
Muscles of the Axial Skeleton & The Cranial Nerves
The axial skeleton forms the central axis of the human body, consisting of the skull, vertebral column, and thoracic cage. The muscles attached to this axis are fundamental for life—they allow us to express emotion, eat, breathe, maintain our posture, and protect our vital organs. By the end of this exhaustive module, you will be able to:
- Identify and categorize the muscles of the head, face, neck, and torso based on their anatomical location.
- Understand the precise origin, insertion, and innervation of each major axial muscle.
- Relate muscular actions to activities of daily living (ADLs) and recognize clinical pathologies associated with muscular dysfunction.
- Master the 12 Cranial Nerves, including their functional types, assessment methods, and clinical relevance.
A. Muscles of the Head and Face
The muscles of the head are unique compared to the rest of the body. They can be broadly categorized into two highly specialized functional groups: the muscles of facial expression and the muscles of mastication (chewing). Understanding these groups is vital for neurological assessments and diagnosing conditions like strokes or nerve palsies.
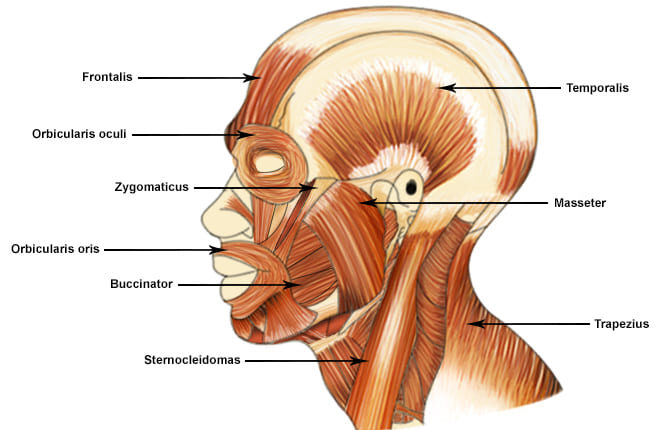
1. Muscles of Facial Expression
Unlike most skeletal muscles that connect bone to bone, these unique muscles frequently originate from the skull and insert directly into the skin or other muscles. This anatomical quirk allows them to tug on the skin, enabling us to show a vast, nuanced range of non-verbal emotions. They are all innervated by the Facial Nerve (Cranial Nerve VII).
A broad, continuous musculofibrous layer covering the top of the skull. It consists of two bellies connected by a broad tendinous sheet called the galea aponeurotica.
- Action: The Frontal belly raises the eyebrows and horizontally wrinkles the forehead skin (the classic expression of surprise or fright). The Occipital belly anchors and pulls the scalp posteriorly.
- Clinical/Daily Example: Raising your eyebrows when you hear shocking news. Tension in the galea aponeurotica is a common cause of tension headaches.
A complex, sphincter-like ring muscle encircling the entire orbit (eye socket).
- Action: Its primary action is to close the eye. The inner (palpebral) part closes it gently (blinking, sleeping), while the outer (orbital) part closes it forcefully (squinting, winking).
- Clinical/Daily Example: Squeezing your eyes shut when walking into a dust storm or facing bright sunlight. In Bell's Palsy (CN VII damage), the patient cannot close the eye, leading to severe dry eye (exposure keratitis).
The complex, multi-layered sphincter muscle encircling the mouth. It is the "kissing muscle."
- Action: It closes, compresses, and protrudes the lips. It shapes the lips during speech.
- Clinical/Daily Example: Puckering up for a kiss, playing a brass instrument like a trumpet, or drinking from a straw. Paralysis here causes drooling and slurred speech (dysarthria).
These diagonal muscles extend from the zygomatic bone (cheekbone) down to the corner of the mouth.
- Action: They are the primary "smiling" muscles, actively raising the lateral corners of the mouth upward and outward.
- Clinical/Daily Example: A genuine, joyful smile (often called a Duchenne smile) strongly engages the Zygomaticus Major alongside the Orbicularis Oculi.
A thin, flat, deep muscle forming the muscular wall of the cheek. Its name derives from the Latin word for "trumpeter."
- Action: It forcefully compresses the cheek against the teeth. It is vital for whistling, sucking, and holding food safely between the teeth during chewing so you don't bite your own cheek.
- Clinical/Daily Example: Infants rely heavily on the buccinator to suckle milk. Glassblowers and musicians use it to expel air forcefully.
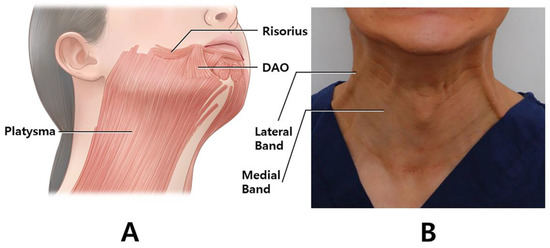 f. Platysma
f. Platysma
A broad, superficial, paper-thin sheet of muscle in the anterior neck, originating from the chest fascia and inserting into the mandible.
- Action: It tenses the skin of the neck, depresses the mandible (opens the jaw slightly), and pulls the lower lip down and back.
- Clinical/Daily Example: The expression of sudden horror or extreme fright. It is also the muscle men instinctively tense when shaving the front of their neck to create a flat surface.
2. Muscles of Mastication (Chewing)
These four powerful pairs of muscles are responsible for moving the mandible (lower jaw) at the Temporomandibular Joint (TMJ) for chewing, grinding, and speaking. Unlike facial expression muscles, they are all heavily innervated by the Mandibular division of the Trigeminal Nerve (Cranial Nerve V3).
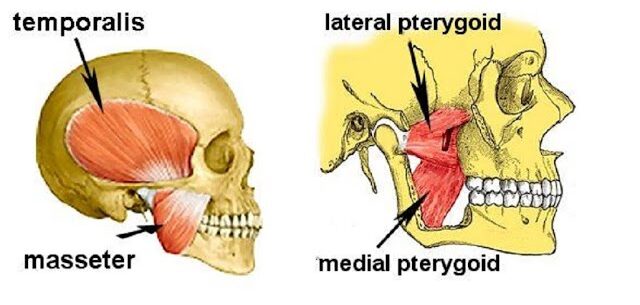
A thick, extremely powerful, quadrilateral muscle covering the lateral side of the jaw.
- Action: It is the prime elevator of the mandible (forcefully closes the jaw).
- Clinical/Daily Example: Biting down hard on a tough piece of steak. Bruxism (nighttime teeth grinding) causes the masseter to become severely hypertrophied (enlarged) and painful.
A large, fan-shaped muscle filling the temporal fossa on the side of the skull, passing deep to the zygomatic arch.
- Action: Elevates the mandible (closes jaw) and its posterior fibers actively retract the mandible (pull it backward).
- Clinical/Daily Example: If you place your fingers on your temples and clench your teeth, you will feel this muscle bulge. Tension here is a massive contributor to stress headaches.
Located deep inside the jaw, mirroring the masseter on the internal surface of the mandible.
- Action: Elevates the jaw synergistically with the masseter and assists in side-to-side (excursive) grinding movements.
- Clinical/Daily Example: The circular, side-to-side grinding motion used when chewing tough plant fibers or gum.
A short, thick, two-headed muscle located deep and horizontally in the jaw. It is the functional oddball of the group.
- Action: It protracts the mandible (pulls it forward), moves it side-to-side, and is the ONLY muscle of mastication that helps OPEN (depress) the jaw.
- Clinical/Daily Example: Thrusting your lower jaw forward to create an underbite, or opening your mouth wide to bite an apple. TMJ disorders often involve spasms of the lateral pterygoid.
Summary Table of Head & Face Muscles
| Muscle | Origin | Insertion | Action |
|---|---|---|---|
| FACIAL EXPRESSION (Innervation: CN VII - Facial Nerve) | |||
| Occipitofrontalis | Galea aponeurotica (Frontal); Occipital bone (Occipital) | Skin of eyebrows; Galea aponeurotica | Raises eyebrows, wrinkles forehead, pulls scalp backward |
| Orbicularis Oculi | Frontal and maxillary bones (medial orbit) | Tissue of eyelid | Closes eye forcefully or gently, squints, blinks |
| Orbicularis Oris | Maxilla and mandible (indirectly via surrounding muscles) | Skin and muscle at angles of mouth | Closes and protrudes lips (puckering, kissing, whistling) |
| Zygomaticus Major/Minor | Zygomatic bone (Cheekbone) | Skin and muscle at angle of mouth | Raises lateral corners of mouth (smiling, laughing) |
| Buccinator | Molar region of maxilla and mandible | Orbicularis oris | Compresses cheek against teeth (whistling, sucking, chewing) |
| Platysma | Fascia of chest (pectoralis and deltoid) | Base of mandible; skin at corner of mouth | Tenses skin of neck, depresses mandible, expresses horror |
| MASTICATION (Innervation: CN V3 - Mandibular Branch of Trigeminal) | |||
| Masseter | Zygomatic arch | Angle and lateral ramus of mandible | Prime elevator of mandible (closes jaw forcefully) |
| Temporalis | Temporal fossa | Coronoid process of mandible | Elevates and retracts mandible |
| Medial Pterygoid | Sphenoid and palatine bones | Medial surface of ramus of mandible | Elevates mandible, assists in side-to-side grinding |
| Lateral Pterygoid | Sphenoid bone (Greater wing and lateral plate) | Condylar process of mandible; TMJ capsule | Protracts and depresses (OPENS) jaw, side-to-side movement |
B. Muscles of the Neck
The muscles of the neck are highly diverse. They are responsible for moving the heavy head, stabilizing the fragile cervical spine, assisting in breathing (respiration), and facilitating the complex internal mechanics of swallowing (deglutition) and speech (phonation). They are categorized here based on anatomical location and their functional primary actions.
1. Superficial Anterior Neck Muscles
- Sternocleidomastoid (SCM)
A prominent, large, two-headed muscle on each anterolateral side of the neck. It is a major anatomical landmark dividing the neck into anterior and posterior triangles.
Action: When acting alone (unilaterally), it rotates the head to the opposite side and laterally flexes it to the same side. When both act together (bilaterally), they powerfully flex the neck (pulling the chin to the chest).
Clinical Example: Torticollis (Wryneck) is a condition where the SCM is in chronic spasm, forcing the patient's head to be tilted and rotated painfully. It is also an accessory muscle of breathing during respiratory distress.
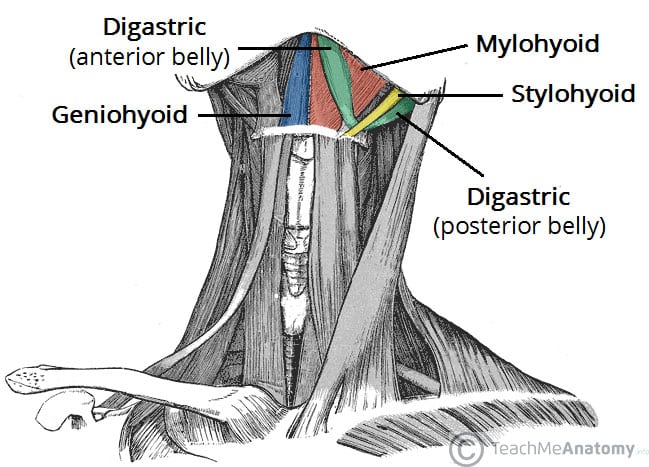
2. Suprahyoid Muscles (Above the Hyoid Bone)
These muscles are located superior to the hyoid bone, forming the physical floor of the mouth. They are primarily responsible for elevating the hyoid bone and widening the esophagus during the initial, voluntary phase of swallowing and speaking.
- a. Digastric: A unique two-bellied muscle (anterior and posterior bellies) connected by a central tendon. It acts to elevate the hyoid during swallowing, or if the hyoid is fixed, it strongly depresses the mandible (opens the mouth wide, like yawning).
- b. Mylohyoid: A flat, triangular muscle that physically forms the sling-like floor of the mouth. It elevates the hyoid and forces the tongue upward to push food back into the throat.
- c. Geniohyoid: A narrow muscle located deep to the mylohyoid. It elevates and strongly protracts (pulls forward) the hyoid bone.
- d. Stylohyoid: A slender muscle running parallel to the posterior digastric belly. It elevates and retracts (pulls backward) the hyoid bone, elongating the floor of the mouth.
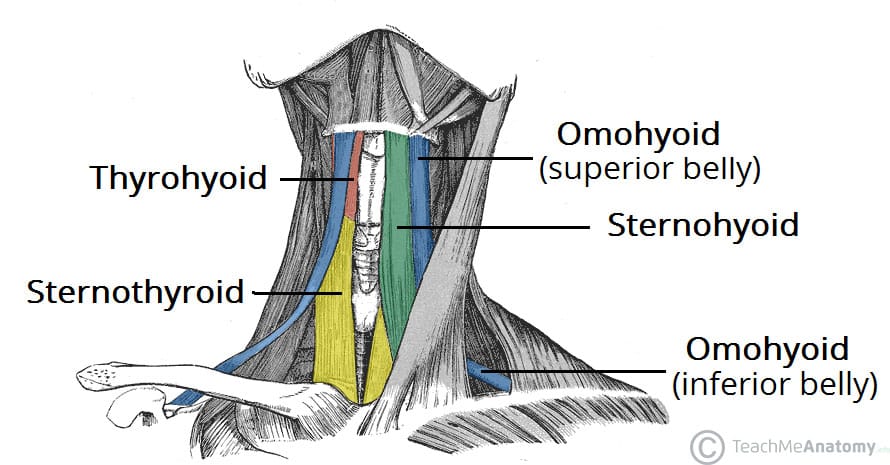
3. Infrahyoid Muscles (Strap Muscles - Below the Hyoid)
These "strap-like" muscles are located inferior to the hyoid bone. Their main physiological job is to depress the hyoid bone and larynx, returning them to their resting positions *after* the act of swallowing or speaking is complete. They act like biological bungee cords.
- a. Sternohyoid: The most superficial strap muscle. It depresses the hyoid bone and larynx after elevation.
- b. Omohyoid: A two-bellied muscle (superior and inferior bellies) that originates all the way from the scapula. It acts to depress and retract the hyoid.
- c. Sternothyroid: Located deep to the sternohyoid. It specifically depresses the larynx (voice box) and the hyoid bone, crucial for altering vocal pitch (e.g., singing low notes).
- d. Thyrohyoid: Acts to depress the hyoid bone, but uniquely, if the hyoid is fixed, it actually elevates the larynx to help close the airway during swallowing to prevent choking.
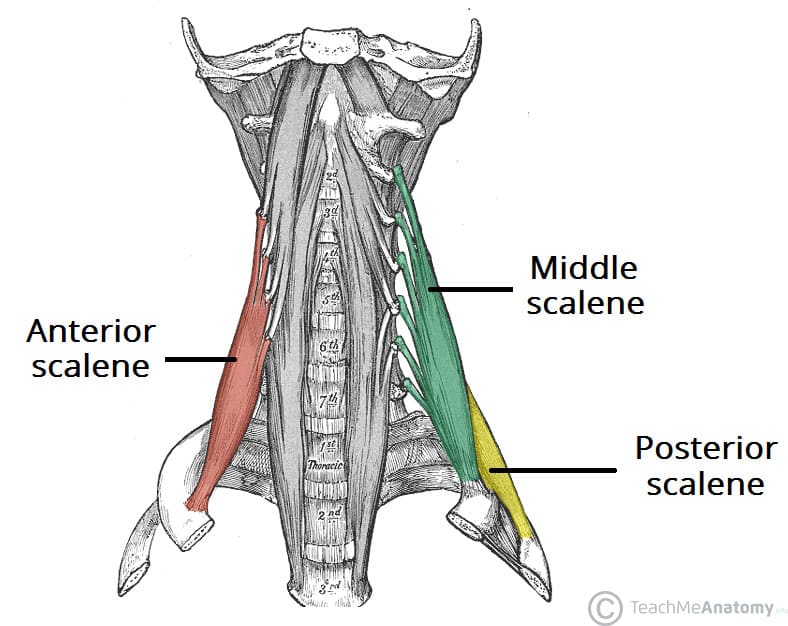
4. Deep Lateral Neck Muscles (Scalenes)
- Scalene Group (Anterior, Middle, and Posterior)
Located deep on the sides of the neck, attached to the cervical vertebrae and the top ribs.
Action: Their primary action is lateral flexion of the neck. However, because they attach to the first two ribs, they act as major accessory muscles of inspiration by elevating the rib cage.
Clinical Example: In severe asthma or COPD, you will see a patient's neck muscles visibly straining (Scalene retractions) as they fight to pull the rib cage open for air. Furthermore, tightness here can compress the brachial plexus nerves, leading to Thoracic Outlet Syndrome (numbness/tingling in the arm).
Summary Table of Neck Muscles
| Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
| Sternocleidomastoid | Manubrium of sternum & medial Clavicle | Mastoid process of temporal bone | Spinal Accessory (CN XI), C2-C3 | Unilateral: Rotates head to opposite side, flexes same side. Bilateral: Flexes neck. |
| Digastric | Mandible (anterior) & Mastoid process (posterior) | Hyoid bone (via fascial sling) | CN V3 (anterior) & CN VII (posterior) | Elevates hyoid during swallowing; depresses mandible to open mouth wide. |
| Mylohyoid | Medial surface of Mandible | Hyoid bone & median raphe | CN V3 (Mandibular nerve) | Forms mouth floor; elevates hyoid & floor of mouth during swallowing. |
| Sternohyoid | Manubrium & medial Clavicle | Inferior border of Hyoid bone | Ansa cervicalis (C1-C3) | Depresses hyoid and larynx after swallowing. |
| Omohyoid | Superior border of Scapula | Inferior border of Hyoid bone | Ansa cervicalis (C1-C3) | Depresses and retracts hyoid. |
| Sternothyroid | Posterior surface of Manubrium | Thyroid cartilage of Larynx | Ansa cervicalis (C1-C3) | Depresses larynx and hyoid (lowers vocal pitch). |
| Thyrohyoid | Thyroid cartilage of Larynx | Inferior border of Hyoid bone | C1 spinal nerve (via CN XII) | Depresses hyoid; if hyoid is fixed, elevates larynx. |
| Scalenes (Ant, Mid, Post) | Transverse processes of Cervical vertebrae (C2-C7) | First & Second ribs | Cervical spinal nerves | Laterally flexes neck; elevates ribs 1 & 2 for forced inspiration. |
C. Muscles of the Torso (Trunk)
The muscles of the trunk form the vital core cylinder of the body. They are absolutely critical for maintaining bipedal posture, protecting soft internal organs without bone coverage (the abdomen), facilitating the pressure changes needed for respiration, and enabling a highly dynamic range of physical movements.
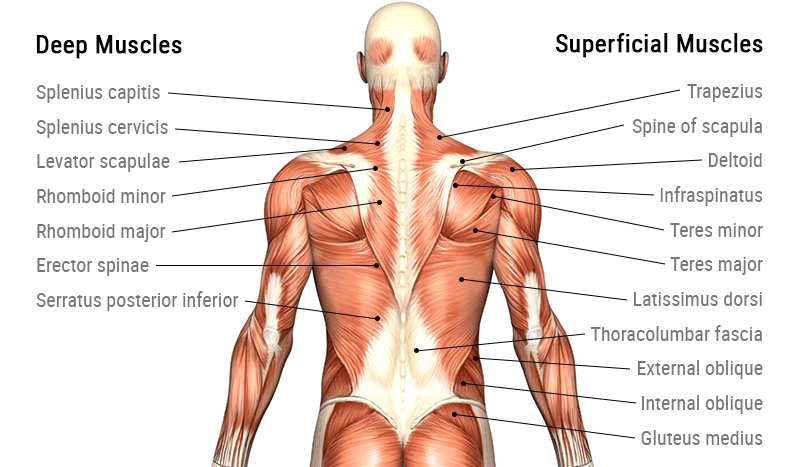
1. Muscles of the Back
These complex, heavily layered muscles move and stabilize the vertebral column, head, and the shoulder girdle.
- a. Superficial Back Muscles (The Appendicular Movers):
Though located on the back, these primarily act to move the upper limbs.- Trapezius: A massive kite-shaped muscle covering the upper back. It moves the scapula (shoulder blade). Example: Shrugging your shoulders (elevation), pulling shoulders back for posture (retraction).
- Latissimus Dorsi: The widest muscle in the human body. Example: The prime mover for a swimmer pulling through the water, or doing a pull-up (extends, adducts, and medially rotates the arm).
- Rhomboids & Levator Scapulae: Deeper muscles that retract and elevate the scapula, keeping the shoulders squared.
- b. Intermediate Back Muscles (The Respiratory Assistants):
Thin muscles that attach to the ribs to assist in the mechanics of breathing.- Serratus Posterior Superior: Elevates ribs to help with inspiration.
- Serratus Posterior Inferior: Depresses ribs to assist in forced expiration.
- c. Deep (Intrinsic) Back Muscles (The Postural Core):
Responsible for the posture and movement of the vertebral column itself.- Erector Spinae Group: A massive column of muscle flanking the spine (consisting of the Iliocostalis, Longissimus, and Spinalis). It is the prime mover of back extension. Clinical Example: Spraining this muscle group during a heavy deadlift or improper lifting technique is the most common cause of lower back pain.
- Transversospinalis Group: Deeper still, these short muscles connect individual vertebrae, stabilizing the spine and providing fine rotational movements.
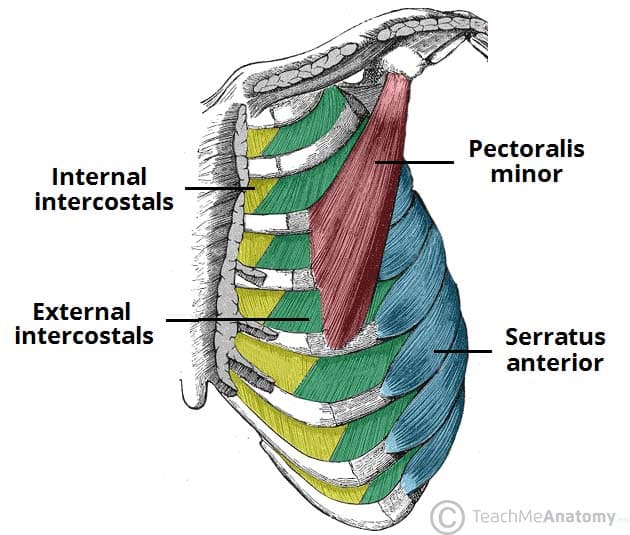
2. Muscles of the Thorax (Chest Wall)
These muscles are primarily dedicated to altering the volume of the thoracic cavity, making the mechanics of breathing (ventilation) possible.
- a. Intercostal Muscles: Located *between* the ribs.
- External Intercostals: Their fibers run down and inward. They elevate the ribs like a bucket handle to expand the chest for inspiration.
- Internal and Innermost Intercostals: Their fibers run down and outward. They forcefully depress the ribs, shrinking the chest cavity for forced expiration (like blowing out a candle).
- b. Diaphragm:
The absolute primary muscle of respiration. It is a large, dome-shaped muscular and tendinous sheet that perfectly separates the thoracic and abdominal cavities.
Action: When it contracts, the dome flattens, dropping inferiorly. This dramatically increases thoracic volume and decreases thoracic pressure, sucking air into the lungs.
Clinical Example: Hiccups are involuntary, spasmodic contractions of the diaphragm. A spinal cord injury at or above C3 can cause respiratory paralysis because the Phrenic nerve (C3, C4, C5 "keeps the diaphragm alive") is severed.
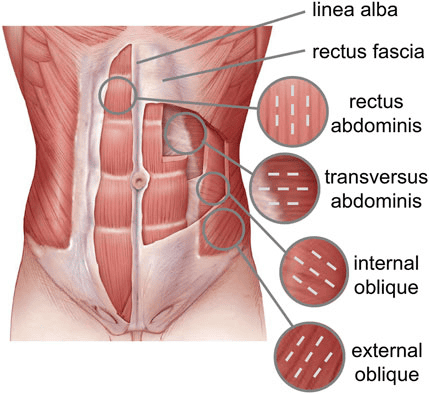
3. Muscles of the Abdominal Wall
Because the abdomen lacks skeletal protection (like ribs), it relies entirely on a muscular corset. These muscles protect viscera, flex the trunk, and perform the Valsalva maneuver (compressing the abdomen to increase intra-abdominal pressure for defecation, urination, vomiting, and childbirth).
The famous vertical "six-pack" muscle running straight down the front. It is segmented by connective tissue bands called tendinous intersections.
- Action: It is the powerful primary flexor of the vertebral column.
- Daily Example: Performing a sit-up or a crunch.
Three distinct layers of flat muscles wrapping the sides of the abdomen like plywood for immense structural integrity.
- External Oblique: Outermost; fibers run down and in (like hands in pockets). Rotates the trunk.
- Internal Oblique: Middle; fibers run up and in. Flexes and rotates the trunk.
- Transversus Abdominis: Deepest; fibers run horizontally. Acts like a tight weightlifting belt to suck in the gut and compress abdominal contents.
A deep, thick, square-shaped muscle forming the posterior abdominal wall next to the spine.
- Action: Unilaterally, it laterally flexes the trunk (bends you sideways) and elevates the hip ("hip hiking").
- Clinical Example: Extremely tight QL muscles are a frequent, hidden cause of severe chronic lower back pain and pelvic tilting.
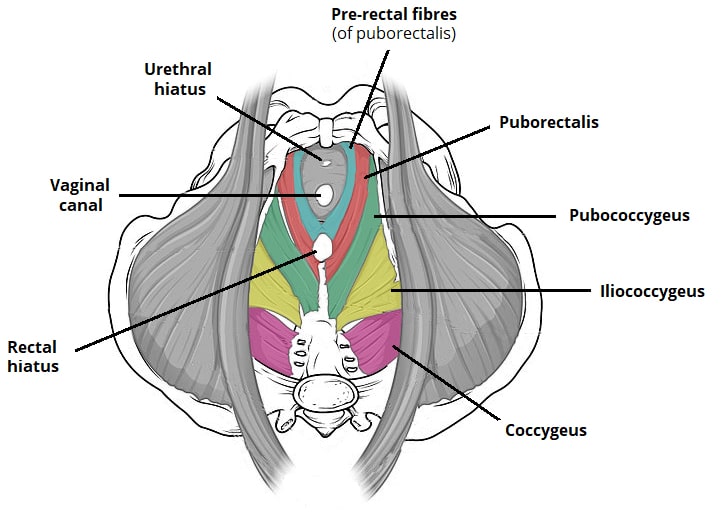
4. Pelvic Floor Muscles (Pelvic Diaphragm)
These muscles close the inferior outlet (the bottom hole) of the bony pelvis. They act as a supportive hammock.
- Levator Ani Group & Coccygeus:
This broad, highly important, funnel-shaped muscle group forms the major part of the pelvic floor.
Action: It physically supports all the heavy pelvic organs (bladder, uterus, rectum) and constantly resists increases in intra-abdominal pressure (when you cough or sneeze). It contains the sphincters that control urinary and fecal continence.
Clinical Example: Weakness in the Levator Ani (often due to trauma from vaginal childbirth) leads to urinary incontinence (leaking urine when coughing) or pelvic organ prolapse (where the uterus drops down). Medical professionals prescribe "Kegel exercises" to specifically strengthen this muscle group.
Summary Table of Torso Muscles
| Muscle | Origin | Insertion | Innervation | Main Actions |
|---|---|---|---|---|
| BACK MUSCLES | ||||
| Trapezius | Occipital bone, Ligamentum nuchae, C7-T12 spinous processes | Clavicle, acromion, spine of scapula | Spinal Accessory (CN XI), C3-C4 | Elevates, retracts, depresses, and upwardly rotates the scapula |
| Latissimus Dorsi | T7-L5 spinous processes, iliac crest, thoracolumbar fascia | Intertubercular groove of humerus | Thoracodorsal Nerve (C6-C8) | Prime mover of arm extension; adducts and medially rotates arm |
| Erector Spinae Group | Iliac crest, sacrum, lumbar/thoracic spinous processes | Ribs, thoracic/cervical vertebrae, mastoid process | Dorsal rami of spinal nerves | Prime mover of back extension; laterally flexes vertebral column |
| THORACIC MUSCLES | ||||
| External Intercostals | Inferior border of rib above | Superior border of rib below | Intercostal nerves (T1-T11) | Elevate ribs (widens chest for inspiration) |
| Internal Intercostals | Superior border of rib below | Inferior border of rib above | Intercostal nerves (T1-T11) | Depress ribs (shrinks chest for forced expiration) |
| Diaphragm | Xiphoid process, costal cartilages, lumbar vertebrae | Central tendon | Phrenic Nerves (C3-C5) | Primary muscle of inspiration; flattens to expand thoracic volume |
| ABDOMINAL & PELVIC MUSCLES | ||||
| Rectus Abdominis | Pubic crest and symphysis | Xiphoid process, costal cartilages 5-7 | Intercostal nerves (T7-T12) | Powerfully flexes vertebral column, compresses abdomen |
| External Oblique | Lower 8 ribs (Ribs 5-12) | Linea alba, pubic tubercle, iliac crest | Intercostal nerves (T7-T12) | Flexes vertebral column, rotates trunk to opposite side |
| Internal Oblique | Thoracolumbar fascia, iliac crest, inguinal ligament | Linea alba, pubic crest, last 3 ribs (10-12) | Intercostal (T7-T12), Iliohypo/inguinal (L1) | Flexes vertebral column, rotates trunk to same side |
| Transversus Abdominis | Thoracolumbar fascia, iliac crest, inner cartilages of ribs 7-12 | Linea alba, pubic crest | Intercostal (T7-T12), Iliohypo/inguinal (L1) | Compresses abdominal contents (increases intra-abdominal pressure) |
| Quadratus Lumborum | Iliac crest and iliolumbar ligament | Last rib (Rib 12), transverse processes of L1-L4 | Lumbar Plexus (T12-L4) | Laterally flexes vertebral column; maintains upright posture |
| Levator Ani Group | Posterior body of pubis, ischial spine | Coccyx, walls of pelvic organs (prostate/vagina/rectum) | Pudendal Nerve (S2-S4), Direct S3-S4 branches | Supports pelvic organs, maintains fecal and urinary continence |
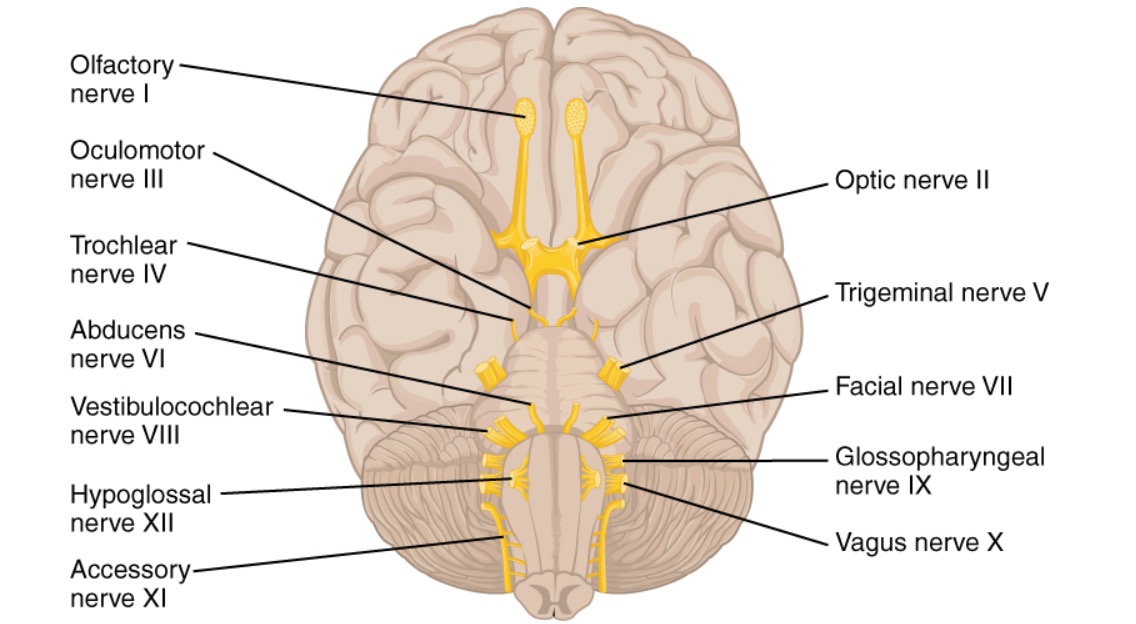
Reference: The 12 Cranial Nerves
The cranial nerves are an absolute cornerstone of neurological anatomy. They are a set of 12 paired nerves that arise directly from the brain and brainstem, bypassing the spinal cord entirely. They are uniquely responsible for conveying special sensory (vision, hearing), general sensory, and complex motor information to and from the head and neck region, as well as controlling vast parasympathetic visceral functions.
Crucial Mnemonics for Memorization
Medical students rely heavily on mnemonics to rapidly recall the order and functional type of the 12 cranial nerves.
- For Nerve Names (I through XII):
"Oh Oh Oh To Touch And Feel A Girls Vagina Ah Heaven"
(Olfactory, Optic, Oculomotor, Trochlear, Trigeminal, Abducens, Facial, Auditory/Vestibulocochlear, Glossopharyngeal, Vagus, Accessory, Hypoglossal). - For Functional Type (S=Sensory, M=Motor, B=Both):
"Some Say Marry Money, But My Brother Says Big Brains Matter More"
Deep Dive: The 12 Cranial Nerves
- I. Olfactory Nerve (Sensory)
Function: Dedicated solely to the special sense of smell (olfaction). It bypasses the thalamus and goes directly to the olfactory cortex.
Clinical Test & Pathology: Ask the patient to identify non-irritating, common scents (e.g., coffee, soap, vanilla) with their eyes closed and one nostril blocked at a time. Total loss of smell is called Anosmia, common in severe head trauma (shearing of olfactory bulbs) or early signs of neurodegenerative diseases like Parkinson's. - II. Optic Nerve (Sensory)
Function: Transmits the special sense of vision from the retina of the eye to the visual cortex in the occipital lobe.
Clinical Test & Pathology: Test visual acuity utilizing a Snellen chart. Test visual fields by confrontation (testing peripheral vision). Examine the optic disc using an ophthalmoscope. Damage can result in partial or total blindness (anopsia). - III. Oculomotor Nerve (Motor & Parasympathetic)
Function: Controls the majority of extraocular eye muscles (superior, inferior, medial recti, and inferior oblique) to move the eye up, down, and medially. It raises the upper eyelid (levator palpebrae). It also provides parasympathetic control to constrict the pupil (sphincter pupillae).
Clinical Test & Pathology: Ask patient to track a finger making a wide "H-pattern" in the air. Shine a light in the eye to check for the pupillary light reflex. Damage presents as a "down and out" deviated eye, severe eyelid drooping (ptosis), and a blown, unreactive dilated pupil. - IV. Trochlear Nerve (Motor)
Function: Controls exactly one muscle: the superior oblique muscle, which utilizes a pulley-like tendon (trochlea) to move the eye downward and inward.
Clinical Test & Pathology: Ask the patient to look down and toward their nose. Damage causes the eye to drift upward, resulting in severe vertical double vision (diplopia), causing the patient to chronically tilt their head to compensate. - V. Trigeminal Nerve (Both - Sensory & Motor)
Function: The massive sensory nerve for the entire face (touch, pain, temperature) via three branches: Ophthalmic (V1), Maxillary (V2), and Mandibular (V3). It provides Motor innervation specifically to the muscles of mastication.
Clinical Test & Pathology: Test facial sensation across all three zones lightly with a cotton wisp and a sharp pin. Ask the patient to forcefully clench their jaw and palpate the masseter and temporalis muscles for equal strength. Trigeminal Neuralgia (Tic Douloureux) is a pathology involving excruciating, lightning-shock pain across the face. - VI. Abducens Nerve (Motor)
Function: Controls exactly one muscle: the lateral rectus muscle, which moves the eye laterally (it literally "abducts" the eye away from the midline).
Clinical Test & Pathology: Ask the patient to look far to the side (laterally). Damage paralyzes the lateral rectus, so the eye gets pulled inward (medially) by the unopposed medial rectus, resulting in a cross-eyed appearance and horizontal double vision. - VII. Facial Nerve (Both - Sensory, Motor, & Parasympathetic)
Function: Motor control for all muscles of facial expression. Sensory for the special sense of taste from the anterior two-thirds of the tongue. Parasympathetic control of tearing (lacrimal glands) and salivation (submandibular/sublingual glands).
Clinical Test & Pathology: Ask the patient to smile broadly, frown, puff out their cheeks, and raise their eyebrows tightly. Bell's Palsy is a severe acute unilateral paralysis of this nerve, resulting in a completely sagging face on one side, inability to close the eye, and drooling. - VIII. Vestibulocochlear Nerve (Sensory)
Function: Splits into two distinct parts: the cochlear nerve handles the special sense of hearing, and the vestibular nerve handles balance, equilibrium, and spatial orientation.
Clinical Test & Pathology: Test hearing using the whisper test, and tuning forks (Rinne and Weber tests) to differentiate conductive vs. sensorineural hearing loss. Test balance with the Romberg test. Pathologies here cause profound deafness, ringing in the ears (tinnitus), or severe, debilitating dizziness (vertigo). - IX. Glossopharyngeal Nerve (Both - Sensory, Motor, & Parasympathetic)
Function: Motor function for swallowing (stylopharyngeus muscle). Sensory for taste from the posterior one-third of the tongue, and general sensation from the pharynx, tonsils, and middle ear. It also monitors blood pressure via the carotid sinus. Parasympathetic control of the parotid salivary gland.
Clinical Test & Pathology: Lightly touch the back of the throat with a cotton swab to check the gag reflex. Ask the patient to say "ahhh" and watch for symmetrical uvula elevation. Damage causes loss of gag reflex and difficulty swallowing (dysphagia). - X. Vagus Nerve (Both - Sensory, Motor, & Parasympathetic)
Function: The name means "the wanderer." It is the massive parasympathetic superhighway of the body, providing motor innervation to the heart (slowing it down), lungs, and most of the abdominal viscera (stimulating digestion). It also provides motor control to the pharynx and larynx for swallowing and speaking.
Clinical Test & Pathology: Assessed simultaneously with CN IX (gag reflex, swallowing). Listen to the patient's voice; a damaged Vagus nerve will paralyze the vocal cords, leading to profound hoarseness and severe difficulty swallowing. - XI. Accessory Nerve (Motor)
Function: A unique nerve with both cranial and spinal roots. It strictly controls two massive neck/back muscles: the trapezius and the sternocleidomastoid (SCM).
Clinical Test & Pathology: Ask the patient to forcefully shrug their shoulders upward against the examiner's hands (testing Trapezius). Ask them to turn their head forcefully to the side against resistance (testing SCM). Damage causes a dropped, sagging shoulder and weakness turning the head. - XII. Hypoglossal Nerve (Motor)
Function: Controls almost all the intrinsic and extrinsic muscles of the tongue, allowing for complex maneuvers required for speech and manipulating food.
Clinical Test & Pathology: Ask the patient to stick their tongue straight out. If the nerve is damaged on one side, the healthy side pushes unopposed, causing the tongue to visibly deviate toward the paralyzed side. Long-term damage will also show atrophy (wasting away) and fasciculations (twitching) of the tongue muscle.
List of References
- Tortora, G. J., & Derrickson, B. H. (2017). Principles of Anatomy and Physiology (15th ed.). Wiley. (Core foundational anatomy and muscular attachments).
- Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2018). Clinically Oriented Anatomy (8th ed.). Lippincott Williams & Wilkins. (Clinical correlations, facial expression pathologies, and cranial nerve assessments).
- Netter, F. H. (2018). Atlas of Human Anatomy (7th ed.). Elsevier. (Visual spatial relationships of the deep neck, back, and pelvic floor musculature).
- Guyton, A. C., & Hall, J. E. (2020). Textbook of Medical Physiology (14th ed.). Elsevier. (Physiological mechanisms of mastication, deglutition, and respiration).
- Bickley, L. S., Szilagyi, P. G., & Hoffman, R. M. (2020). Bates' Guide to Physical Examination and History Taking (13th ed.). Wolters Kluwer. (Standardized clinical testing protocols for the 12 Cranial Nerves).