
Respiratory System Anatomy: Breathe In, Breathe Out!
To exhaustively describe the macroscopic and microscopic anatomy of the respiratory system and relate structural morphology to its fundamental functions in the processes of air conduction, gas exchange, and physiological protection. This comprehensive guide leaves no stone unturned, detailing everything from embryological development to complex clinical pathologies.
1. Introduction to the Respiratory System
The respiratory system is a highly intricate, dynamic network of organs, tissues, and muscular pumps that work in perfect harmony to move air into and out of the body, facilitating the ultimate goal: Gas Exchange. It is a vital biological system absolutely responsible for the exchange of gases between the body's internal circulation and the external atmosphere.
Its primary physiological function is to take in oxygen (O₂) from the atmosphere—required by every cell in the body to produce ATP (energy)—and expel carbon dioxide (CO₂), a toxic waste product of cellular metabolism. This continuous, rhythmic process, known as respiration, is not only essential for energy production but also serves as a primary mechanism for maintaining the body's delicate pH balance (acid-base homeostasis).
The respiratory system can be broadly divided in two distinct ways:
1. Functionally: The Conducting Zone (for transporting, warming, and cleaning air) and the Respiratory Zone (the actual site of gas exchange).
2. Anatomically: The Upper Respiratory Tract (everything above the vocal cords) and the Lower Respiratory Tract (everything below the vocal cords).
2. Upper Respiratory Tract (The Conducting Zone)
This upper portion of the system is primarily involved in conditioning the inspired air. Before air ever reaches the delicate lung tissue, it must be aggressively filtered, warmed, and humidified.
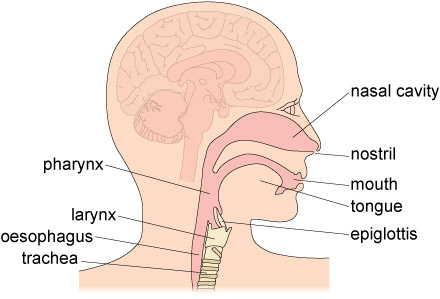
A. The Nose and Nasal Cavity
- External Nose: The visible protruding part of the face, supported superiorly by the nasal bones and inferiorly by pliable hyaline cartilage.
- Nasal Cavity: A large, hollow space extending from the anterior nostrils (nares) all the way back to the posterior nasal apertures (choanae), which open into the throat.
- Vestibule: The anterior-most, dilated part of the nasal cavity just inside the nostrils. It is lined with skin and heavily populated with stiff, coarse hairs called vibrissae that act as the first line of defense, filtering out large particulate matter like dust and insects.
- Nasal Conchae (Turbinates): Three distinct bony projections on the lateral walls of the nasal cavity—the superior, middle, and inferior conchae. They are highly vascularized and covered by thick mucous membranes.
The Essential Function of Turbinates & Mucosa
The conchae are not just anatomical bumps; they are brilliant bio-engineering. They dramatically increase the surface area of the nasal cavity and force inhaled air to swirl around in a turbulent flow rather than moving in a straight line. This turbulence forces inhaled air molecules to constantly bounce against the moist, warm mucous membranes, which effectively:
- Filters: Traps microscopic dust, pollen, bacteria, and other particulate matter in the sticky mucus.
- Warms: Heat radiates from the underlying capillary beds (a rich vascular network known as Kiesselbach's plexus), instantly warming cold environmental air to body temperature (37°C) to prevent shocking the lungs.
- Humidifies: Water vapor evaporating from the mucus completely saturates the inhaled air with moisture, preventing the drying out and cracking of the delicate alveolar tissues deep in the lungs.
Mucosal Types in the Nasal Cavity:
- Olfactory Mucosa: Located strictly in the superior-most roof of the nasal cavity; it contains specialized olfactory receptors for the sense of smell. These nerve fibers pass directly through the cribriform plate of the ethmoid bone into the brain.
- Respiratory Mucosa: Lines the vast majority of the nasal cavity. It is composed of pseudostratified ciliated columnar epithelium packed with abundant goblet cells.
- Goblet Cells: Specialized glandular cells that continuously produce and secrete a thick sheet of sticky mucus.
- Cilia: Microscopic hair-like projections that beat rapidly and rhythmically to move the contaminated mucus backwards towards the pharynx, where it is swallowed and destroyed by stomach acid. This continuous sweeping is known as the mucociliary escalator.
Paranasal Sinuses
These are four paired, air-filled cavities located within the frontal, sphenoid, ethmoid, and maxillary bones surrounding the nasal cavity. They serve several functions: they significantly lighten the weight of the skull, provide additional surface area to warm and humidify air, and act as resonance chambers to amplify and deepen the sound of your voice. They drain their mucus directly into the nasal cavity.
Sinusitis & Epistaxis
Sinusitis: When a viral or bacterial infection inflames the respiratory mucosa, the tissue swells. This swelling easily blocks the tiny drainage ducts of the paranasal sinuses. Mucus becomes trapped inside the sinus cavities, creating a perfect breeding ground for bacteria and causing severe pressure headaches and facial pain.
Epistaxis (Nosebleed): To warm the air efficiently, the nasal cavity requires massive blood flow. The anterior nasal septum contains a highly vascularized area called Kiesselbach's plexus. Because these vessels are very superficial, dry air, trauma (nose-picking), or high blood pressure can easily rupture them, leading to profuse bleeding.
B. The Pharynx (Throat)
The pharynx is a muscular, funnel-shaped tube extending from the posterior nasal cavity all the way down to the esophagus and larynx. It serves as a vital dual-purpose passageway for both air (to the lungs) and food/liquids (to the stomach).
It is divided into three distinct anatomical regions:
- Nasopharynx: Located directly posterior to the nasal cavity. Because it only ever handles air, it remains lined with respiratory epithelium (pseudostratified ciliated columnar). It houses the pharyngeal tonsils (adenoids) on its posterior wall and the openings of the auditory (Eustachian) tubes, which connect to the middle ear to equalize pressure.
- Oropharynx: Located posterior to the oral cavity (mouth). Because both air and abrasive, rough food pass through here, the lining dramatically shifts to stratified squamous epithelium to resist friction and wear-and-tear. It contains the palatine tonsils and the lingual tonsils at the base of the tongue.
- Laryngopharynx: Extends downwards from the epiglottis to the point where the digestive and respiratory tracts diverge (the esophagus and the larynx). It is also lined with robust stratified squamous epithelium to handle the passage of food.
C. The Larynx (Voice Box)
The larynx is a complex, primarily cartilaginous structure that connects the pharynx to the trachea. It is the gateway to the lower respiratory tract.
Main Cartilages of the Larynx
- Thyroid Cartilage: The largest, shield-shaped cartilage. Its anterior prominence forms the "Adam's apple" (laryngeal prominence), which is more pronounced in males due to testosterone.
- Cricoid Cartilage: A complete, signet-ring-shaped cartilage located inferior to the thyroid cartilage. It forms the solid base of the larynx and connects it to the trachea.
- Epiglottis: A highly flexible, leaf-shaped flap of elastic cartilage anchored to the inner rim of the thyroid cartilage. It acts as the guardian of the airways (the glottis). During the act of swallowing, the entire larynx is pulled upward, causing the epiglottis to tip backwards like a lid, completely sealing off the opening to the trachea and preventing food or liquid from being aspirated into the lungs.
- Arytenoid, Corniculate, & Cuneiform Cartilages: Small, paired cartilages located posteriorly. The arytenoid cartilages are particularly important as they anchor the vocal cords and pivot to control vocal cord tension and positioning.
Vocal Folds & Function
Vocal Folds (True Vocal Cords): These are tough, pearly-white elastic ligaments covered by a mucous membrane, stretching horizontally across the interior of the larynx. They vibrate intensely to produce sound as exhaled air rushes over them. The tension, length, and position of these folds are controlled by intricate, tiny intrinsic laryngeal muscles.
Functions of the Larynx:
- Air Passageway: Its rigid cartilage skeleton keeps the airway permanently patent (open).
- Phonation: The primary organ for voice production.
- Sphincter Action (Valsalva Maneuver): The vocal cords can forcefully clamp shut to trap air in the lungs. This raises intra-abdominal pressure to help empty the rectum (defecation) or stabilize the body trunk when lifting heavy objects.
- Prevention of Aspiration: Through the action of the epiglottis and vocal cord closure during swallowing.
3. Lower Respiratory Tract (Conducting and Respiratory Zones)
This portion begins at the base of the neck, enters the thoracic cavity, and branches extensively deep into the lungs.
A. The Trachea (Windpipe)
The trachea is a tough, flexible, rigid tube extending from the inferior edge of the larynx (around cervical vertebra C6) down through the mediastinum to the point where it bifurcates (around thoracic vertebra T4/T5).
- Structure: It is structurally supported by 16 to 20 stacked, C-shaped rings of hyaline cartilage.
- Function of Cartilage Rings: These hard rings are absolutely crucial; they prevent the trachea from collapsing inward under the negative pressure generated during inhalation, ensuring a permanently patent (open) airway.
- The Trachealis Muscle: The posterior aspect of the C-rings is entirely open (meaning the rings do not form a full circle). This gap is bridged by smooth muscle called the trachealis muscle. Because the esophagus sits directly behind the trachea, this soft posterior wall allows the esophagus to expand anteriorly into the tracheal space when you swallow large chunks of food.
- Lining: Similar to the nasal cavity, it is lined with pseudostratified ciliated columnar epithelium rich in goblet cells, maintaining a robust mucociliary escalator that traps deep lung debris and aggressively sweeps it upwards towards the pharynx.
- The Carina: The internal ridge situated exactly at the point where the trachea bifurcates into the left and right main bronchi. The mucosa here is incredibly sensitive; even the slightest touch from a foreign object or fluid triggers a violent, uncontrollable cough reflex to expel the hazard.
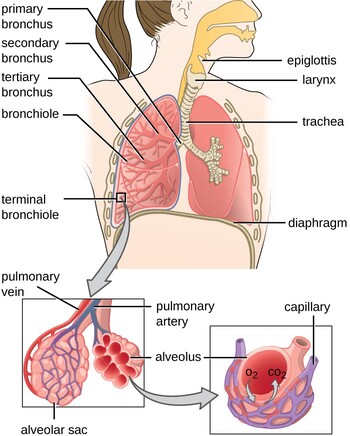
B. The Bronchi (The Bronchial Tree)
At the carina, the trachea divides into two main (primary) bronchi, one traveling into each lung.
Anatomically, the Right Main Bronchus is significantly shorter, wider, and runs more vertically (steeper angle) than the left main bronchus. Because it represents a more direct, straight-down pathway from the trachea, accidentally inhaled (aspirated) foreign objects—such as coins, peanuts, or vomit—are much more likely to lodge in the right lung than the left.
Once inside the lungs, the branching continues rapidly, resembling an inverted tree:
- Main (Primary) bronchi enter the hilum of each lung and immediately divide into:
- Lobar (Secondary) bronchi: There are three on the right (supplying the superior, middle, and inferior lobes) and two on the left (supplying the superior and inferior lobes).
- Segmental (Tertiary) bronchi: These branch further to supply specific, surgically isolatable sectors of the lung called bronchopulmonary segments (typically 10 in the right lung and 8-10 in the left).
Structural Changes down the Tree: As the tubes get smaller, structural changes occur. The rigid cartilage rings of the trachea break up into irregular cartilage plates in the bronchi, eventually disappearing entirely. Simultaneously, the amount of smooth muscle in the walls heavily increases, allowing the nervous system to control the diameter of the airway.
C. The Bronchioles
When the conducting airways branch down to a diameter of less than 1 millimeter and completely lose all cartilage support, they are officially termed bronchioles.
- Terminal Bronchioles: These represent the absolute final, smallest branches of the conducting zone. Air here is just flowing, not exchanging. The epithelium thins out to simple cuboidal.
- Club Cells (Clara cells): Found extensively in terminal bronchioles. These are non-ciliated cells that secrete a component of surfactant to prevent the small airways from sticking shut. They also contain cytochrome P450 enzymes to detoxify airborne toxins, and they act as stem cells to regenerate damaged airway lining.
- Function: Because bronchioles lack rigid cartilage and consist almost entirely of smooth muscle, they are the primary site of airway resistance control. The autonomic nervous system acts here: Sympathetic nerves cause massive bronchodilation (opening), while parasympathetic nerves cause bronchoconstriction (narrowing).
D. The Respiratory Zone (Respiratory Bronchioles & Alveolar Ducts)
This is where the magic of gas exchange finally begins.
- Respiratory Bronchioles: The terminal bronchioles divide into these. They are distinguished by the sudden appearance of scattered, balloon-like alveoli budding directly off their walls. Because alveoli are present, minimal gas exchange can occur here.
- Alveolar Ducts: The respiratory bronchioles divide into alveolar ducts, which are essentially straight tubes composed almost entirely of rings of alveoli.
- Alveolar Sacs: The ducts terminate in blind-ended clusters of alveoli called alveolar sacs, visually resembling a dense bunch of grapes. These represent the primary site of maximum gas exchange.
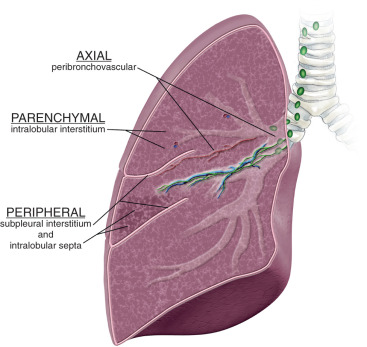
4. Lung Parenchyma and The Alveoli
The functional, spongy tissue of the lungs is known as the parenchyma, heavily dominated by the alveoli.
A. The Alveoli (The Air Sacs)
Alveoli are microscopic, incredibly thin-walled air sacs. A healthy adult possesses an astonishing 300 to 500 million alveoli per lung. Collectively, they expand the internal surface area of the lungs to approximately 70 to 100 square meters (roughly the size of a tennis court), providing a massive surface for gas diffusion.
The alveolar wall is an active biological frontier comprised of specific cell types:
Squamous Alveolar Cells
These are extremely thin, flattened epithelial cells (0.1 to 0.5 micrometers thick). Although they are fewer in absolute number, their vast, flattened shape covers 95% of the total alveolar surface area. They form the primary structural wall of the alveolus and are the main site of gas exchange. Their extreme thinness minimizes the diffusion distance for oxygen and carbon dioxide.
Septal / Secretory Cells
These are chubby, cuboidal cells interspersed sporadically among the flat Type I cells. They have two vital functions:
- Surfactant Production: They constantly secrete pulmonary surfactant, a complex mixture of phospholipids and proteins that coats the inner surface of the alveolus.
- Cellular Repair: They act as progenitor (stem) cells. If Type I cells are damaged by toxins or infections, Type II cells multiply and differentiate into new Type I cells to patch the holes.
"Dust Cells"
These are aggressive, wandering phagocytic white blood cells that patrol the alveolar surface. Because the mucociliary escalator does not reach down into the alveoli, these macrophages are the last line of defense. They literally crawl around, actively engulfing and destroying inhaled dust particles, pollen, bacteria, and dead cell debris. When full, they migrate up into the bronchioles to be swept away or enter the lymphatic system.
Physics of the Lungs: Surfactant and LaPlace's Law
Why is surfactant so critical? The inside of an alveolus is lined with a thin layer of water. Water molecules are highly attracted to each other (surface tension). Without surfactant, the surface tension of this water would be so strong that it would pull the delicate walls of the alveolus inward, collapsing the lung entirely every time you exhaled (atelectasis).
According to LaPlace's Law, smaller spheres have a higher collapsing pressure than larger ones. Surfactant uniquely intersperses between water molecules, destroying their attraction to each other. This drastically lowers surface tension, prevents alveolar collapse during expiration, and severely reduces the muscular effort (work of breathing) required to inflate the lungs on the next breath.
B. The Alveolar-Capillary Membrane (Respiratory Membrane)
This is the ultimate barrier that gases must cross to move between the inhaled air and the bloodstream. It is an evolutionary marvel, measuring a mere 0.2 to 0.6 micrometers in thickness to optimize the rapid diffusion rate defined by Fick's Law.
It consists of distinct layers (from the air side to the blood side):
- The very thin layer of alveolar fluid containing the vital surfactant.
- The extremely thin cytoplasm of the alveolar epithelial cell (Type I pneumocyte).
- A fused basement membrane shared by both the alveolar epithelium and the capillary endothelium.
- The cytoplasm of the capillary endothelial cell.
The Interstitium: In some areas, there is a tiny connective tissue space between the epithelial and endothelial basement membranes containing elastic and collagen fibers.
Clinical Note: In diseases like Pulmonary Edema (fluid in the lungs) or Pulmonary Fibrosis (scarring), this interstitium becomes thick and swollen. This massively increases the distance oxygen has to travel, leading to severe hypoxia (oxygen starvation in the blood).
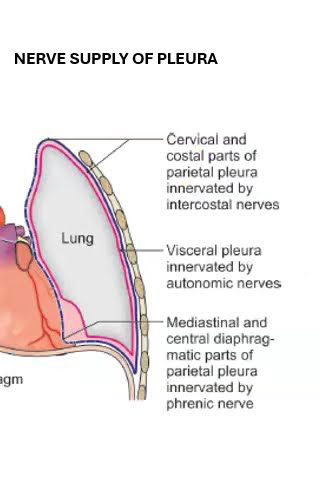
5. The Pleura and its Nerve Supply
The pleura are double-layered serous membranes that envelop the lungs and line the walls of the thoracic cavity.
A. The Pleural Layers
- Visceral Pleura: Directly covers the entire surface of the lungs, dipping deep into the fissures between the lobes. It is thin, transparent, and firmly adherent to the lung tissue.
- Innervation & Sensitivity: Supplied by autonomic nerves from the pulmonary plexus (Vagus nerve for parasympathetic, and Sympathetic trunks). It is completely insensitive to pain, touch, and temperature, but contains stretch receptors. (Clinical significance: Lung tumors do not cause pain until they invade the parietal pleura).
- Parietal Pleura: Lines the inner surface of the thoracic cavity. It is subdivided based on the region it lines:
- Cervical Pleura (Cupola): Extends superiorly into the neck, covering the lung apex.
- Costal Pleura: Lines the inner surface of the ribs and intercostal muscles.
- Mediastinal Pleura: Covers the lateral aspect of the mediastinum.
- Diaphragmatic Pleura: Covers the superior surface of the diaphragm.
- Innervation & Sensitivity: Supplied by somatic sensory nerves. It is highly sensitive to pain, touch, temperature, and pressure.
-> The Intercostal nerves supply the costal pleura.
-> The Phrenic nerves supply the mediastinal and central diaphragmatic pleura. (Clinical significance: Inflammation here causes sharp pleuritic chest pain. Phrenic nerve irritation can cause referred pain to the shoulder tip).
The Pleura and Mechanics of Breathing
The lungs themselves contain absolutely no skeletal muscle; they cannot expand or contract on their own. They rely entirely on the volume changes of the thoracic cage, mediated by the pleura.
A. The Pleural Layers
The lungs are hermetically sealed within double-layered serous membranes called the pleura.
- Visceral Pleura: The inner layer that firmly and inextricably attaches directly to the entire surface of the lung tissue, dipping deep into the fissures between the lobes. (Innervation: Autonomic nerves; completely insensitive to sharp pain, but sensitive to stretch).
- Parietal Pleura: The outer layer that lines the inner surface of the thoracic cavity, the mediastinum, and the superior surface of the diaphragm. (Innervation: Somatic intercostal and phrenic nerves; highly sensitive to sharp pain, touch, and temperature).
B. The Pleural Cavity & Pleural Fluid
The pleural cavity is the microscopic potential space between the visceral and parietal layers. It is completely sealed and contains a very small amount (10-20 mL) of serous pleural fluid secreted by the membranes.
Functions of the Pleura and its Fluid:
- Lubrication: It drastically reduces friction, allowing the lungs to glide silently and effortlessly against the chest wall during the tens of thousands of breaths taken every day.
- Surface Tension (The Suction Cup Effect): Just like two wet panes of glass stuck together, the pleural fluid creates a massive cohesive surface tension. Because the chest wall naturally wants to spring outward and the elastic lungs naturally want to recoil inward, this suction creates a constant negative intrapleural pressure (around -4 mmHg). This suction physically binds the lung to the chest wall. When the chest expands, it forcibly pulls the lungs open with it.
Clinical Correlate: Pneumothorax & Pleurisy
Pneumothorax: If a stab wound (or a ruptured lung blister) punctures the pleura, air rushes into the pleural cavity. The vacuum seal is instantly broken, the negative pressure is lost, and the lung's natural elasticity causes it to instantly recoil and collapse into a small ball.
Pleurisy (Pleuritis): Inflammation of the pleural membranes. Because the parietal pleura is highly innervated with pain fibers, when the inflamed, roughened surfaces rub against each other during breathing, it causes agonizing, sharp, stabbing chest pain with every single breath.
C. Pleural Recesses
These are "empty" areas where the parietal pleura extends further down than the resting lung borders, creating deep pockets.
- Costodiaphragmatic Recess: The largest, deepest recess located at the very bottom of the rib cage where it meets the diaphragm. Because it is the lowest anatomical point of the thoracic cavity when a person is standing upright, it is the primary site where abnormal fluid (blood, pus, or edema) pools in gravity-dependent conditions like pleural effusions. Physicians use a needle here (thoracentesis) to drain excess fluid safely without hitting the lung.
D. The Respiratory Muscles
Breathing relies on Boyle's Law: If you increase the volume of a closed container, the pressure inside drops. Muscles increase the volume of the chest, creating negative pressure, which sucks air into the lungs.
Primary Muscles of Inspiration (Active Process)
- The Diaphragm: The primary engine of breathing. A large, dome-shaped parachute of skeletal muscle separating the chest from the abdomen. When stimulated by the Phrenic Nerves (C3-C5), it contracts, flattens out, and pushes down into the abdomen. This massively increases the vertical height of the thoracic cavity.
- External Intercostal Muscles: Located between the ribs. When they contract, they pull the entire rib cage upwards and outwards (like a bucket handle), increasing the side-to-side and front-to-back dimensions of the chest.
Muscles of Expiration (Passive/Active)
- Normal Expiration: A completely passive process. You simply stop flexing the inspiration muscles. The diaphragm relaxes and bows upward, and the elastic lungs naturally snap back to their original size, forcing air out.
- Forced Expiration: When blowing out candles or during exercise, expiration becomes active. The Internal Intercostal Muscles contract to violently pull the ribs down and inward. Simultaneously, the abdominal muscles contract, forcefully pushing the abdominal organs up into the diaphragm to crush the air out of the lungs.
6. Key Functions of the Respiratory System Summarized
- Ventilation (Breathing): The mechanical, muscular process of moving bulk air into (inhalation) and out of (exhalation) the lungs.
- Gas Exchange: The diffusion of O₂ and CO₂ between the lungs and blood (External respiration) and between the blood and bodily tissues (Internal respiration).
- Acid-Base Balance: The lungs are incredibly fast pH regulators. By altering the breathing rate, they control how much CO₂ is expelled. (High CO₂ in blood creates acid. Rapid breathing blows off CO₂, making blood more alkaline).
- Speech (Phonation): Air passing forcefully over the vocal cords produces sound for communication.
- Olfaction (Smell): Olfactory receptors in the superior nasal cavity detect airborne chemicals.
- Protection & Defense: The physical barrier, the mucociliary escalator, and alveolar macrophages actively protect the body from airborne pathogens and irritants.
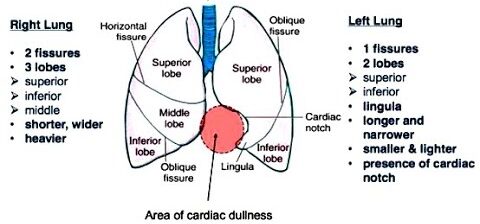
7. Anatomical Differences Between Right and Left Lungs
While both lungs perform identical gas exchange functions, they are distinctly asymmetrical, primarily molded by the position of the heart and massive blood vessels within the left side of the thoracic cavity.
| Anatomical Feature | Right Lung | Left Lung |
|---|---|---|
| Size & Weight | Significantly larger, wider, and heavier. (Because the liver pushes up on it from below, it is slightly shorter vertically). | Smaller, narrower, and lighter (to make room for the heart). |
| Lobes | 3 Lobes: Superior, Middle, and Inferior. | 2 Lobes: Superior and Inferior. |
| Fissures | 2 Fissures: Oblique Fissure (separates inferior from superior/middle) AND a Horizontal Fissure (separates superior from middle). | 1 Fissure: Oblique Fissure only. (No horizontal fissure). |
| Cardiac Notch | Absent. (Only bears minor impressions). | Prominent: A large, deep indentation on the anterior border of the superior lobe where the apex of the heart rests. |
| Lingula | Absent. | Present: A small, tongue-like projection of lung tissue extending from the inferior tip of the superior lobe, just below the cardiac notch. (Developmentally equivalent to the right middle lobe). |
| Main Bronchus | Shorter, wider, and steeper (more vertical). High risk for aspiration. | Longer, narrower, and more horizontal. (Forced horizontal because the massive aortic arch pushes down on it). |
| Hilum (Root) Arrangement | Bronchus is superior and posterior. The pulmonary artery is anterior. The Azygos vein arches over the top of the root. | The pulmonary artery is the most superior structure. The bronchus lies posterior and inferior. The Aortic Arch passes prominently over the top. |
8. Respiratory System Embryology & Development
The respiratory system begins its fascinating development early in embryonic life (around week 4) as a ventral outgrowth from the primitive foregut (which forms the digestive system). This shared origin explains why congenital fistulas (abnormal connections) between the trachea and esophagus are so common.
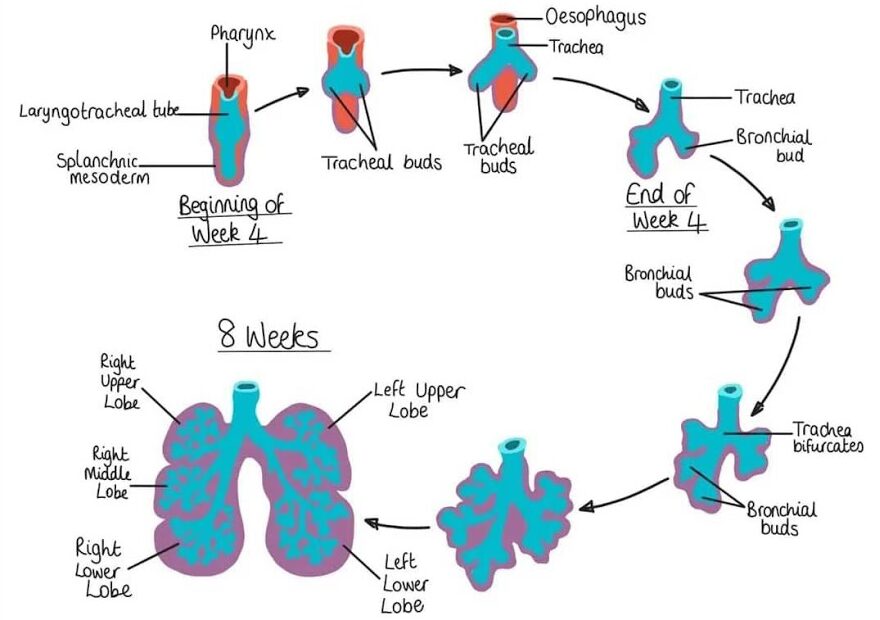
Formation of the Structures
- Laryngotracheal Diverticulum (Respiratory Bud): A groove forms in the ventral wall of the foregut, deepens, and pinches off outward. The tracheoesophageal septum fuses, physically separating the front tube (which becomes the trachea/lungs) from the back tube (which becomes the esophagus).
- Tissue Origins:
- Endoderm: The innermost embryonic layer forms the vital epithelial lining of the entire tract (larynx, trachea, bronchi, alveoli) and its glands.
- Splanchnic Mesenchyme: The surrounding middle layer forms all the supporting physical structures: cartilage rings, smooth muscle, connective tissue, and the dense pulmonary blood vessels.
- Branching Morphogenesis: Around week 5, the singular tube splits into two bronchial buds. These buds repeatedly branch, dividing over and over in a fractal pattern to form the entire complex bronchial tree down to the microscopic bronchioles.
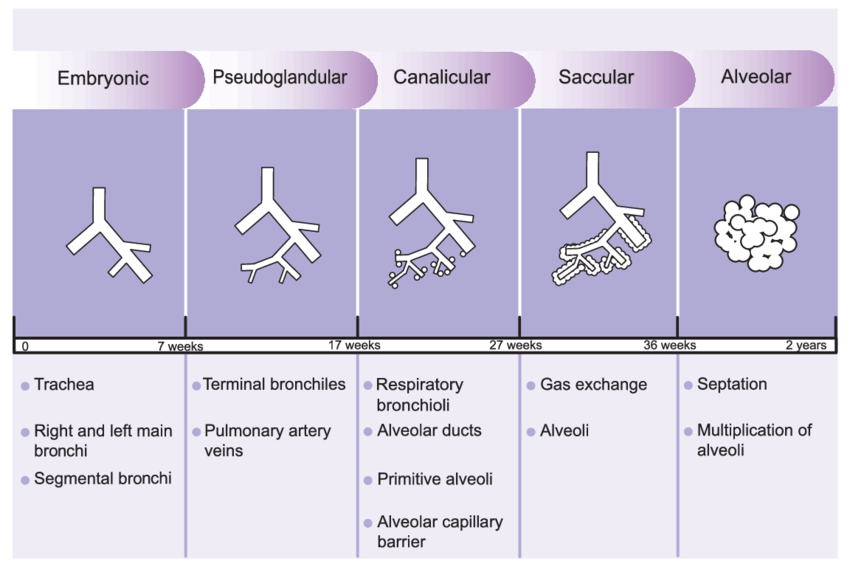
The Five Stages of Lung Maturation
The development from a simple tube into an organ capable of sustaining human life outside the womb is a prolonged, highly structured process.
The initial formation of the respiratory bud and its division into primary, secondary, and tertiary bronchi. The basic, gross architectural framework is established.
Extensive branching forms the terminal bronchioles. Under a microscope, the lung tissue at this stage looks remarkably like an exocrine gland (hence the name). Crucially, no alveoli exist yet, and vascularization is poor. A fetus born at this stage absolutely cannot survive, as gas exchange is impossible.
The terminal bronchioles divide into respiratory bronchioles, and the lung tissue becomes heavily vascularized (capillaries grow wildly). Primitive alveolar sacs begin to form at the end of this period. Survival becomes possible but extraordinarily difficult if born at the very end of this stage (around 24-26 weeks).
Alveolar ducts terminate in massive amounts of thin-walled terminal sacs. Type I pneumocytes thin out severely to prepare for gas exchange. Crucially, Type II pneumocytes mature and begin the massive production of Surfactant. Premature babies born before 28 weeks often lack this surfactant, suffering from lethal Neonatal Respiratory Distress Syndrome (NRDS) because their lungs collapse with every breath.
True, mature alveoli develop. A newborn infant has only about 50 million alveoli, representing just one-sixth of the adult number. Over the first 8 years of life, the lungs continue to grow via the massive multiplication of alveoli, eventually reaching the adult number of roughly 300 million.
9. Complications and Common Clinical Disorders
The respiratory system, being constantly exposed to the outside environment, is incredibly susceptible to a wide range of destructive disorders.
A. Obstructive Lung Diseases
These diseases are defined by an increased resistance to airflow. The patient can breathe in easily, but airways collapse or are blocked during exhalation, making it incredibly difficult to fully exhale the air. This traps old air in the lungs.
- Chronic Obstructive Pulmonary Disease (COPD): A progressive, irreversible disease encompassing two entities. Chronic Bronchitis features inflamed, narrow airways overflowing with excess mucus (chronic productive cough). Emphysema involves the destruction of alveolar walls and elastic tissue by protease enzymes (often triggered by smoking or a genetic Alpha-1 Antitrypsin deficiency), leading to massive, floppy lungs full of trapped air.
- Asthma: A chronic inflammatory disease characterized by hypersensitive, twitchy airways. Upon exposure to a trigger (allergen, cold air), immune mast cells dump leukotrienes and histamines, causing violent, reversible smooth muscle spasms (bronchoconstriction), swelling, and wheezing.
- Cystic Fibrosis (CF): A severe genetic disorder caused by a mutated CFTR chloride channel. The body produces incredibly thick, sticky, dehydrated mucus that totally clogs the airways, paralyzing the mucociliary escalator and leading to recurrent, deadly bacterial infections and permanent airway scarring (bronchiectasis).
B. Restrictive Lung Diseases
Characterized by reduced total lung volumes and decreased lung compliance (stiffness). The lung physically cannot expand fully, making it very difficult to take a deep breath in.
- Pulmonary Fibrosis: Severe scarring and thickening of the delicate alveolar interstitium, turning the spongy lung into stiff leather. It massively impairs oxygen diffusion. Can be idiopathic (unknown cause) or secondary to autoimmune diseases (like Rheumatoid Arthritis).
- Pneumoconiosis: A group of occupational lung diseases caused by the chronic inhalation of indestructible inorganic dusts. Examples include Asbestosis (asbestos fibers from old construction), Silicosis (sand/silica dust from mining), and Coal Worker's Pneumoconiosis (black lung). Macrophages try to eat the dust, die, and release chemicals that cause massive scarring.
- Chest Wall & Neuromuscular Disorders: Structural deformities like severe scoliosis, or paralyzing nerve diseases like ALS (Lou Gehrig's disease) and Muscular Dystrophy, which weaken the diaphragm and intercostal muscles until the patient can no longer pull air in.
C. Infections of the Respiratory System
- Pneumonia: Acute inflammation of the deep lung parenchyma usually caused by a bacterial (Streptococcus pneumoniae) or viral infection. The alveoli fill with pus, dead white blood cells, and fluid (exudate), essentially drowning the patient from the inside and completely shutting down gas exchange in the affected area.
- Tuberculosis (TB): A highly contagious, chronic bacterial infection caused by Mycobacterium tuberculosis. The bacteria evade immune destruction, forcing the body to wall them off inside hard, calcified nodules called caseating granulomas. This causes a chronic bloody cough, night sweats, and massive lung destruction over years.
D. Vascular and Pleural Disorders
- Pulmonary Embolism (PE): A sudden, life-threatening medical emergency where a massive blood clot (usually formed in the deep veins of the leg—DVT) breaks off, travels through the heart, and jams tightly into a pulmonary artery. It immediately blocks blood flow to a section of the lung, causing sudden, sharp chest pain, extreme shortness of breath, and potential sudden cardiac death.
- Pulmonary Hypertension: Chronically high blood pressure specifically isolated in the arteries of the lungs. The right side of the heart has to work incredibly hard to push blood against this pressure, eventually leading to right-sided heart failure (cor pulmonale).
- Pleural Effusion: An abnormal, massive accumulation of fluid in the pleural cavity. Can be a transudate (watery fluid pushed out by heart failure) or an exudate (protein-rich fluid leaked out by infections or lung cancer). It physically crushes the lung from the outside, preventing it from inflating.
10. Developmental Anomalies of the Respiratory System
Because the embryological formation of the lungs involves complex tubes splitting and merging, catastrophic errors can occur in the womb, leading to severe congenital birth defects.
- Tracheoesophageal Fistula (TEF) & Esophageal Atresia (EA): The most common severe anomaly. The septum fails to separate the airway from the gut properly. The esophagus ends in a blind pouch (EA), and the lower esophagus connects directly to the trachea (TEF). Clinical Presentation: The newborn swallows milk, it fills the blind pouch, and spills over into the lungs via the fistula, causing immediate choking, violent coughing, turning blue (cyanosis), and massive pneumonia on day one of life.
- Tracheal Stenosis / Atresia: A narrowing (stenosis) or complete absence (atresia) of a segment of the trachea. Atresia is uniformly fatal at birth without immediate, complex surgical intervention.
- Tracheomalacia: The cartilage rings of the trachea are severely underdeveloped and floppy. When the infant exhales or cries, the trachea collapses shut, creating a harsh, seal-like barking cough and stridor (high-pitched wheezing).
- Pulmonary Hypoplasia: Severe underdevelopment of the lung. It is incredibly small with vastly reduced alveoli. This almost always occurs secondarily to something compressing the fetal lungs in the womb, most famously a Congenital Diaphragmatic Hernia (CDH), where a hole in the diaphragm allows fetal intestines and the liver to push up into the chest cavity, physically crushing the growing lung.
- Congenital Pulmonary Airway Malformation (CPAM): A chaotic, disorganized mass of abnormal, cystic lung tissue that replaces normal alveoli. It does not exchange gas and can act as a space-occupying tumor, shifting the heart and crushing normal lung tissue.
- Bronchopulmonary Sequestration: A bizarre anomaly where a chunk of lung tissue develops completely disconnected from the normal bronchial airway tree. Furthermore, it steals its blood supply directly from a massive abnormal artery branching right off the descending aorta, bypassing the pulmonary circulation entirely. Often requires surgical removal due to recurrent chronic infections.
- Congenital Lobar Emphysema (CLE): An anomaly where cartilage in a specific lobe bronchus acts like a one-way flap valve. Air can enter the lobe when the baby inhales, but the flap closes when they exhale. The lobe becomes massively, dangerously over-inflated, trapping air and crushing the healthy lobes around it.
Summary of Developmental Anomalies of the Respiratory System
A. Anomalies of the Trachea and Bronchi
- Tracheoesophageal Fistula (TEF) & Esophageal Atresia (EA): An abnormal connection between the trachea and esophagus (TEF), often with the esophagus ending in a blind pouch (EA). Clinical Presentation: Neonates present with severe choking, coughing, and cyanosis during their first feed, and an inability to pass a nasogastric tube into the stomach.
- Tracheal Stenosis / Atresia: A narrowing (stenosis) or complete absence (atresia) of a segment of the trachea, leading to severe respiratory distress or stridor at birth.
- Tracheomalacia / Bronchomalacia: Severe weakness of the tracheal or bronchial cartilage, leading to airway collapse during exhalation. Causes a barking cough and stridor that worsens with crying.
- Bronchial Atresia: A blind-ending bronchus leading to an over-inflated, air-trapping segment of the lung distally.
B. Anomalies of the Lungs and Lung Development
- Pulmonary Agenesis / Aplasia / Hypoplasia: A spectrum ranging from complete absence of a lung (agenesis) to severe underdevelopment with reduced alveoli (hypoplasia). Hypoplasia is most commonly associated with conditions that physically restrict lung growth in the womb.
- Congenital Diaphragmatic Hernia (CDH): A defect in the diaphragm allowing abdominal organs (intestines/liver) to herniate up into the chest cavity, physically crushing the growing lungs and leading to severe pulmonary hypoplasia and lethal pulmonary hypertension at birth. A surgical emergency.
- Congenital Pulmonary Airway Malformation (CPAM): A non-cancerous, disorganized lesion of abnormal, cystic lung tissue that can compress healthy lung and cause respiratory distress in neonates.
- Bronchopulmonary Sequestration: A mass of non-functional lung tissue completely disconnected from the normal bronchial tree, which bizarrely receives its blood supply from a systemic artery (like the aorta) instead of the pulmonary circulation.
- Congenital Lobar Emphysema (CLE): Over-inflation of a single lung lobe due to a defective cartilage "check-valve" mechanism where air gets trapped on expiration. Causes progressive respiratory distress and shifts mediastinal structures.
References and Further Reading
- Standring, S. (2020). Gray's Anatomy: The Anatomical Basis of Clinical Practice (42nd ed.). Elsevier.
- Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2017). Clinically Oriented Anatomy (8th ed.). Lippincott Williams & Wilkins.
- Hall, J. E. (2015). Guyton and Hall Textbook of Medical Physiology (13th ed.). Saunders.
- Schoenwolf, S. C., Bleyl, S. B., Brauer, P. R., & Francis-West, P. H. (2014). Larsen's Human Embryology (5th ed.). Churchill Livingstone.
- West, J. B., & Luks, A. M. (2015). West's Respiratory Physiology: The Essentials (10th ed.). Wolters Kluwer.
- Kumar, V., Abbas, A. K., & Aster, J. C. (2020). Robbins & Cotran Pathologic Basis of Disease (10th ed.). Elsevier.