
🏥 Nurses Revision Uganda
📱 WhatsApp: 0726113908 | 🌐 Website:https://nursesrevisionuganda.com
UNMEB PALLIATIVE CARE DND 2023
SECTION A: Objective Questions (20 marks)
💡 Palliative Care Focus: Remember the WHO definition - improving quality of life for patients with life-threatening illness. It's about living fully until death, not just dying.
1
The most commonly occurring gastro-intestinal malignancy among patients receiving palliative care is ............................................. cancer.
(c) Colonal (Colorectal)
Colorectal cancer is the most common gastrointestinal malignancy globally and frequently presents at advanced stages requiring palliative care. High incidence rates, especially in developed countries, combined with late diagnosis due to asymptomatic early disease, make it the leading GI cancer in palliative settings. It causes bowel obstruction, bleeding, pain, and cachexia that significantly impair quality of life.
GI CANCER PREVALENCE: "C-CORD" - Colorectal, Colon, Oesophageal, Rectal, Duodenal
2
A high percentage of palliative care patients admitted in hospitals have complaints of pain which sometimes is NOT well attended to because of
(d) Inadequate knowledge and skills
Pain undertreatment in palliative care stems primarily from knowledge deficits - lack of understanding of pain assessment, opioid pharmacology, addiction myths, and fear of side effects. Many healthcare providers have inadequate training in palliative pain management, leading to "opiophobia" and poor pain control. This is the most systemic and correctable barrier compared to individual staff issues or workload.
📚 Knowledge Gap: Studies show 70% of medical students receive <5 hours of palliative care education. This creates generations of clinicians unprepared for pain management!
3
Which of the following is NOT a quality of a good listener?
(c) Being emotional
Being emotional (losing composure, crying with patient, becoming overly involved) compromises therapeutic boundaries and impairs objective assessment. While empathy is crucial, emotional over-involvement prevents active listening, clouds judgment, and may burden the patient with the nurse's feelings. Professional detachment with compassion is the ideal stance.
ACTIVE LISTENING: "PEAR" - Paraphrase, Eye contact, Ask open questions, Reflect feelings
4
The most common symptom associated with cancer is
(c) Pain
Pain is the most prevalent and feared symptom in cancer, affecting 70-90% of advanced cancer patients. It results from tumor infiltration of nerves/compression of structures, treatment side effects, or inflammatory processes. Pain is multidimensional (physical, emotional, spiritual) and the primary driver for seeking palliative care. Effective pain control is the cornerstone of cancer palliation.
🔥 Pain is the 5th Vital Sign! Always assess pain intensity, character, location, and response to treatment. Uncontrolled pain is a medical emergency.
5
Poor wound healing in palliative care patients occurs mainly due to
(c) Debility and poor nutrition
Cancer cachexia and protein-calorie malnutrition are the primary causes of impaired wound healing in palliative patients. Cachexia involves muscle wasting, hypoalbuminemia, and metabolic derangements that deprive tissues of essential building blocks. Poor nutrition reduces collagen synthesis, angiogenesis, and immune function. Combined with anemia, hypoxia, and metabolic demands of cancer, wounds fail to progress through normal healing phases.
WOUND HEALING FACTORS: "NUTRIENTS" - Nutrition, Underlying disease, Tissue perfusion, Radiation, Infection, Edges, Moisture, Stress
6
Noisy breathing and excess secretions experienced at the end of life (death rattle) should best be managed with
(b) Buscopan
Buscopan (hyoscine butylbromide) is the drug of choice for terminal secretions/death rattle. It's an antimuscarinic that reduces respiratory secretions by blocking parasympathetic stimulation. Given subcutaneously (20-40 mg stat, then 20-80 mg/24h via syringe driver). Unlike atropine, it doesn't cross BBB significantly, causing fewer CNS side effects. It effectively dries secretions within 30-60 minutes.
🫁 Death Rattle is NOT suffering! The patient is usually unconscious and not distressed. The medication is for family/observer comfort. Positioning (semi-prone) helps too.
7
Which of the following is NOT a challenge of offering palliative care in Uganda?
(c) Reaching everyone is possible
"Reaching everyone is possible" is false and NOT a challenge - it's an aspiration. In Uganda, reaching all palliative care patients is impossible due to severe resource constraints, geographic barriers, poverty, and lack of services. Only ~10% of those needing palliative care actually receive it. The statement describes an ideal, not a challenge. All other options are documented major challenges in Ugandan palliative care delivery.
UGANDA PALLIATIVE CHALLENGES: "LATE" - Late presentation, Accessibility issues, Too many patients, Education gaps
8
Which of the following manifestations should the nurse anticipate in patients with spiritual distress?
(c) Loneliness
Spiritual distress manifests as profound isolation and loneliness - feeling disconnected from self, others, meaning, and transcendence. Patients question life's purpose, feel abandoned by God/higher power, and experience existential loneliness even in company. This differs from psychological denial or bargaining (part of grief stages). Spiritual distress requires chaplaincy referral, life review, reconciliation, and presence.
🙏 Spiritual Assessment Tool: FICA - F=Faith beliefs, I=Importance, C=Community, A=Address in care. Loneliness is the red flag!
9
Which of the following nursing interventions is NOT appropriate in end of life care?
(b) Encourage family to maximize social isolation
Social isolation is harmful and inappropriate in end-of-life care. Social connection and support are fundamental human needs at life's end. Isolation increases suffering, depression, and spiritual distress. The goal is to facilitate visits, connections, and legacy activities. Social isolation directly contradicts palliative care principles of holistic support and relationship-centered care.
👥 Never Isolate! The dying need connection. Facilitate "gatherings," memory-making, reconciliation, and community support. Isolation = suffering.
10
Which of the following is NOT a suggestive symptom of superior vena cava compression?
(a) Pallor of the lower limbs
SVCS affects the upper body only (above the heart). Lower limb pallor suggests anemia, arterial insufficiency, or other pathology, not SVC obstruction. SVCS causes superior vena cava obstruction leading to venous congestion in head, neck, arms, and upper torso. Symptoms are all above the diaphragm.
SVCS SYMPTOMS: "FACE" - Facial swelling, Arm swelling, Cyanosis, Engorged veins (neck/chest)
11
Which of the following is a sign of opioid toxicity?
(d) Respiratory distress and insomnia
The most critical and life-threatening sign of opioid toxicity is **respiratory depression**, which is encapsulated by "Respiratory distress" in this option. Opioids depress the central nervous system, leading to slowed and shallow breathing, which can progress to respiratory arrest. While "insomnia" is typically associated with opioid withdrawal rather than acute toxicity (which usually causes drowsiness/sedation), the presence of "Respiratory distress" makes this option the most accurate indicator of a severe and dangerous level of opioid toxicity among the choices provided. In a multiple-choice question where the best option must be chosen, the life-threatening nature of respiratory compromise takes precedence.
Key signs of opioid toxicity include:
Key signs of opioid toxicity include:
- **Respiratory depression:** Slowed, shallow, or absent breathing.
- **Miosis (pinpoint pupils):** Very constricted pupils.
- **Sedation/Decreased level of consciousness:** Ranging from drowsiness to unresponsiveness.
- Hypotension (low blood pressure) and bradycardia (slow heart rate) can also occur.
OPIOID TOXICITY (Severe Overdose): Think "CPR-S" for Critical signs:
- Coma (or severe sedation)
- Pinpoint Pupils
- Respiratory Depression
- Slowed Heart Rate (Bradycardia) / Shallow Breathing
12
A non-pharmacological measure that significantly controls pain in children is to
(b) Keep the child with the mother all time
Maternal presence is the most powerful non-pharmacological analgesic for children. Skin-to-skin contact, breastfeeding, and maternal voice activate oxytocin release, reduce cortisol, and provide security and comfort that modulates pain perception. This is evidence-based for procedures and chronic pain. The mother's presence provides distraction, emotional support, and helps child cope with painful stimuli.
👩👧 Mother as Medicine! Kangaroo care reduces pain scores by 30% in neonates. Encourage family-centered care - parents are partners in pain management.
13
Which of the following is the most common side effect of morphine?
(d) Constipation
Constipation is the most common and persistent side effect of opioids, affecting >95% of patients. Opioids bind to mu receptors in the gut, reducing peristalsis and increasing sphincter tone. It is dose-dependent and tolerance does NOT develop. Must be prevented proactively with laxatives (stimulant + stool softener) started at same time as opioid, not waiting for constipation to occur.
OPIOID SIDE EFFECTS: "C-SNAP" - Constipation, Sedation, Nausea, Addiction (rare), Pruritus. Always remember: Constipation never sleeps!
14
Which of the following is NOT a primary goal for hospice care? To
(b) hasten death as quickly as possible
Hospice care NEVER aims to hasten death. This is a fundamental ethical principle distinguishing palliative care from euthanasia. Hospice focuses on comfort, dignity, and quality of life until natural death occurs. Hastening death violates the principle of non-maleficence and is illegal. The goal is to neither hasten nor postpone death, but to support living fully until death.
⚖️ Ethical Distinction: Hospice = comfort until natural death. Euthanasia = intentionally ending life. Physician-assisted suicide = providing means. Know the difference - it's crucial!
15
Which of the following is a clinician related factor that contributes to the low rate of end of life discussion?
(a) Lack of time
Clinicians consistently report insufficient time as a major barrier to end-of-life conversations. These discussions require 30-60 minutes of uninterrupted time to assess understanding, explore values, discuss options, and answer questions. In busy clinical settings with high patient loads, finding this time is challenging. This is a systems issue requiring protected time and scheduling.
16
Which of the following is NOT true about breaking bad news to patients?
(c) Do not follow the patient's decision while breaking the news
NOT following patient's decision violates autonomy and the SPIKES protocol. Patients have the right to determine how much information they want and who should receive it. Some may not want full disclosure. The nurse must respect these preferences while ensuring someone (family member) can act as information receiver. Imposing information against will causes psychological harm.
SPIKES PROTOCOL: S=Setting, P=Perception, I=Invitation, K=Knowledge, E=Emotions, S=Strategy
17
Addiction and psychological dependence does NOT occur when opioids are given
(a) orally
Route of administration does NOT determine addiction risk - this question appears flawed. However, oral route has the lowest addiction potential because slower absorption produces less euphoria. Addiction in palliative care is <1% regardless of route. The key is indication - therapeutic use for pain doesn't cause addiction; recreational use seeking euphoria does. All parenteral routes (IV, SC, IM) have higher abuse potential.
📉 Addiction Myth: Studies show <1% of cancer patients become addicted when opioids used for pain. Physical dependence is normal, addiction is rare. Don't undertreat pain due to fear!
18
Which of the following is true about end-of-life care?
(c) The patient's own wishes should always be respected
Autonomy is paramount in end-of-life care. Patients have the right to refuse any treatment, including artificial nutrition/hydration, CPR, and hospitalization. This is protected by law and ethics. Respecting wishes may mean allowing natural death, stopping ineffective treatments, or focusing only on comfort. This is the principle of self-determination in palliative care.
END-OF-LIFE PRINCIPLES: "RESPECT" - Respect autonomy, Elicit wishes, Support family, Palliate symptoms, Evaluate futility, Comfort focus, Time to let go
19
Which of the following is NOT a sign of actual death?
(a) Decreasing fluid and food intake
Decreasing intake is a sign of APPROACHING death (days to weeks before), not actual death. It's part of the pre-active dying phase as the body naturally shuts down. Actual death signs are: cessation of breathing, heartbeat, pulse, fixed pupils, and rigor mortis (stiffness) occurring AFTER death. Decreased intake is reversible and not diagnostic of death.
⚰️ DEATH SIGNS: No respiration, No heart sounds, No pulse, Fixed dilated pupils, Pale skin, Rigor mortis. Always confirm with 2nd nurse/doctor.
20
Which of the following is a psychological symptom of stress?
(d) Low self esteem
Low self-esteem is a psychological manifestation of chronic stress in palliative patients. It reflects negative self-evaluation, feelings of worthlessness, and loss of identity due to functional decline, dependency, and body image changes. It affects coping and quality of life. Other options are cognitive (indecision, poor concentration) or physiological (inability to relax) symptoms rather than purely psychological.
STRESS SYMPTOMS: "PENCIL" - Physical, Emotional, Cognitive, Interpersonal, Behavioral, Lifestyle changes
Filling in the blank spaces (10 Marks)
21
The active total care of patients with advanced chronic illness that focuses on patient's quality of life rather than cure is called
Palliative care
World Health Organization (WHO) Definition: Palliative care is an approach that improves quality of life of patients and their families facing life-threatening illness, through prevention and relief of suffering by means of early identification, assessment and treatment of pain and other problems - physical, psychosocial and spiritual. It affirms life and regards dying as a normal process.
22
The type of pain that arises from damage to body tissues and is usually localized is termed as
Nociceptive pain (or somatic pain)
Nociceptive pain results from activation of peripheral nociceptors due to tissue injury, inflammation, or mechanical damage. It is typically well-localized, described as aching, throbbing, or sharp. Two types: somatic (skin, muscle, bone) and visceral (internal organs). Responds well to opioids and NSAIDs. Differs from neuropathic pain which involves nerve damage.
23
Progressive care given to a palliative care patient and family from the time of diagnosis to bereavement period is called
Continuity of care/continuum of care
Continuity of care ensures seamless support across settings and time, from diagnosis through treatment, progression, dying, death, and bereavement. Involves coordination between hospital, home, hospice, and community services. The family is the unit of care throughout. This longitudinal approach builds trust and addresses evolving needs predictively rather than reactively.
24
The process of enabling and helping a patient to make a particular decision is termed as
Shared decision-making
Patient empowerment through Shared decision-making is central to palliative care ethics. It involves providing information, exploring values, and supporting autonomy so patients can make informed choices consistent with their goals. Includes advance care planning, informed consent, and respecting preferences. The nurse acts as facilitator, not director, helping patients articulate and implement their wishes.
25
Emotional response associated with loss is called
Grief
Grief is the complex emotional response to loss - sadness, anger, guilt, denial, bargaining, acceptance. It is universal, individual, and non-pathological. Mourning is the outward expression of grief. Anticipatory grief begins before death in terminal illness. Complicated grief requires clinical intervention. Nurses must normalize grief and provide supportive presence.
26
The period from diagnosis of a chronic illness to the time one copes with the situation is called
Adjustment period
The Adjustment period or sometimes illness trajectory describes the course of chronic illness from diagnosis through decline to death. It includes phases of crisis, stabilization, decline, and dying. Each phase has different care needs. Understanding the trajectory helps nurses anticipate challenges, provide timely interventions, and support adaptive coping. The "transition point" from curative to palliative focus is a critical phase.
27
Migration of cancerous cells from the site of origin to other parts of the body forming secondary tumours is called
Metastasis
Metastasis is the spread of cancer cells from primary site to distant organs via blood, lymphatics, or body cavities. It signifies advanced disease and is the major cause of cancer mortality. Common sites: lung, liver, bone, brain. Metastatic disease often determines prognosis and treatment goals (palliative vs curative). Pain from bone metastasis is a common palliative care issue.
28
The scale used to assess pain in children by using different colours to depict different level of pain is
Wong bakers Faces Pain Scale - Revised Color Analog scale
The wong bakers Faces Pain Scale shows 6 faces from smiling (no pain) to crying (worst pain). Children point to the face that matches their pain. Colour can be incorporated (green to red). Validated for ages 4-12 years. The Oucher Scale uses photographs of children's faces. These tools make pain assessment developmentally appropriate for non-verbal or young children who cannot use numeric rating scales. 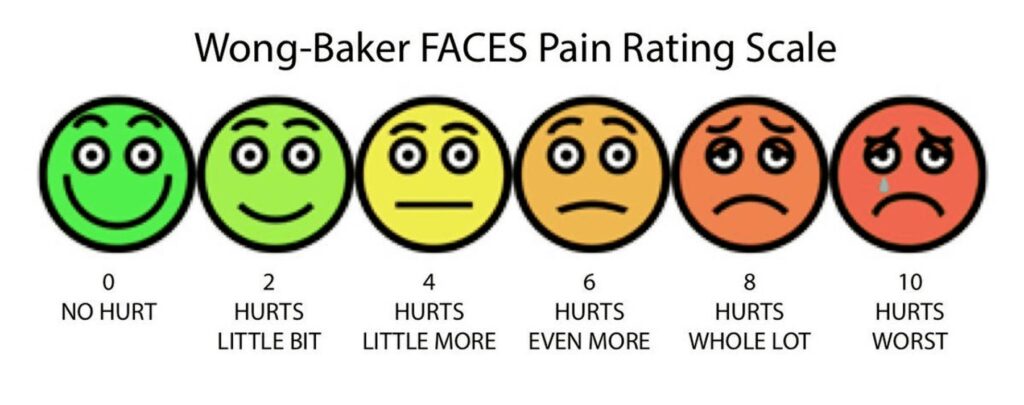
29
When a patient's responses to stress are ineffective, they are referred to as
Maladaptive coping (or Dysfunctional coping)
Maladaptive coping worsens the situation or creates new problems. Examples in palliative care: denial preventing treatment decisions, substance abuse for pain, social withdrawal increasing isolation, aggression damaging relationships. Contrast with adaptive coping (seeking information, expressing emotions, using support). Nurses help patients develop adaptive strategies through counseling and support.
30
Difficult in swallowing is referred to as
Dysphagia
Dysphagia is common in advanced cancer (head/neck, oesophageal, neurological) and end-of-life. Causes: obstruction, mucositis, xerostomia, muscle weakness, CNS involvement. Leads to malnutrition, dehydration, aspiration pneumonia. Management includes texture modification, positioning, swallowing therapy, and in end-of-life, decisions about artificial nutrition vs comfort feeding only.
SECTION B: Short Essay Questions (10 marks)
31
Outline five (5) reasons why it is important for nurses and midwives to break bad news to the patient of cancer and his/her family. (5 marks)
1. Respects patient autonomy and right to know: Patients have legal and ethical right to information about their diagnosis, prognosis, and treatment options to make informed decisions about their care and life planning.
2. Facilitates informed decision-making and advance care planning: Enables patients to participate in treatment choices, set realistic goals, complete advance directives, and arrange personal affairs while mentally competent.
3. Reduces anxiety and uncertainty: Not knowing often causes more suffering than knowing the truth. Open communication decreases fear of the unknown and allows psychological adjustment.
4. Builds trust in therapeutic relationship: Honest communication demonstrates respect, compassion, and professionalism, strengthening nurse-patient-family bonds essential for effective care.
5. Promotes realistic expectations and reduces false hope: Helps families understand disease trajectory, prepares them for decline, and prevents pursuit of futile aggressive treatments that may increase suffering.
32
Outline five (5) specific interventions that should be implemented to promote effective coping to living a life with cancer. (5 marks)
1. Psychoeducation about disease and treatment: Provide clear, understandable information about diagnosis, treatment options, side effects, and self-care strategies to reduce uncertainty and increase sense of control.
2. Establish strong support systems: Facilitate family meetings, connect with support groups (peer survivors), involve spiritual care, and identify community resources to combat isolation.
3. Teach adaptive coping strategies: Introduce mindfulness, relaxation techniques, guided imagery, journaling, and problem-solving skills to manage anxiety, pain, and treatment side effects.
4. Promote realistic hope and goal setting: Help patients identify achievable short-term goals, find meaning in daily life, celebrate small victories, and maintain a sense of purpose beyond cure.
5. Facilitate open communication and emotional expression: Create safe space for patients to express fears, anger, and sadness; use active listening, validate feelings, and encourage life review and legacy activities.
CANCER COPING: "SUPPORT" - Share information, Understand feelings, Problem-solve, Participate in care, Open communication, Realistic hope, Talk about meaning
SECTION C: Long Essay Questions (60 Marks)
33
(a) Describe ten (10) features that should be checked for during comprehensive pain assessment in a patient with cancer. (10 marks)
(b) Outline ten (10) non-pharmacologic measures nurses should implement to manage pain in a patient with cancer. (10 marks)
(b) Outline ten (10) non-pharmacologic measures nurses should implement to manage pain in a patient with cancer. (10 marks)
(a) Comprehensive Cancer Pain Assessment Features:
1. Pain intensity: Use numeric rating scale (0-10), verbal descriptor scale, or faces scale to quantify severity and track changes over time.
2. Location and radiation: Ask patient to point to pain site on body diagram; identify if pain radiates and map its distribution.
3. Pain quality and character: Use patient's own words (sharp, dull, burning, throbbing) to differentiate nociceptive vs neuropathic pain.
4. Temporal pattern: Assess onset, duration, frequency; identify if constant vs intermittent, breakthrough pain, and daily patterns.
5. Aggravating and relieving factors: Identify activities, positions, treatments that worsen or improve pain to guide interventions.
6. Physiological responses: Observe for tachycardia, hypertension, sweating, muscle tension, guarding, and facial grimacing.
7. Impact on function and sleep: Assess ADL limitations, mobility restrictions, sleep disturbance, and appetite changes.
8. Emotional and cognitive components: Evaluate for anxiety, depression, fear, catastrophizing, and pain beliefs that amplify suffering.
9. Current analgesic regimen and response: Document all pain medications, doses, timing, effectiveness, and side effects experienced.
10. Patient's pain goal and expectation: Ask "What pain level is acceptable?" and "What activities do you want to be able to do?" to individualize targets.
(b) Non-Pharmacologic Pain Management Measures:
1. Patient education and reassurance: Explain pain mechanisms, treatment plan, and that pain can be controlled to reduce anxiety that amplifies pain.
2. Positioning and comfort measures: Use pillows to support painful areas, frequent repositioning every 2 hours, and pressure relief to prevent bedsores.
3. Relaxation and breathing techniques: Teach deep breathing, progressive muscle relaxation, and guided imagery to reduce muscle tension and anxiety.
4. Distraction and activity engagement: Use music therapy, reading, TV, conversation, and gentle activities to shift focus from pain.
5. Massage and therapeutic touch: Gentle massage of non-painful areas promotes comfort, reduces muscle tension, and provides human connection.
6. Application of heat or cold: Warm compresses for muscle spasm; cold packs for inflammatory pain and bone pain; duration 15-20 minutes.
7. Transcutaneous electrical nerve stimulation (TENS): Low-voltage electrical stimulation blocks pain signals and releases endorphins; useful for neuropathic pain.
8. Aromatherapy and complementary therapies: Lavender, peppermint oils for relaxation; acupuncture/acupressure for selected patients.
9. Facilitating spiritual practices: Prayer, meditation, rituals provide comfort and meaning that reduces suffering perception.
10. Environmental modifications: Control noise, lighting, temperature; provide comfortable bedding and familiar personal items to create healing environment.
💊 Non-Pharmacologic ≠ Non-Effective! These measures enhance drug therapy, reduce opioid doses, and address suffering that drugs cannot touch. Always combine with pharmacologic treatment.
34
(a) Outline ten (10) challenges that family care givers of patients diagnosed with cancer face. (10 marks)
(b) Outline five (5) expected outcomes for a family caregiver who has just been informed of a cancer diagnosis for her sick loved relative. (5 marks)
(c) Outline five (5) roles of nurses working on a palliative care unit. (5 marks)
(b) Outline five (5) expected outcomes for a family caregiver who has just been informed of a cancer diagnosis for her sick loved relative. (5 marks)
(c) Outline five (5) roles of nurses working on a palliative care unit. (5 marks)
(a) Challenges for Family Caregivers of Cancer Patients:
1. Physical exhaustion and caregiver burden: Providing 24/7 care, assisting with ADLs, managing medications, and lack of sleep leading to burnout and health problems.
2. Financial hardship: Lost income from quitting jobs, medical expenses, transportation costs, and purchasing special equipment creating economic strain.
3. Emotional distress and anticipatory grief: Watching loved one suffer, fear of impending death, anxiety, depression, and helplessness.
4. Lack of knowledge and skills: Uncertainty about how to manage symptoms, give medications, provide personal care, and recognize emergencies.
5. Social isolation: Reduced social activities, friends withdrawing due to discomfort with illness, and lack of time for self-care or other relationships.
6. Communication difficulties: Struggling to talk about prognosis with patient, family disagreements about care decisions, and difficulty expressing emotions.
7. Role changes and relationship strain: Shifting from spouse/partner to nurse role, loss of intimacy, and changing family dynamics causing resentment.
8. Inadequate support from healthcare system: Limited home care services, poor coordination, unclear instructions, and feeling abandoned by providers.
9. Balancing multiple responsibilities: Managing own household, childcare, work obligations while caregiving leading to role overload.
10. Spiritual distress and existential questioning: Questioning meaning of suffering, struggling with faith, and searching for purpose in the experience.
(b) Expected Outcomes for Family Caregiver After Cancer Diagnosis:
1. Demonstrates understanding of diagnosis and prognosis: Verbalizes key information about cancer type, stage, treatment goals, and expected course.
2. Identifies available support resources: Lists support groups, financial assistance, respite care, and community services available to help with caregiving.
3. Expresses emotions appropriately: Acknowledges feelings of fear, sadness, anger and seeks support rather than suppressing emotions.
4. Participates in care planning: Actively engages in treatment decisions, asks questions, and collaborates with healthcare team on care goals.
5. Accesses respite care and self-care strategies: Recognizes personal limits, arranges periodic relief from caregiving duties, and maintains own health to sustain caregiving role.
(c) Roles of Nurses Working on a Palliative Care Unit:
1. Expert symptom management: Assess and manage complex pain, dyspnea, nausea, delirium, and other distressing symptoms using both pharmacologic and non-pharmacologic interventions.
2. Care coordinator and case manager: Organize multidisciplinary team meetings, arrange home care services, coordinate referrals, and ensure seamless transitions between care settings.
3. Family educator and counselor: Teach caregivers about disease progression, medication administration, symptom monitoring, and provide emotional support, anticipatory guidance, and bereavement counseling.
4. Advance care planning facilitator: Guide patients and families through discussions about goals of care, treatment preferences, DNAR orders, and completion of advance directives.
5. Advocate for patient wishes: Ensure patient preferences are respected, communicated to all team members, and implemented in care plans; protect vulnerable patients from unwanted interventions.
🤝 Nurse as Linchpin! Palliative care nurses coordinate the entire care ecosystem - medical, psychosocial, spiritual, and practical. You're the glue that holds it together for patients and families.
35
(a) Explain five (5) stages of grief experienced by children after loss. (10 marks)
(b) Outline ten (10) ways through which nurses should help a bereaved family or person. (10 marks)
(b) Outline ten (10) ways through which nurses should help a bereaved family or person. (10 marks)
(a) Stages of Grief in Children:
1. Denial and shock: Young children may not comprehend death's permanence, expecting the deceased to return. They may continue to ask for the person, think they're sleeping, or deny the reality. This serves as emotional protection from overwhelming loss.
2. Anger and acting out: Children may express anger at the deceased for leaving, at surviving family members, or at God. This manifests as tantrums, aggression, defiance, or regression to earlier behaviors (bedwetting, thumb-sucking).
3. Bargaining and magical thinking: Children may believe they can reverse death through good behavior, promises, or special thoughts. Common in school-age children who think "If I'm very good, maybe mommy will come back." This reflects developmental understanding of causality.
4. Depression and withdrawal: As reality sets in, children may become sad, lose interest in play, experience sleep and appetite disturbances, and socially withdraw. May express somatic complaints (stomachaches, headaches) instead of emotional pain.
5. Acceptance and reintegration: Eventually children accept the loss, remember the deceased with sadness but not incapacitating grief, and resume normal activities. They incorporate the loss into their life story and may find meaning through memories, legacies, and maintaining bonds through remembrance activities.
CHILD GRIEF: "DABDA-C" - Denial, Anger, Bargaining, Depression, Acceptance (with Concrete thinking, Crying, Confusion)
👶 Age Matters! Under 5: death is temporary; 5-9: begin to understand permanence; 10+: grasp finality but struggle with existential meaning. Adapt your language and expectations!
(b) Ways Nurses Should Help Bereaved Families:
1. Be present and listen actively: Offer silent support, sit with family, listen without trying to "fix" their grief, and allow them to express emotions without judgment.
2. Provide information about what to expect: Explain normal grief reactions, that grief has no timeline, and that varied emotions (anger, guilt, relief) are normal.
3. Offer practical assistance: Help with notification of other family members, funeral home arrangements, collecting belongings, and completing paperwork.
4. Create a memory keepsake: Offer handprints, lock of hair, photos, or memory box items that families can treasure as tangible connections to their loved one.
5. Provide bereavement literature and resources: Give written materials about grief, support group information, counselor contacts, and community resources for ongoing support.
6. Follow-up phone call or visit: Contact family within 2-4 weeks after death to check on wellbeing, answer questions, and identify complicated grief requiring intervention.
7. Acknowledge the loss formally: Send condolence card, attend funeral if appropriate, and make a memorial donation if family wishes - shows continuing caring relationship.
8. Screen for complicated grief and depression: Use tools like Persistent Complex Bereavement Disorder criteria to identify those needing mental health referral.
9. Facilitate family meetings: Bring family together to share memories, express feelings, and support each other, especially if there were conflicts or unresolved issues.
10. Take care of your own grief: Recognize that caring for dying patients creates attachment and loss; seek peer support, debriefing, and counseling to prevent compassion fatigue and continue effective care for others.
💔 Bereavement care continues after death! The nurse's role doesn't end at death - it's just beginning for the family. Follow-up is crucial for identifying complicated grief.
Enable Notifications
OK
No thanks