weeks to Months)
As the soft callus forms, osteoblasts migrate to the area and rapidly multiply. They systematically begin replacing the soft fibrocartilage with hard, spongy bone trabeculae. This gradually converts the soft callus into a rigid, bony callus. This process firmly and physically unites the two broken bone fragments, significantly increasing the mechanical strength of the repair site to the point where a clinical cast can often be removed.
(Months to Years)
Over the next several months to years, the bulky, unrefined bony callus is meticulously remodeled by the Bone Remodeling Unit. Osteoclasts shave away excess, bulging material on the outside of the bone shaft and hollow out the interior to re-establish the medullary cavity. Osteoblasts lay down highly organized compact bone to reconstruct the shaft walls. This final phase completely restores the bone to its original shape and mechanical strength, often leaving little to no trace of the original traumatic injury on an X-ray.
Factors Influencing Bone Healing
The success, quality, and speed of fracture repair can be heavily influenced by a variety of local and systemic factors.
- Fracture Severity and Type: Simple, clean, closed fractures heal much more quickly than complex, severely comminuted (shattered), or open (compound/bone sticking through skin) fractures, which have a high risk of bacterial infection.
- Blood Supply: An adequate, robust blood supply is absolutely crucial for delivering the necessary macrophages, osteoblasts, oxygen, and nutrients to the fracture site. Avascular necrosis (bone death due to lack of blood) is a severe complication.
- Immobilization: Proper alignment (reduction) and rigid stabilization (e.g., with a plaster cast, or surgical ORIF - Open Reduction Internal Fixation using plates and screws) are essential to prevent movement that could constantly tear apart the delicate soft callus. Poor immobilization leads to nonunion or malunion.
- Nutrition: A diet exceptionally rich in calcium, vitamin D, vitamin C (required for collagen synthesis), and high-quality protein is vital for providing the building blocks of new bone.
- Age: Children and adolescents generally heal at a dramatically faster rate than adults and the elderly due to higher basal metabolic and osteogenic activity.
- Health Status: Chronic, systemic diseases (like uncontrolled diabetes mellitus), systemic infections, smoking (which causes severe vasoconstriction), and certain medications (e.g., high-dose corticosteroids) can significantly impair or permanently delay the healing process.
- Hormones: Adequate levels of Growth hormone, thyroid hormones, and hormones that regulate calcium (Calcitonin, Parathyroid Hormone - PTH) all play vitally important, supporting roles in bone metabolism and repair.
8. Congenital Bone Malformations
Congenital bone malformations, also known clinically as skeletal dysplasias, are a diverse group of over 400 distinct, rare genetic disorders that severely affect the prenatal development of bones and cartilage. These conditions result in profound abnormalities in the size, density, and shape of the skeleton, affecting approximately 1 in every 5,000 live births.
I. Disorders of Bone Formation (Dysplasias)
These involve abnormal, generalized development of bone or cartilage tissue itself at a cellular level, leading to systemic skeletal defects throughout the entire body.
Achondroplasia
Description: The most common form of short-limbed dwarfism in humans. It is an autosomal dominant genetic disorder caused by a specific gain-of-function mutation in the FGFR3 gene. This mutation effectively acts as an "overactive brake pedal" that severely impairs chondrocyte proliferation in the epiphyseal plate during endochondral ossification. This leads to severely shortened long bones (arms and legs) while the trunk remains relatively normal size. Features also include a prominent forehead (frontal bossing) and a flattened nasal bridge.
Osteogenesis Imperfecta (Brittle Bone Disease)
Description: A group of severe genetic disorders characterized by extremely fragile, weak bones that break or shatter easily, often from mild trauma or even no apparent cause. It is most commonly caused by mutations in the COL1A1 or COL1A2 genes, resulting in defective or severely deficient production of Type I collagen (the "steel rebar" of the bone). Without collagen, the bone is highly brittle. Classic clinical features include frequent childhood fractures, a distinct blue tint to the sclera (the whites of the eyes, due to thin scleral collagen revealing the underlying veins), hearing loss, and dental imperfections.
II. Disorders of Bone Number or Fusion
These embryological errors involve having too many bones, too few bones, or bones that have improperly fused together prematurely.
- Polydactyly & Syndactyly:
- Polydactyly is the physical presence of extra supernumerary fingers or toes.
- Syndactyly is the failure of apoptosis (programmed cell death) between the digits during fetal development, resulting in the fusion of two or more digits (commonly known as "webbed" fingers or toes).
- Spina Bifida:
Description: A severe neural tube defect where the posterior vertebral arches (the bony rings that normally enclose and protect the spinal cord) completely fail to fuse posteriorly during early embryonic development. Severity ranges immensely from mild, asymptomatic forms (spina bifida occulta, often marked only by a tuft of hair on the lower back) to the most severe form (myelomeningocele), where the spinal cord and its protective meninges dangerously protrude outside the baby's back in a fluid-filled sac, often causing lower-limb paralysis and bowel/bladder dysfunction.
- Craniosynostosis:
Description: The abnormal, premature fusion (ossification) of one or more cranial sutures (the fibrous joints between the skull bones) in an infant's skull. Because the skull cannot expand normally at the fused suture, the growing brain forces the skull to expand in other directions, leading to a highly asymmetrical, abnormally shaped head and, if untreated, restricted brain growth and increased dangerous intracranial pressure.
III. Disorders of Limb Development
These are profound embryological disruptions involving massive malformations of the entire limb or significant, missing portions of it.
- Amelia:
Description: The complete and total absence of one or more arms or legs, resulting from a severe, early disruption or failure of the embryonic limb bud development around the 4th week of gestation.
- Phocomelia:
Description: An extremely rare congenital deformity where the hands or feet are attached abnormally close to the main trunk of the body, with the proximal limbs (arms and thighs) being vastly reduced in size or entirely absent (resembling the flippers of a seal). This condition is historically and tragically most notably associated with maternal exposure to the drug Thalidomide during early pregnancy in the 1950s and 60s.
IV. Genetic Syndromes with Skeletal Manifestations
Many complex genetic syndromes inherently include skeletal abnormalities as merely one part of a much broader, multi-systemic clinical picture.
Marfan Syndrome
Description: An autosomal dominant connective tissue disorder caused by a deleterious mutation in the FBN1 gene, which encodes the essential glycoprotein fibrillin-1. Because fibrillin is crucial for the integrity of connective tissue everywhere, the disease affects multiple systems.
Skeletal features are prominent and classic: Affected individuals exhibit unusually tall stature, excessively long limbs, and abnormally long, spider-like fingers (arachnodactyly). They also frequently present with highly hypermobile, flexible joints, severe curvature of the spine (scoliosis), and distinct chest wall deformities (such as pectus excavatum - a sunken chest, or pectus carinatum - a pigeon chest). Furthermore, they face massive, potentially fatal cardiovascular complications, notably progressive dilation and sudden tearing (dissection) of the aorta.
List of References
- Standring, S. (2020). Gray's Anatomy: The Anatomical Basis of Clinical Practice (42nd ed.). Elsevier. (Definitive reference for gross bone anatomy, structural classifications, and embryological bone development).
- Hall, J. E., & Hall, M. E. (2020). Guyton and Hall Textbook of Medical Physiology (14th ed.). Elsevier. (Core reference for the physiology of bone remodeling, calcium homeostasis, and the endocrine functions of bone).
- Mescher, A. L. (2021). Junqueira's Basic Histology: Text and Atlas (16th ed.). McGraw-Hill Education. (Detailed microscopic structures of osteons, trabeculae, bone cellular lineage, and the precise steps of intramembranous and endochondral ossification).
- Kumar, V., Abbas, A. K., & Aster, J. C. (2020). Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier. (Comprehensive clinical pathology of fracture healing mechanisms, osteogenesis imperfecta, achondroplasia, and Marfan syndrome).
- Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2017). Clinically Oriented Anatomy (8th ed.). Lippincott Williams & Wilkins. (Practical clinical correlations involving bone markings, sprains, strains, and common congenital malformations like spina bifida and craniosynostosis).
- Waugh, A., & Grant, A. (2018). Ross & Wilson Anatomy and Physiology in Health and Illness (13th ed.). Elsevier. (Foundational overview of the musculoskeletal system functions, components, and cellular actions).