
Anatomy of the Lower Extremities: Muscles from the Pelvis to the Toe
By the end of this highly detailed anatomical master guide, you will be deeply conversant with:
- The Osteology (Bones) of the lower limb, including the intricate details of the bony pelvis, hip bone, and femur.
- The vital Ligaments of the Hip Joint that provide unmatched stability and posture control.
- The precise Origins, Insertions, Innervations, and Actions of every muscle group from the gluteal region down to the four layers of the foot.
- Clinical Correlations and Real-World Examples illustrating what happens when these bones, nerves, and muscles are injured.
Part 1: Osteology — The Bony Pelvis & The Hip Bone
The lower limb is engineered for two massive responsibilities: bearing the entire weight of the upper body and locomotion (movement). The hip joint is one of the most important joints in the body for complex movements like walking, running, or dancing. It relies on a strong bony foundation.
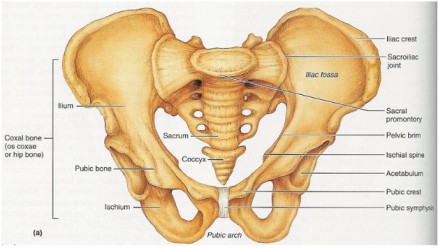
The Bony Pelvis
The bony pelvis is a massive, basin-shaped ring of bones connecting the flexible vertebral column to the femurs (thigh bones). It is formed by the sacrum, the coccyx (tailbone), and the two large hip bones (Os coxae).
Functional Example: The pelvis acts like a structural funnel. When you stand, the weight of your head, arms, and torso travels down your spine, hits the sacrum, splits in half across the pelvic ring, and is driven straight down into the heads of your two femurs.
The Hip Bone (Os Coxa)
Each large, irregularly shaped hip bone is actually a fusion of three primary bones. In children, these are separate bones joined by cartilage, but they completely fuse into a single solid bone by the end of puberty (around age 20-25).
The largest, most superior (top) part of the hip bone. It forms the prominent "wings" of the pelvis that you can feel when you put your hands on your hips.
- Iliac Crest: The palpable superior border. It serves as a major attachment site for abdominal muscles.
- Spines: It terminates anteriorly as the Anterior Superior Iliac Spine (ASIS) and posteriorly as the Posterior Superior Iliac Spine (PSIS). Below these are the AIIS and PIIS.
- Surfaces: The large, concave internal Iliac Fossa (houses the iliacus muscle); the rough outer Gluteal Surface (where the gluteal muscles attach); and the medial Auricular Surface (which articulates with the sacrum to form the sacroiliac joint).
- Notches: The Greater Sciatic Notch, a massive indentation allowing the thick sciatic nerve to exit the pelvis and enter the leg.
Forms the posteroinferior (lower-back) part of the hip bone. This is the heavy, durable bone you sit on.
- Ischial Tuberosity: The large, roughened "sitting bone." It supports your entire body weight when seated and is the origin point for the hamstring muscles.
- Ischial Spine: A pointed projection posterior to the acetabulum. It physically separates the Greater and Lesser Sciatic Notches.
- Ramus of the Ischium: A branch of bone that projects forward to join with the pubis.
Forms the anterior (front) part of the hip bone.
- Body of Pubis: The central, flat part that meets the other pubic bone at the midline cartilaginous joint called the Pubic Symphysis.
- Superior & Inferior Rami: Bars of bone that branch off the body to help form the acetabulum and the obturator foramen.
- Key Markings: Includes the Pubic Tubercle (where the inguinal ligament attaches) and the Obturator Crest for muscle attachments.
Key Landmarks of the Fused Hip Bone
- The Acetabulum: The deep, cup-shaped socket on the lateral surface of the hip bone, formed by the union of all three bones (Ilium, Ischium, Pubis). It articulates with the head of the femur.
- Lunate Surface: The crescent-shaped, smooth articular cartilage region.
- Acetabular Fossa: The rough, deep central depression.
- Acetabular Labrum: A raised ring of fibrocartilage that deepens the socket, gripping the femoral head like a suction cup for increased stability.
- Obturator Foramen: The massive opening created by the ischium and pubis. While it looks huge on a skeleton, in a living person it is almost completely closed by the tough obturator membrane, leaving only a tiny obturator canal for the obturator nerve and blood vessels to squeeze through into the thigh.
The Femur (Thigh Bone)
The femur is the longest, strongest, and heaviest bone in the human body. It is designed to transmit weight seamlessly from the hip bone down to the tibia.
- Proximal End: Features the highly spherical Head (which fits into the acetabulum). The head contains a tiny pit called the Fovea Capitis (attachment for the ligament of the head of the femur). Below the head is the constricted Neck. At the base of the neck are the massive Greater and Lesser Trochanters (leverage points for massive hip muscles). The Intertrochanteric Line (anterior) and Intertrochanteric Crest (posterior) connect the two trochanters.
- Shaft: A long, cylindrical body that bows slightly forward. It features a very prominent posterior ridge called the Linea Aspera, acting like a seam for the attachment of many powerful thigh muscles. Proximally, the linea aspera splits into the Pectineal Line and the Gluteal Tuberosity.
- Distal End: Flares out to form the knee joint with the massive Medial and Lateral Condyles. The deep posterior notch between them is the Intercondylar Fossa. The sides feature the Medial and Lateral Epicondyles (for knee ligament attachment), and the front features the smooth Patellar Surface (where the kneecap glides).
When an elderly patient with osteoporosis "breaks their hip," they usually have not broken the hip bone (os coxa). Instead, they have suffered a fracture across the Neck of the Femur. Because the blood vessels supplying the femoral head run exactly along this neck, a fracture here can sever the blood supply, leading to Avascular Necrosis (bone death) of the femoral head, often requiring a total hip replacement.
Part 2: Key Ligaments of the Hip Joint
Because the hip bears so much weight, its joint capsule is heavily reinforced by spiraling, thick ligaments. When you stand up straight, these ligaments twist tightly like wringing out a towel, pulling the femoral head deep into the socket and locking the joint in place. This allows you to stand for long periods using almost zero muscle energy!
- Iliofemoral Ligament (Y-ligament of Bigelow): The strongest ligament in the entire human body! Located anteriorly, it looks like an inverted 'Y'. Action: It prevents hyperextension of the hip when standing upright.
- Pubofemoral Ligament: Located anteroinferiorly (front and bottom). Action: It limits excessive abduction (spreading the legs too wide) and extension.
- Ischiofemoral Ligament: Located posteriorly (the back of the joint capsule). Action: It limits excessive internal rotation and adduction.
- Ligament of the Head of the Femur (Ligamentum Teres): Located entirely inside the joint cavity. It connects the fovea capitis of the femur to the acetabular fossa. It provides minimal physical stability but carries a tiny artery to feed the head of the femur in children.
- Transverse Acetabular Ligament: A strong band that bridges the gap (notch) at the bottom of the acetabulum, completing the full 360-degree socket ring.
Part 3: Muscles of the Lower Limb
The powerful muscles of the lower limb are uniquely designed for stability, locomotion, and maintaining an upright posture. We will cover them regionally, starting from the hip and working our way down to the toes.
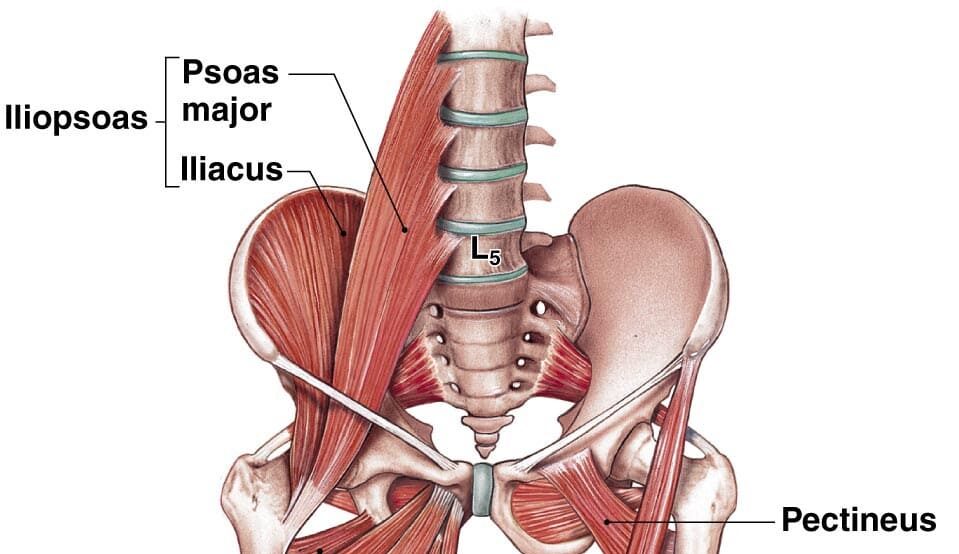
1. The Hip Muscles: The Iliopsoas Group
The Iliopsoas is not one muscle, but a composite of two muscles that merge. It is the strongest hip flexor in the body.
- Psoas Major: Originates high up from the lumbar vertebrae of the spine.
- Iliacus: Originates from the broad iliac fossa of the pelvis.
- Insertion: The two muscle bellies merge and insert together onto the lesser trochanter of the femur.
- Main Actions: Flexes the hip. This is the primary muscle you use when doing high-knee sprints, lifting your leg to climb a tall stair, or doing sit-ups (because it pulls the torso toward the thighs).
Because the Psoas Major originates from the lumbar spine and travels all the way down into the thigh, infections from the spine (like spinal tuberculosis) can drain into the sheath of this muscle. This creates a painful pocket of pus called a Psoas Abscess. A patient will present with severe groin pain and will refuse to extend their hip, keeping their leg pulled up in a flexed posture to reduce the stretch on the infected muscle.
2. Muscles of the Gluteal Region (Buttocks)
These muscles are absolutely essential for hip movement, pelvic stability, and keeping the trunk upright. They are divided into a superficial layer and a deep layer.
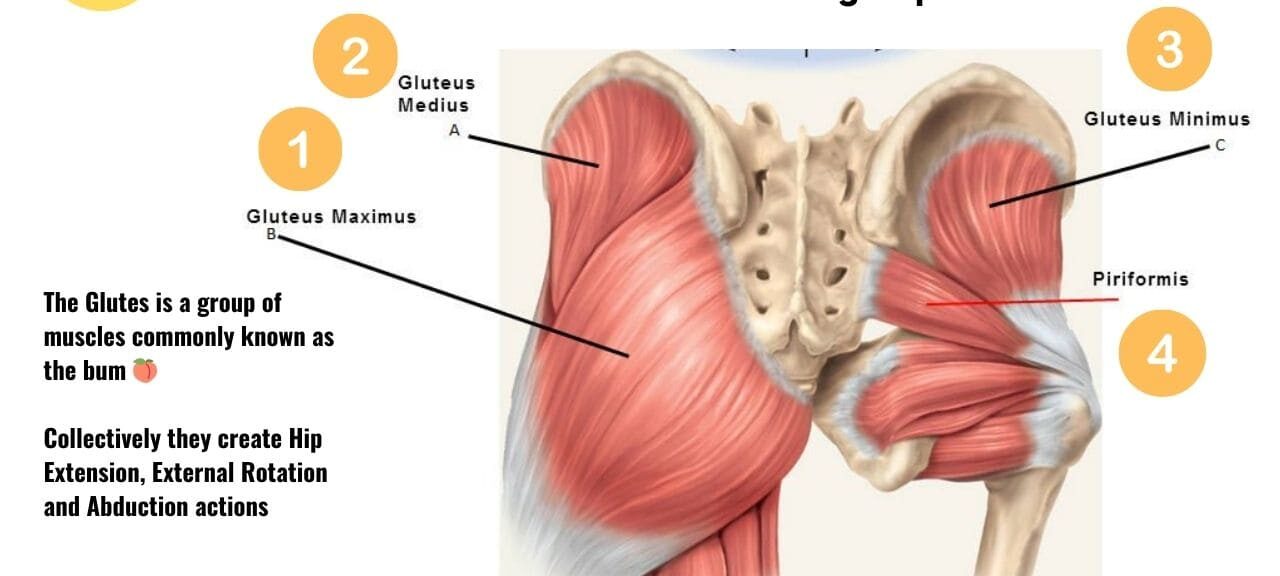
Superficial Gluteal Muscles
The largest, thickest, and most superficial gluteal muscle. It forms the primary mass of the buttocks.
- Action: It is the main extensor of the thigh. It generates massive power.
- Functional Example: You barely use this muscle when walking normally on flat ground. However, you use it heavily when climbing steep stairs, running, or performing a heavy barbell squat (standing up from a seated position). It is also a lateral rotator.
Lies deep to the Maximus. A thick, fan-shaped muscle.
- Action: The main abductor and medial rotator of the thigh.
- Functional Example: Its most vital job is stabilizing the pelvis during walking. When you lift your right foot off the ground to take a step, your left Gluteus Medius contracts aggressively to keep your pelvis level, preventing your right hip from dropping towards the floor.
The smallest and deepest of the three gluteal muscles.
- Action: It works as an exact synergist with the Gluteus Medius to abduct and medially rotate the thigh, helping to stabilize the pelvis during the gait cycle.
A small muscle situated anterolaterally (front and side) near the hip pocket.
- Action: Flexes, abducts, and medially rotates the thigh.
- Functional Example: Its main job is to pull tight (tense) the massive band of connective tissue on the side of your leg called the Iliotibial (IT) tract. By pulling this tight, it acts like a brace to lock and stabilize the knee in extension.
If the Superior Gluteal Nerve (which innervates the Gluteus Medius and Minimus) is injured—perhaps due to a poorly placed intramuscular injection in the buttocks—the patient loses the ability to stabilize their pelvis. When they stand on the affected leg, their pelvis will visibly drop on the unsupported, healthy side. To compensate while walking, they will lean their torso heavily over the injured side, producing a very distinctive waddling walk known as the Trendelenburg Gait.
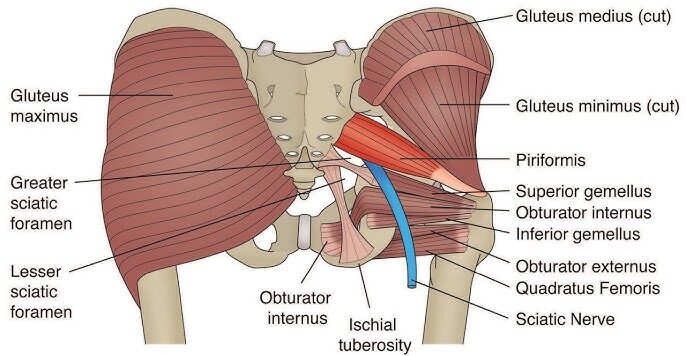
Deep Gluteal Muscles (Short External Rotators)
This group of six smaller muscles lies completely hidden deep to the bulky gluteus maximus. They act much like the "rotator cuff" of the shoulder. They collectively function as powerful lateral rotators of the thigh and physically hug the head of the femur, stabilizing it tightly inside the acetabulum.
- Piriformis: Pear-shaped muscle.
- Origin: Anterior surface of sacrum. Insertion: Superior border of greater trochanter. Innervation: Nerve to Piriformis (S1, S2).
- Actions: Laterally rotates, abducts (when hip is flexed), and extends the thigh.
- Superior Gemellus:
- Origin: Ischial spine. Insertion: Medial surface of greater trochanter. Innervation: Nerve to Obturator Internus.
- Actions: Laterally rotates and abducts the thigh.
- Obturator Internus:
- Origin: Pelvic surface of obturator membrane. Insertion: Medial surface of greater trochanter. Innervation: Nerve to Obturator Internus.
- Actions: Laterally rotates and abducts the thigh.
- Inferior Gemellus:
- Origin: Ischial tuberosity. Insertion: Medial surface of greater trochanter. Innervation: Nerve to Quadratus Femoris.
- Actions: Laterally rotates and abducts the thigh.
- Obturator Externus:
- Origin: External surface of obturator membrane. Insertion: Trochanteric fossa of femur. Innervation: Obturator Nerve.
- Actions: Laterally rotates and adducts the thigh.
- Quadratus Femoris: A flat, square-shaped muscle.
- Origin: Lateral border of ischial tuberosity. Insertion: Quadrate tubercle on intertrochanteric crest. Innervation: Nerve to Quadratus Femoris.
- Actions: A powerful lateral rotator and adductor of the thigh.
The massive Sciatic Nerve (the thickest nerve in the body) exits the pelvis and usually passes directly inferior to (underneath) the piriformis muscle. If a person overworks their glutes, the piriformis muscle can become tight, inflamed, or undergo spasms. This swollen muscle physically crushes the sciatic nerve against the pelvic bone. The patient will suffer from excruciating shooting pain, tingling, and numbness radiating from the buttock all the way down the back of the leg to the foot. This is called Sciatica caused by Piriformis Syndrome.
Summary Table of Gluteal Muscles
| Muscle | Origin | Insertion | Innervation | Main Actions |
|---|---|---|---|---|
| Gluteus Maximus | Ilium, sacrum, coccyx | IT tract, gluteal tuberosity | Inferior Gluteal N. | Extends & laterally rotates thigh |
| Gluteus Medius | External surface of ilium | Greater trochanter | Superior Gluteal N. | Abducts & medially rotates thigh; stabilizes pelvis |
| Gluteus Minimus | External surface of ilium | Greater trochanter | Superior Gluteal N. | Abducts & medially rotates thigh; stabilizes pelvis |
| Tensor Fasciae Latae | ASIS, iliac crest | IT tract | Superior Gluteal N. | Flexes, abducts, medially rotates thigh |
| Piriformis | Anterior sacrum | Greater trochanter | N. to Piriformis | Laterally rotates & abducts thigh |
| Obturator Internus | Obturator membrane | Greater trochanter | N. to Obturator Internus | Laterally rotates & abducts thigh |
| Gemelli (Sup & Inf) | Ischial spine/tuberosity | Greater trochanter | Varies | Laterally rotate & abduct thigh |
| Quadratus Femoris | Ischial tuberosity | Intertrochanteric crest | N. to Quadratus Femoris | Powerful lateral rotator of thigh |
Part 4: Muscles of the Thigh
The powerful muscles of the thigh are tightly packed and separated by thick walls of fascia (connective tissue) into three distinct compartments: Anterior, Medial, and Posterior. Each compartment has a primary nerve and a primary action.
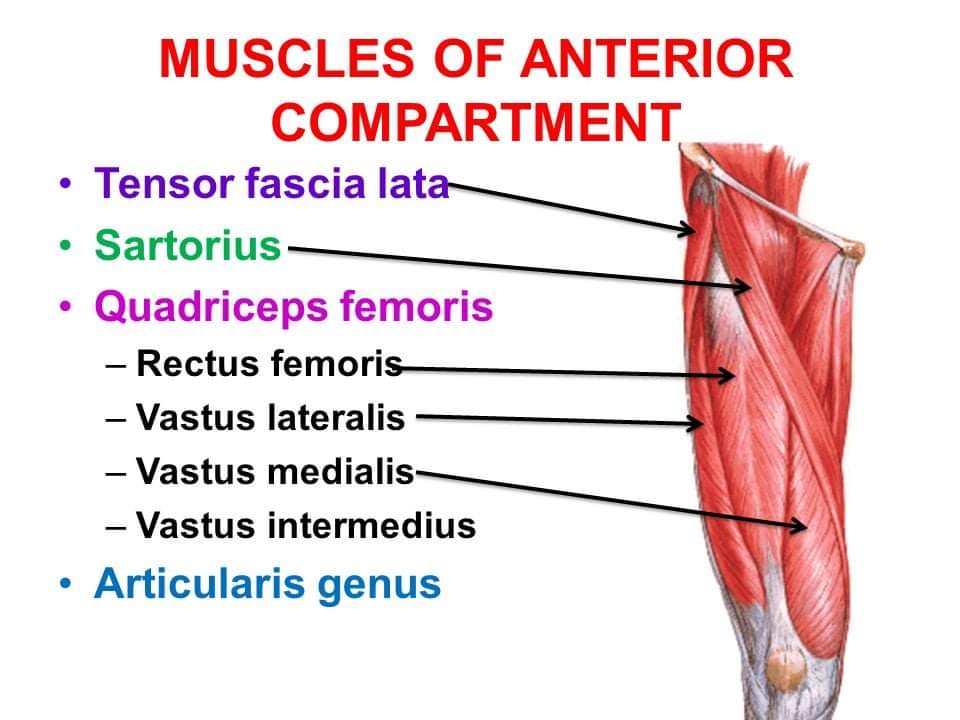
1. Anterior Compartment of the Thigh (The Extensors)
Innervation: Femoral Nerve (L2, L3, L4).
Main Actions: Primarily extension of the knee (kicking a ball); some flexion of the hip.
- Quadriceps Femoris: The massive muscle on the front of your thigh. It is actually a group of four distinct muscle bellies that converge into a single, incredibly strong patellar tendon (which encases the kneecap). It is the powerful extensor of the knee (essential for standing up, jumping, and kicking).
- Rectus Femoris: Runs straight down the middle. Unique because it originates on the pelvis (AIIS), meaning it crosses two joints. It extends the knee AND flexes the hip.
- Vastus Lateralis: The large muscle on the outside of the thigh.
- Vastus Medialis: The teardrop-shaped muscle on the inside of the knee. (Crucial for patellar tracking; keeps the kneecap from dislocating).
- Vastus Intermedius: Hidden completely beneath the Rectus Femoris.
- Sartorius: The longest muscle in the human body. It runs diagonally like a seatbelt from the outer hip (ASIS) to the inner knee. It flexes, abducts, and laterally rotates the thigh, and flexes the knee. Functional Example: It is known as the "tailor's muscle" because it performs the exact movement required to sit cross-legged on the floor.
2. Medial Compartment of the Thigh (The Adductors)
Innervation: Mostly Obturator Nerve (L2, L3, L4).
Main Actions: Primarily adduction of the thigh (squeezing the knees together).
This group includes five muscles. Functional Example: These are the muscles horseback riders use heavily to grip the horse, or soccer players use to pass the ball with the inside of their foot. Straining these muscles causes a "groin pull."
- Pectineus
- Adductor Longus
- Adductor Brevis
- Adductor Magnus: The largest and most powerful. It is a hybrid muscle. It has an "adductor part" (innervated by the obturator nerve) and a "hamstring part" (innervated by the sciatic nerve) that helps extend the hip.
- Gracilis: A very long, delicate, strap-like muscle running down the extreme medial thigh.
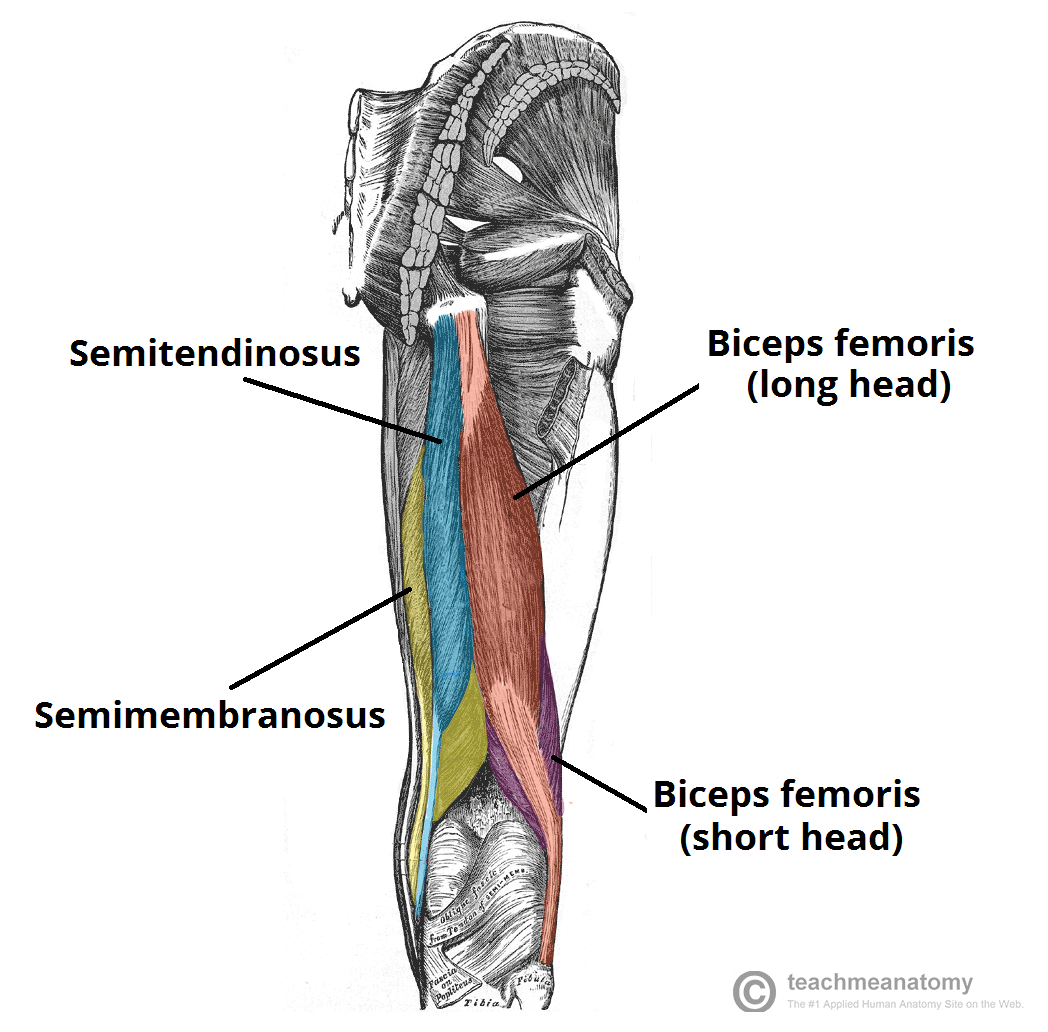
3. Posterior Compartment of the Thigh (The Hamstrings)
Innervation: Sciatic Nerve (Tibial portion), except for the short head of Biceps Femoris.
Main Actions: Primarily flexion of the knee (bending the knee backward) and extension of the hip.
- Biceps Femoris: The lateral (outer) hamstring muscle. As the name suggests, it has two heads (a long head from the ischial tuberosity and a short head from the linea aspera). It flexes the knee and laterally rotates the leg.
- Semitendinosus: A medial hamstring muscle. About half its length is a long, cord-like tendon. It flexes the knee and medially rotates the leg.
- Semimembranosus: A medial hamstring muscle lying directly deep to the Semitendinosus. It features a wide, flat, membranous tendon at its origin. It flexes the knee and medially rotates the leg.
Hamstring injuries are incredibly common in sprinters, hurdlers, and soccer players. These muscles cross two joints (hip and knee). During an explosive sprint, the hamstrings must eccentrically contract (brake) to stop the leg from violently snapping forward at the end of the swing phase. This massive, sudden tension often causes the muscle fibers to tear, usually near their origin at the Ischial Tuberosity, resulting in severe pain, bruising, and inability to extend the leg.
Summary Table of Thigh Muscles
| Muscle | Origin | Insertion | Innervation | Main Actions |
|---|---|---|---|---|
| ANTERIOR COMPARTMENT | ||||
| Rectus Femoris | AIIS | Patella & Tibial Tuberosity | Femoral N. | Extends knee, flexes hip |
| Vastus Lateralis | Greater trochanter, linea aspera | Patella & Tibial Tuberosity | Femoral N. | Extends knee |
| Vastus Medialis | Intertrochanteric line, linea aspera | Patella & Tibial Tuberosity | Femoral N. | Extends knee |
| Vastus Intermedius | Femoral shaft | Patella & Tibial Tuberosity | Femoral N. | Extends knee |
| Sartorius | ASIS | Medial tibia (Pes Anserinus) | Femoral N. | Flexes, abducts, lat. rotates thigh; flexes knee |
| MEDIAL COMPARTMENT | ||||
| Adductor Longus/Brevis/Magnus | Pubis, Ischial ramus | Femur (linea aspera) | Obturator N. (Magnus also Sciatic N.) | Adduct thigh; Magnus also extends thigh |
| Gracilis | Pubic symphysis | Medial tibia (Pes Anserinus) | Obturator N. | Adducts thigh, flexes knee |
| POSTERIOR COMPARTMENT (HAMSTRINGS) | ||||
| Biceps Femoris | Long: Ischial tuberosity; Short: Linea aspera | Head of fibula | Sciatic N. (Tibial & Common Fibular) | Flexes knee, extends hip, lat. rotates leg |
| Semitendinosus | Ischial tuberosity | Medial tibia (Pes Anserinus) | Sciatic N. (Tibial) | Flexes knee, extends hip, med. rotates leg |
| Semimembranosus | Ischial tuberosity | Medial condyle of tibia | Sciatic N. (Tibial) | Flexes knee, extends hip, med. rotates leg |
Part 5: Muscles of the Leg
The portion of the lower limb between the knee and the ankle is anatomically called the "leg" (crus). The muscles here are divided into four tightly packed compartments bounded by the tough interosseous membrane and unyielding fascial septa.
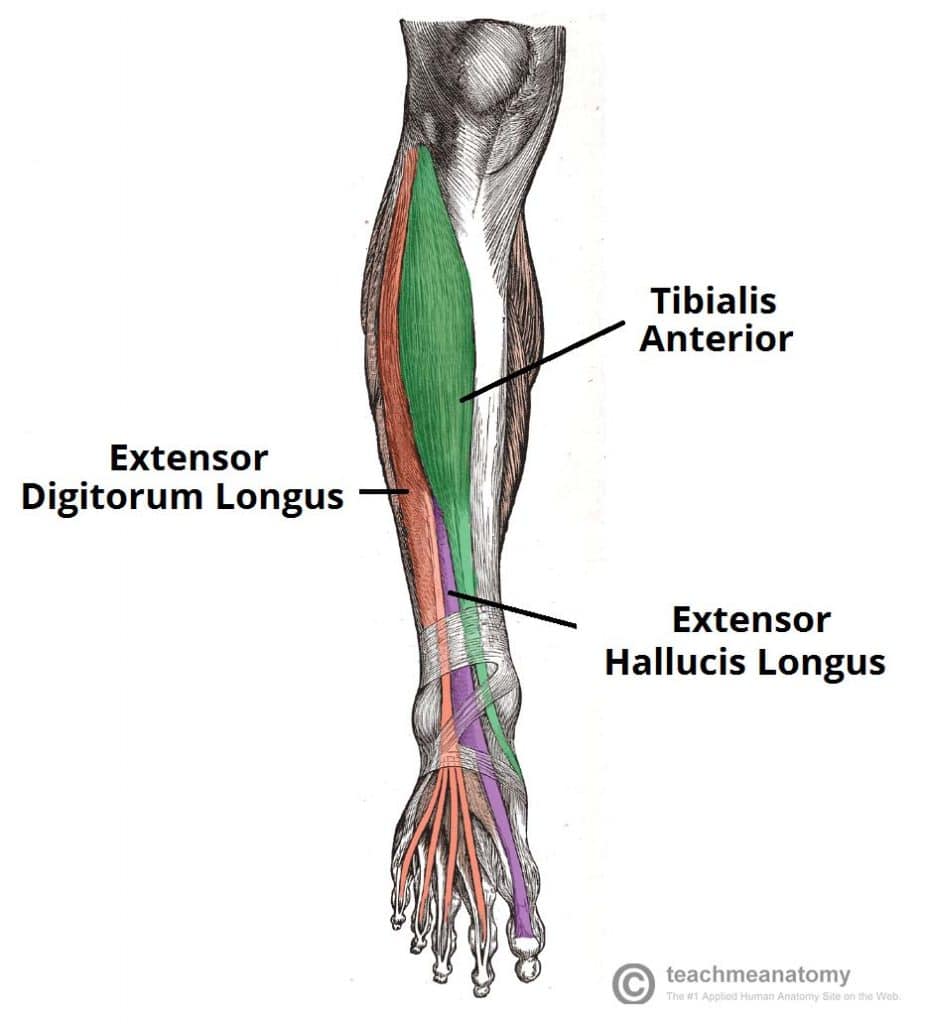
1. Anterior Compartment of the Leg
Innervation: Deep Fibular (Peroneal) Nerve (L4, L5, S1).
Main Actions: Primarily dorsiflexion of the ankle (pulling the toes up toward the shin) and extension of the toes.
- Tibialis Anterior: The thick muscle next to the shin bone. The main dorsiflexor and invertor of the foot. It prevents your toes from dragging on the ground when you swing your leg forward to walk.
- Extensor Digitorum Longus: Extends the lateral four toes.
- Extensor Hallucis Longus: Extends the great toe (hallux).
- Fibularis (Peroneus) Tertius: A small muscle that dorsiflexes and everts the foot.
If a patient fractures the head of their fibula, the Deep Fibular Nerve wrapping around the bone can be crushed. This paralyzes the entire anterior compartment. The patient completely loses the ability to dorsiflex the ankle. As they walk, their foot flops down limply (Foot Drop), and their toes drag on the ground. To compensate, they must lift their knee abnormally high on every step, producing a "Steppage Gait."
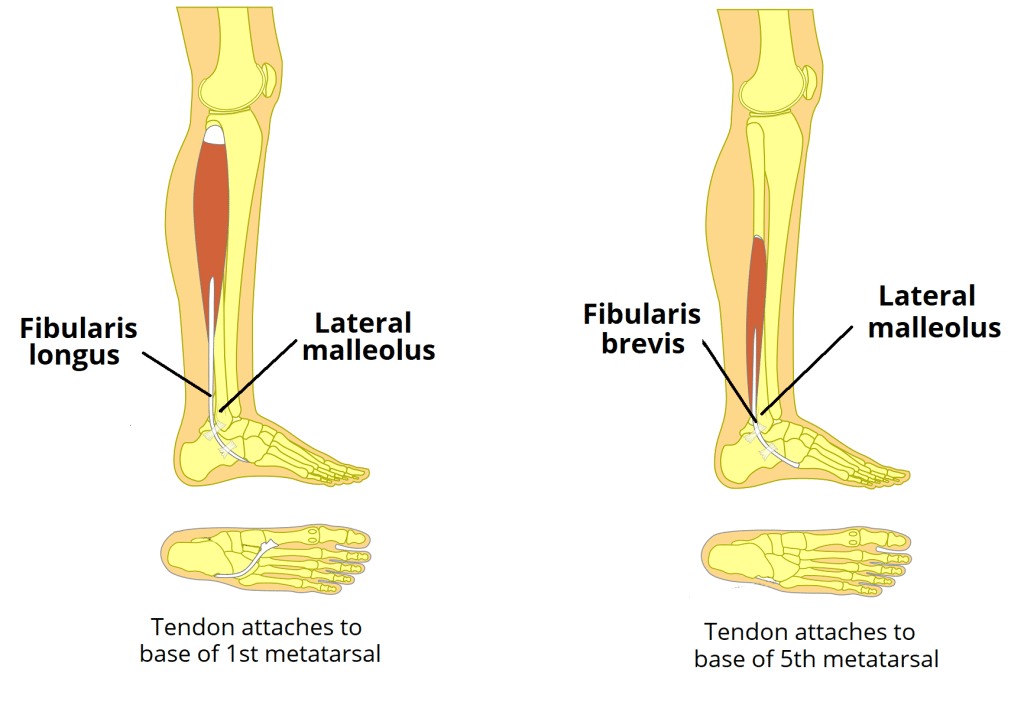
2. Lateral Compartment of the Leg
Innervation: Superficial Fibular (Peroneal) Nerve (L5, S1, S2).
Main Actions: Primarily eversion of the foot (turning the sole outward) and weak plantarflexion.
This compartment contains two muscles: Fibularis (Peroneus) Longus and Fibularis (Peroneus) Brevis. Functional Example: When you accidentally step on a rock and your ankle starts to roll inward (inversion sprain), these muscles fire aggressively, everting the foot to try and save your ankle ligaments from tearing.
3. Posterior Compartment of the Leg
Innervation: Tibial Nerve (L4-S2).
Main Actions: Primarily plantarflexion of the ankle (pointing toes down, standing on tiptoes), inversion of the foot, and flexion of the toes.
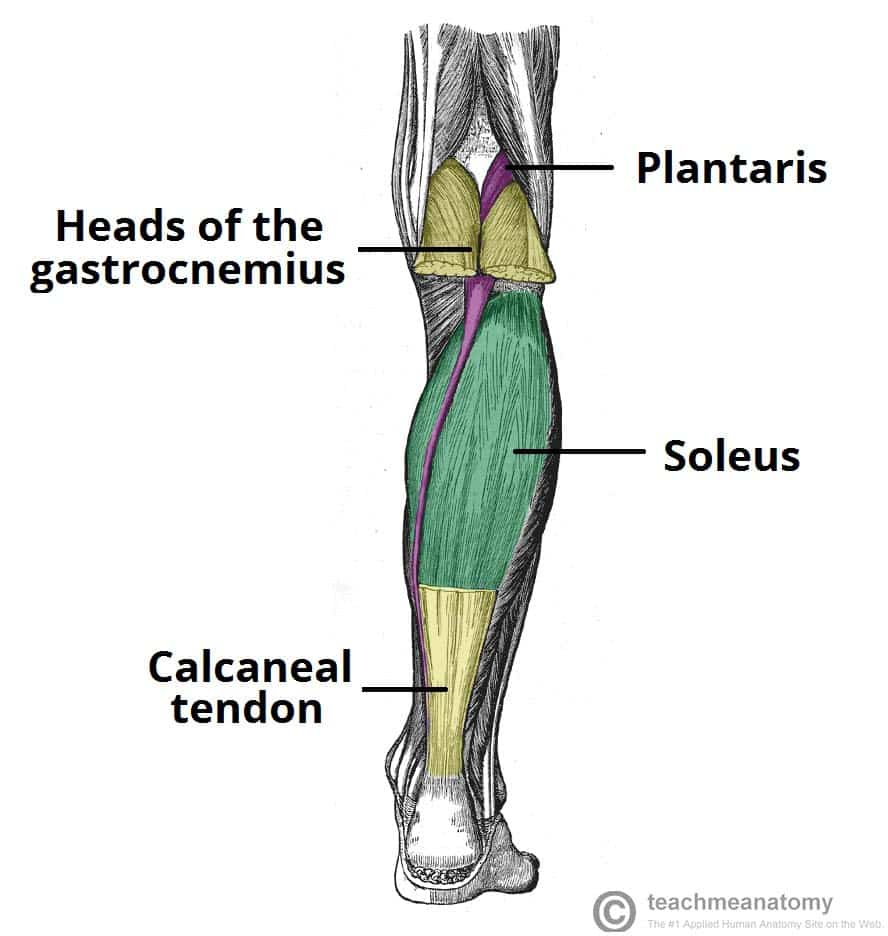
Superficial Group (The Calf Muscles)
This group forms the massive bulk of the calf. They all merge to insert onto the heel bone via the massive Calcaneal (Achilles) tendon.
- Gastrocnemius: The prominent, two-headed muscle that gives the calf its shape. Because it crosses the knee joint, it can both flex the knee and plantarflex the ankle. Highly active during explosive jumping and sprinting.
- Soleus: A massive, flat, powerful muscle lying deep to the gastrocnemius. It is a pure plantarflexor. Functional Example: It is packed with slow-twitch endurance fibers because it fires continuously all day long to keep you from falling forward when standing still.
- Plantaris: A tiny muscle belly with an incredibly long, thin tendon. Often mistaken for a nerve by medical students.
(Together, the Gastrocnemius and Soleus are known as the Triceps Surae).
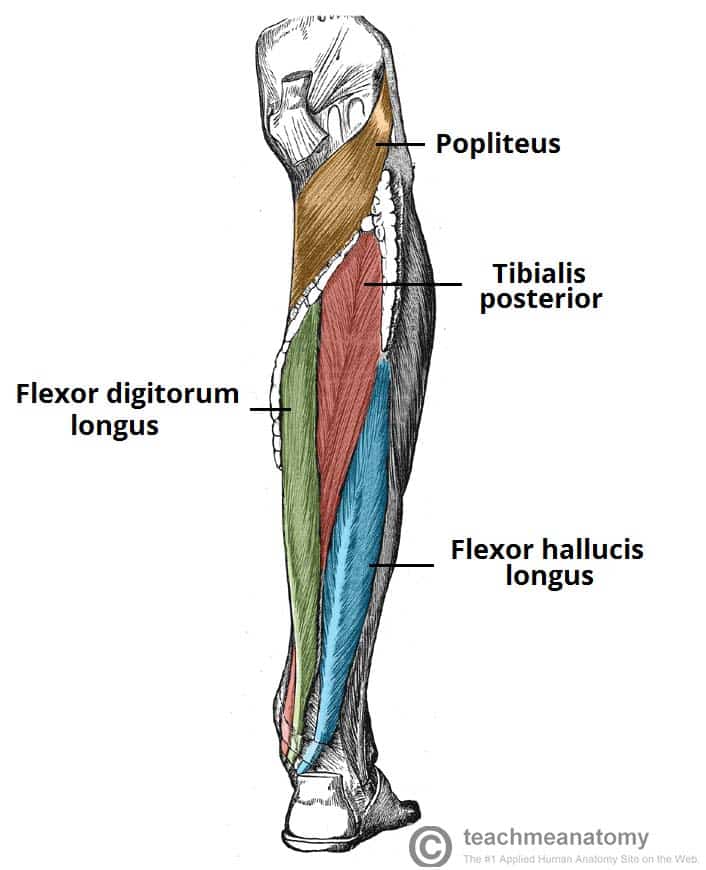
Deep Group
These muscles lie buried beneath the soleus, plastered against the back of the tibia and fibula.
- Popliteus: A small diagonal muscle behind the knee. Its crucial job is to "unlock" the fully extended knee by laterally rotating the femur slightly, allowing flexion to begin.
- Flexor Digitorum Longus: Flexes the lateral four toes.
- Flexor Hallucis Longus: Flexes the great toe (provides the powerful "push-off" force at the end of a walking stride).
- Tibialis Posterior: The deepest muscle. It is the main invertor of the foot and provides massive dynamic support to the medial arch of the foot.
The tendons, artery, and nerve of the deep posterior compartment pass snugly behind the medial malleolus (inner ankle bone) on their way to the foot. You can remember their order from anterior to posterior using the classic phrase:
"Tom, Dick, And Very Nervous Harry"
Tibialis posterior, flexor Digitorum longus, posterior tibial Artery, Vein, tibial Nerve, flexor Hallucis longus.
Summary Table of Leg Muscles
| Muscle | Origin | Insertion | Innervation | Main Actions |
|---|---|---|---|---|
| ANTERIOR COMPARTMENT | ||||
| Tibialis Anterior | Lateral tibia | Medial cuneiform, 1st metatarsal | Deep Fibular N. | Main dorsiflexor; inverts foot |
| Extensor Digitorum Longus | Tibia, fibula | Distal phalanges of digits 2-5 | Deep Fibular N. | Extends lateral four toes |
| Extensor Hallucis Longus | Fibula | Distal phalanx of great toe | Deep Fibular N. | Extends great toe |
| LATERAL COMPARTMENT | ||||
| Fibularis (Peroneus) Longus | Head of fibula | 1st metatarsal, medial cuneiform | Superficial Fibular N. | Everts foot; plantarflexes ankle |
| Fibularis (Peroneus) Brevis | Lateral fibula | Base of 5th metatarsal | Superficial Fibular N. | Everts foot; plantarflexes ankle |
| POSTERIOR COMPARTMENT (SUPERFICIAL) | ||||
| Gastrocnemius | Femoral condyles | Calcaneus via Achilles tendon | Tibial N. | Plantarflexes ankle, flexes knee |
| Soleus | Tibia, fibula | Calcaneus via Achilles tendon | Tibial N. | Powerful plantarflexor |
| POSTERIOR COMPARTMENT (DEEP) | ||||
| Tibialis Posterior | Tibia, fibula | Navicular, cuneiforms, etc. | Tibial N. | Main invertor of foot |
| Flexor Digitorum Longus | Posterior tibia | Distal phalanges of digits 2-5 | Tibial N. | Flexes lateral four toes |
| Flexor Hallucis Longus | Posterior fibula | Distal phalanx of great toe | Tibial N. | Flexes great toe |
Part 6: Muscles of the Foot
The intrinsic muscles of the foot (meaning both origin and insertion are within the foot) are divided into dorsal (top) and plantar (sole) groups. They are responsible for fine motor control, spreading the toes, and providing dynamic, spring-like support to the arches of the foot when walking barefoot on uneven surfaces like sand.
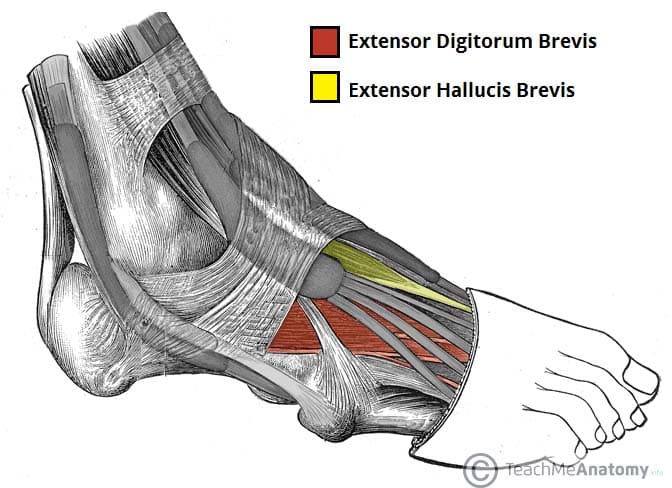
1. Dorsal Muscles of the Foot
- Extensor Digitorum Brevis: Originates from the calcaneus (heel bone) and helps extend toes 2-4.
- Extensor Hallucis Brevis: Originates from the calcaneus and helps extend the great toe.
2. Plantar Muscles of the Foot (The Sole)
These muscles are incredibly complex and are organized into four distinct layers from superficial (closest to the skin) to deep (closest to the bones). They are covered by the thick, leathery Plantar Aponeurosis (fascia). They are primarily innervated by the Medial and Lateral Plantar Nerves (branches of the Tibial Nerve).
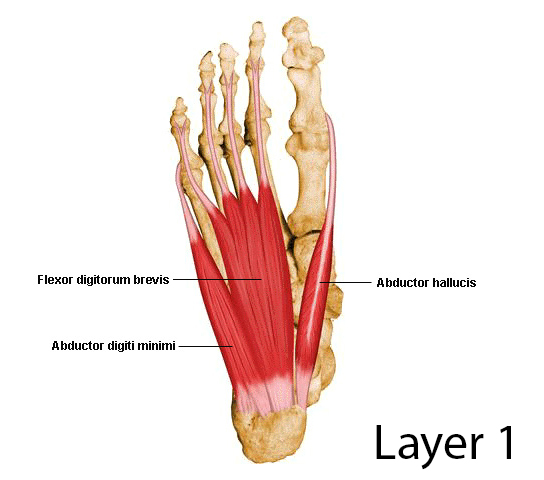 Layer 1 (Superficial)
Layer 1 (Superficial)
The first layer you see after stripping away the thick plantar fascia.
- Abductor Hallucis: Abducts and flexes the great toe. (Innervated by Medial Plantar N.)
- Flexor Digitorum Brevis: Flexes the lateral four toes at the PIP joints. (Innervated by Medial Plantar N.)
- Abductor Digiti Minimi: Abducts and flexes the little toe. (Innervated by Lateral Plantar N.)
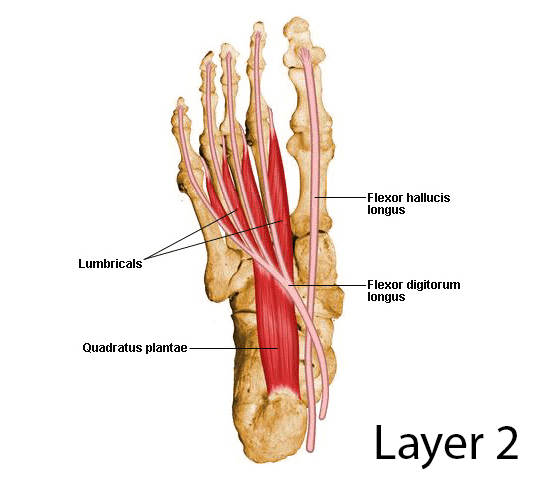 Layer 2
Layer 2
Contains two muscle groups directly associated with the long tendons coming from the leg.
- Quadratus Plantae: A square muscle that grabs onto the tendon of the Flexor Digitorum Longus (FDL). Because the FDL tendon comes in at a diagonal angle from the ankle, the Quadratus Plantae pulls on it to straighten its line of pull, ensuring the toes flex straight down. (Innervated by Lateral Plantar N.)
- Lumbricals (4): Worm-like muscles originating off the FDL tendons. They flex the MTP joints and extend the IP joints of the lateral four toes. (Innervated by Medial and Lateral Plantar Nerves).
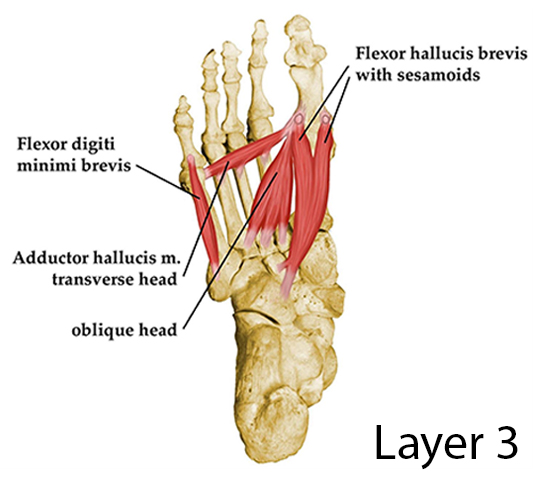 Layer 3
Layer 3
Focuses primarily on the great and little toes.
- Flexor Hallucis Brevis: Flexes the great toe at the MTP joint. Its split tendon houses the two tiny sesamoid bones of the foot. (Innervated by Medial Plantar N.)
- Adductor Hallucis: Has a large oblique head and a transverse head. It firmly adducts the great toe, helping maintain the transverse arch of the foot. (Innervated by Lateral Plantar N.)
- Flexor Digiti Minimi Brevis: Flexes the little toe. (Innervated by Lateral Plantar N.)
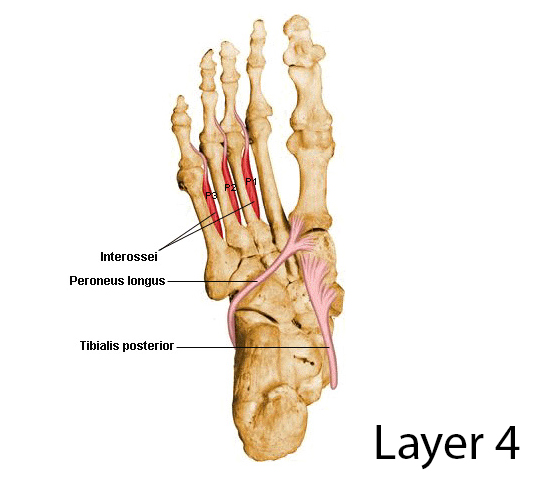 Layer 4 (Deepest)
Layer 4 (Deepest)
Buried deeply between the metatarsal bones.
- Plantar Interossei (3): Adduct toes 3-5.
Mnemonic: PAD (Plantar Adduct). (Innervated by Lateral Plantar N.) - Dorsal Interossei (4): Abduct toes 2-4.
Mnemonic: DAB (Dorsal Abduct). (Innervated by Lateral Plantar N.)
Although their fleshy muscle bellies are located way up in the leg, the massive tendons of the Tibialis Anterior and Fibularis Longus cross the ankle joint and insert deep into the bones of the foot. The Fibularis Longus tendon wraps completely under the sole of the foot to meet the Tibialis Anterior, creating a structural "stirrup" or "sling." Together, they provide immense dynamic support holding up the arches of your foot and preventing flat feet (pes planus).
Summary Table of Foot Muscles
| Layer/Group | Muscle | Origin | Insertion | Innervation | Main Actions |
|---|---|---|---|---|---|
| DORSAL MUSCLES | |||||
| Dorsal | Extensor Digitorum Brevis | Calcaneus | Extensor expansions 2-4 | Deep Fibular N. | Extends toes 2-4 |
| Dorsal | Extensor Hallucis Brevis | Calcaneus | Prox. phalanx of great toe | Deep Fibular N. | Extends great toe |
| PLANTAR MUSCLES | |||||
| Layer 1 | Abductor Hallucis | Calcaneus | Prox. phalanx of great toe | Medial Plantar N. | Abducts & flexes great toe |
| Layer 1 | Flexor Digitorum Brevis | Calcaneus | Middle phalanges 2-5 | Medial Plantar N. | Flexes toes 2-5 (PIP) |
| Layer 1 | Abductor Digiti Minimi | Calcaneus | Prox. phalanx of 5th toe | Lateral Plantar N. | Abducts & flexes 5th toe |
| Layer 2 | Quadratus Plantae | Calcaneus | Tendon of FDL | Lateral Plantar N. | Assists FDL in flexing |
| Layer 2 | Lumbricals (4) | Tendons of FDL | Extensor expansions 2-5 | Medial & Lateral Plantar N. | Flex MTPs, Extend IPs |
| Layer 3 | Flexor Hallucis Brevis | Cuboid, cuneiforms | Prox. phalanx of great toe | Medial Plantar N. | Flexes great toe |
| Layer 3 | Adductor Hallucis | Metatarsals 2-4 | Prox. phalanx of great toe | Lateral Plantar N. | Adducts great toe |
| Layer 3 | Flexor Digiti Minimi Brevis | Base of 5th metatarsal | Prox. phalanx of 5th toe | Lateral Plantar N. | Flexes little toe |
| Layer 4 | Plantar Interossei (3) | Metatarsals 3-5 | Prox. phalanges 3-5 | Lateral Plantar N. | Adduct toes (PAD) |
| Layer 4 | Dorsal Interossei (4) | Adjacent metatarsals | Prox. phalanges 2-4 | Lateral Plantar N. | Abduct toes (DAB) |
List of References
The anatomical details, functional biomechanics, and clinical correlations in this guide are synthesized based on universally accepted medical anatomy curricula and reference standards, including:
- Moore, K. L., Dalley, A. F., & Agur, A. M. R. Clinically Oriented Anatomy. 8th Edition. Lippincott Williams & Wilkins. (Core standard for clinical and regional anatomy).
- Standring, S. Gray's Anatomy: The Anatomical Basis of Clinical Practice. 42nd Edition. Elsevier. (Definitive reference for gross anatomical structures).
- Netter, F. H. Atlas of Human Anatomy. 7th Edition. Elsevier. (For visual correlations of muscle layers, bony landmarks, and fascial compartments).
- Snell, R. S. Clinical Anatomy by Regions. 9th Edition. Lippincott Williams & Wilkins.
- Drake, R., Vogl, A. W., & Mitchell, A. W. M. Gray's Anatomy for Students. 4th Edition. Elsevier.