
Anatomy of the Thorax: The Rib Cage, Vertebrae, and Diaphragm
By the end of this highly detailed, exhaustive guide, you will master:
- The complete osteology and functional boundaries of the Thoracic Cage.
- The intricate anatomy of the Sternum and the vital topographical importance of the Sternal Angle.
- The structural classification, specific features, and comparative anatomy of the Ribs.
- The general and specific distinguishing features of the Thoracic Vertebrae.
- The precise neurovascular arrangement within a typical Intercostal Space.
- The boundaries, contents, and pathologies of the Thoracic Inlet and Thoracic Outlet.
- The muscular structure, vital apertures, and complex physiological actions of the Diaphragm.
1. The Rib Cage (Thoracic Cage)
The thoracic cage, commonly known as the rib cage, is a robust, dynamic bony-cartilaginous framework that forms the skeletal wall of the chest. Far from being a static structure, it is designed for continuous movement throughout a person's lifespan.
Critical Functions
- Protection: It entirely encapsulates and safeguards vital thoracic organs, including the heart, lungs, and great vessels (aorta, vena cava). Due to the dome shape of the diaphragm, the lower ribs also protect highly vascular upper abdominal organs, specifically the liver (on the right) and the spleen and kidneys (on the left and posteriorly).
- Muscle Attachment: It provides numerous, expansive points of attachment for muscles of the neck, back, chest, anterior abdominal wall, and upper limbs. This structural anchoring is heavily responsible for maintaining core posture and facilitating complex movements of the upper body.
- Respiration: Its flexible, expandable structure is fundamental to the mechanics of breathing. By elevating and expanding outward, it allows for massive changes in thoracic volume, creating the negative pressure necessary for inspiration.
- Support: It forms the central axial skeleton to which the pectoral girdle (clavicles and scapulae) and upper limbs are structurally attached.
Shape and Location
The rib cage is situated in the thorax, which is the region of the trunk directly between the neck and the abdomen.
- Its overall shape is that of a truncated cone. It is significantly wider inferiorly (at the base) than superiorly (at the neck).
- It is characteristically flattened anteriorly and posteriorly (dorsoventrally flattened), but prominently rounded laterally, creating a spacious cavity within to maximize lung expansion capacity.
2. Boundaries of the Thoracic Cage
The thoracic cage forms a well-defined, enclosed anatomical compartment with very distinct boundaries:
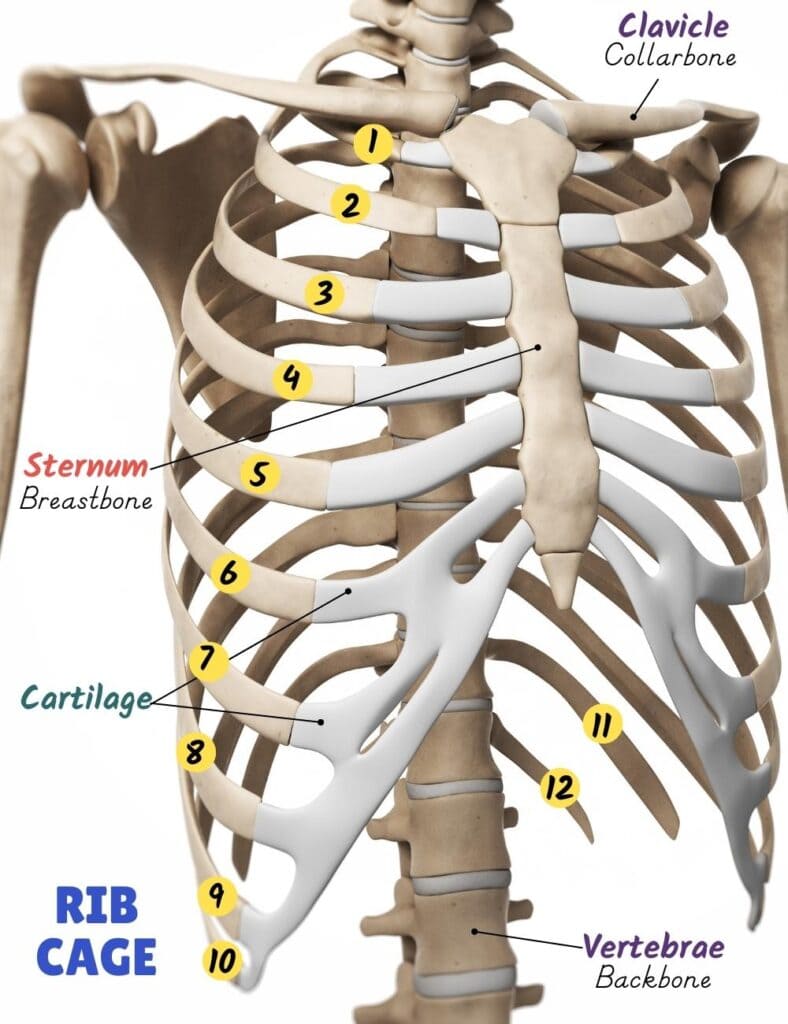
- Anterior Boundary: Formed centrally by the sternum (breastbone) and laterally by the articulating costal cartilages.
- Posterior Boundary: Formed by the twelve thoracic vertebrae (T1 through T12) and their resilient, shock-absorbing intervertebral discs.
- Lateral Boundaries: Consist of the twelve pairs of ribs, which arc expansively from the thoracic vertebrae posteriorly to the sternum or costal cartilages anteriorly.
Superior Boundary: Thoracic Inlet (Superior Thoracic Aperture)
This is a relatively small, kidney-shaped opening that acts as the physical gateway between the structures of the neck and the thoracic cavity.
- Formed by: The superior aspect of the first thoracic vertebra (T1) posteriorly, the medial borders of the first ribs laterally, and the superior border of the manubrium anteriorly.
- Passageway: This narrow aperture provides passage for dense, critical structures including the trachea, esophagus, major vessels (common carotid arteries, jugular veins, subclavian vessels), and vital nerves (vagus nerves, phrenic nerves, and the sympathetic trunk).
Inferior Boundary: Thoracic Outlet (Inferior Thoracic Aperture)
This is a much larger, highly irregular opening that forms the absolute floor of the skeletal thorax.
- Formed by: The 12th thoracic vertebra (T12) posteriorly, the 11th and 12th pairs of ribs laterally, and the costal margin (formed by the fused cartilages of ribs 7-10) and the xiphoid process anteriorly.
- The Seal: This aperture is almost completely sealed by the musculotendinous diaphragm, which definitively separates the thoracic cavity from the abdominal cavity.
3. The Sternum (Breastbone)
The sternum, or breastbone, is a flat, elongated bone positioned perfectly in the central anterior midline of the thoracic cage. It resembles a gladiator's sword and forms the anterior articulation point for the ribs via their costal cartilages.
Composition of the Sternum
The sternum is systematically divided into three fused parts:
The broadest, thickest, and most superior part of the sternum.
- Vertebral Level: Roughly lies opposite the T3 and T4 vertebral bodies.
- Superior Articulations: Features the deep suprasternal (jugular) notch at its superior border. Lateral to this notch are the clavicular notches for articulation with the clavicles, forming the highly mobile synovial sternoclavicular joints.
- Lateral Articulations: Possesses complete facets for articulation with the costal cartilages of the 1st pair of ribs, and demi-facets (half facets) for the upper half of the 2nd pair of ribs. These are synovial joints, permitting slight but essential movement.
- Inferior Articulation: Articulates with the body of the sternum at the manubriosternal joint.
The longest, central part of the sternum, resembling the blade of the sword.
- Superiorly: Articulates with the manubrium at the manubriosternal joint.
- Laterally: Contains scalloped facets for articulation with the costal cartilages of the lower half of the 2nd ribs, continuing all the way down through the 7th ribs.
- Inferiorly: Articulates with the xiphoid process at the xiphisternal joint.
The smallest, thinnest, and most inferior part of the sternum.
- Vertebral Level: The xiphisternal joint is typically exactly at the level of the T9 vertebral body.
- Characteristics: It is highly variable in shape and size (can be pointed, bifid, or perforated). It generally does not articulate with any ribs.
- Ossification: It remains purely cartilaginous in young individuals and gradually undergoes ossification (hardens into bone) starting from its proximal end. This process completes in adulthood and continues hardening into old age.
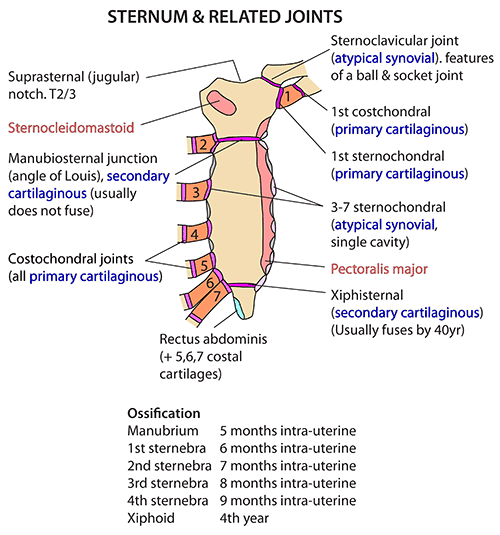
Joints of the Sternum
- Manubriosternal Joint (Sternal Angle / Angle of Louis): A secondary cartilaginous joint (symphysis) between the manubrium and the body. It forms a highly palpable transverse ridge on the chest.
- Xiphisternal Joint: A secondary cartilaginous joint between the sternal body and the xiphoid process. It typically fuses completely into a synostosis in older adults.
Clinical Uses and Pathologies of the Sternum
A. Diagnostic and Therapeutic Procedures
- Median Sternotomy (Median Thoracotomy): A major surgical incision made longitudinally straight down the center of the sternum. The bone is then physically divided using a specialized sternal saw.
Purpose: Provides massive, wide surgical access to the mediastinum (heart, great vessels, trachea, thymus) for critical procedures such as cardiac surgery (e.g., coronary artery bypass grafting, valve replacement) and lung transplantation. Post-surgery, the sternal halves are typically rejoined forcefully with thick stainless steel wires. - Bone Marrow Biopsy/Aspiration: Due to its broad, flat, and relatively superficial nature under the skin, the sternum (particularly the thick manubrium) is a highly common site for obtaining bone marrow samples. A specialized thick needle is bored into the sternal cancellous bone to extract marrow for diagnostic purposes.
Clinical Indication: Vital for diagnosing leukemia, severe anemias, or other hematological disorders. This site is chosen due to its easy accessibility, though great care is taken to avoid piercing entirely through the bone into the vital heart and aorta directly below.
B. Congenital Anomalies of the Sternum
Congenital malformations of the sternum primarily involve abnormalities in its physical shape, which can severely affect respiratory and cardiac function in extreme cases.
- Pectus Carinatum (Pigeon Chest): A chest wall deformity characterized by an outward protrusion of the sternum and adjacent costal cartilages. It gives the chest a prominent, "pigeon-breasted" appearance.
Clinical Significance: Usually cosmetic, but severe cases can physically restrict lung expansion and cardiac function, especially noticeable during strenuous exercise. - Pectus Excavatum (Funnel Chest): The absolute most common sternal deformity, characterized by an inward depression of the sternum and costal cartilages. It creates a "funnel-shaped" indentation in the chest. (Other descriptive terms include "Cup-shaped deformity" or "Saucer-shaped" deformity depending on the variant).
Clinical Significance: Ranges from mild cosmetic concerns to severe cases where the sunken sternum directly compresses the right ventricle of the heart and the lungs, leading to major respiratory and cardiac compromise (e.g., severely reduced exercise tolerance and arrhythmias). Often corrected via the Nuss Procedure. - Horns-of-Steer Deformity: An unusual and less commonly cited variant of chest wall deformity where the costal cartilages project aggressively laterally or superiorly, resembling the horns of a steer. This suggests distorted projections of the ribs or costal cartilages in relation to the sternum, often associated with other genetic connective tissue syndromes.
4. Anatomical Happenings at the Sternal Angle (Angle of Louis)
The sternal angle (Angle of Louis) is arguably the most crucial topographical anatomical landmark on the human chest due to the massive number of significant structures and events that occur exactly at its horizontal level. It is a palpable transverse ridge formed by the junction of the manubrium and the body of the sternum.
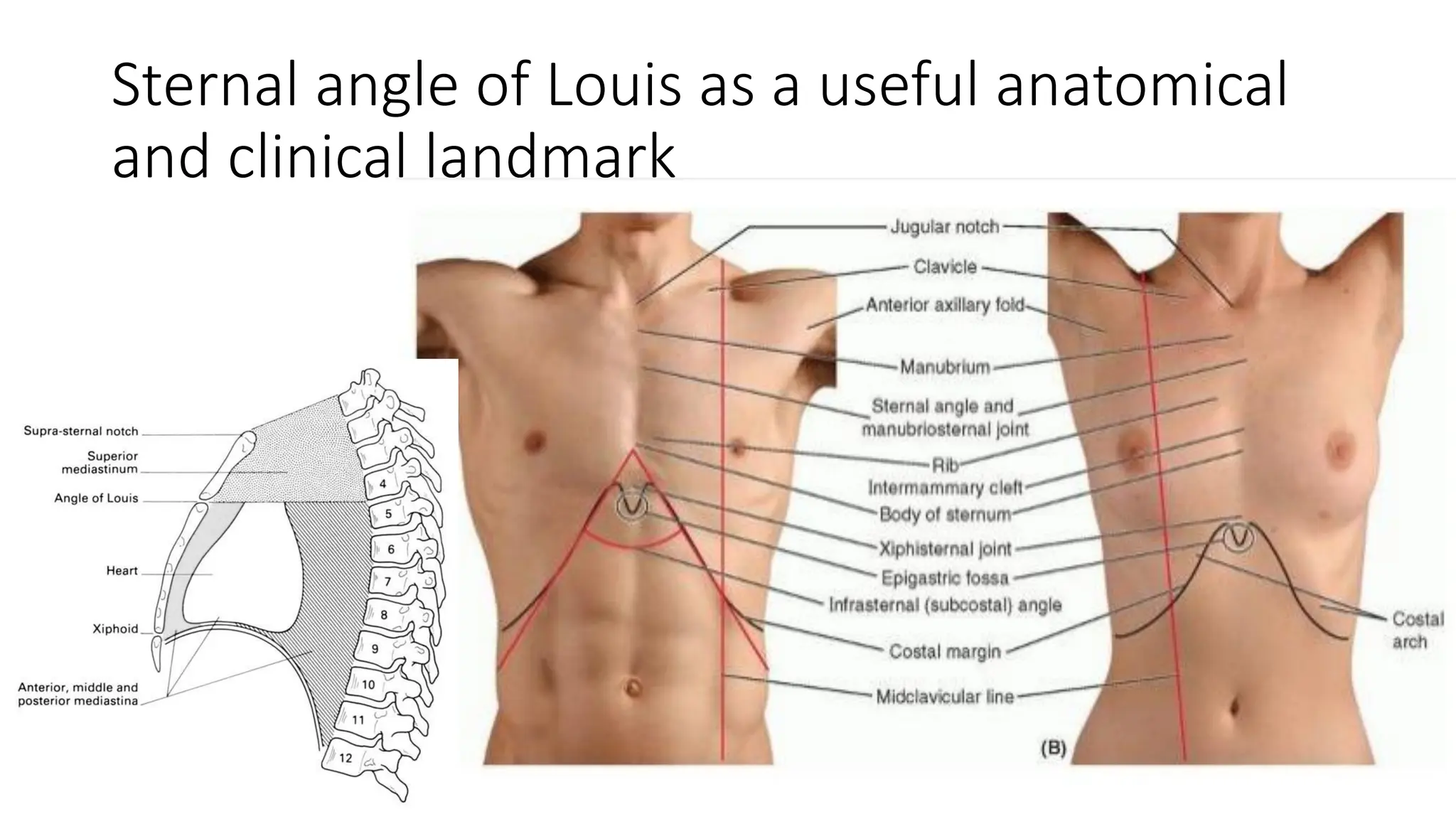
If an imaginary transverse plane is drawn straight backward from this angle to the spine, it dictates the following anatomical events:
- Skeletal Level: It marks the exact level of the intervertebral disc between the 4th and 5th thoracic vertebrae (T4/T5) posteriorly.
- Rib Articulation (The Counting Landmark): It is at the precise level where the costal cartilage of the second rib articulates with the sternum. Because the first rib is buried under the clavicle, this makes the second rib the easiest to identify clinically. From this point, physicians can confidently count other ribs and intercostal spaces down the chest (vital for placing ECG leads or chest tubes).
- Tracheal Bifurcation: It marks the level at which the trachea bifurcates (splits) into the right and left main bronchi at an internal ridge known as the carina.
- The Aortic Arch: It marks the anatomical beginning and end of the aortic arch:
- The ascending aorta ends (or becomes the aortic arch).
- The aortic arch begins and ends, giving rise to its three major branches.
- The descending aorta begins (at the inferior aspect of the T4 vertebra).
- Great Vessels and Connections:
- The ligamentum arteriosum, a fibrous remnant of the fetal ductus arteriosus, connects the arch of the aorta to the left pulmonary artery at this exact level.
- The azygos vein arches forward over the root of the right lung to drain into the superior vena cava (SVC) at or just above this level.
- The SVC itself enters the right atrium of the heart at this level.
- Nerve Relation: The left recurrent laryngeal nerve (a branch of the Vagus) loops under the inferior aspect of the arch of the aorta, just posterior to the ligamentum arteriosum, ascending back up to the larynx.
- Mediastinal Division: It serves as the arbitrary anatomical plane that divides the thoracic cavity into the Superior Mediastinum and the Inferior Mediastinum.
- Lymphatic Drainage: The main lymphatic drainage ducts (the massive thoracic duct and the smaller right lymphatic duct) may cross or terminate in the venous system in the direct vicinity of this level.
5. The Ribs: Structure and Function
The ribs are highly curved, flat, resilient bones that form the greater part of the thoracic cage. In healthy human anatomy, there are exactly 12 pairs of ribs.
Functions in Humans
- Respiration: The absolute primary function of the ribs, acting in concert with their associated intercostal muscles and flexible cartilage, is to facilitate respiration. Their bucket-handle and pump-handle mobility allows for the expansion and contraction of the thoracic cavity, essential for ventilation.
- Protection: The ribs provide profound, significant protection for the delicate vital organs within the thoracic cavity (heart, lungs, great vessels) and the superior abdominal organs (liver, spleen, kidneys). While high-velocity severe trauma can still damage these organs even with an intact rib cage, the bony matrix undoubtedly reduces their vulnerability to everyday blunt force.
- Muscle Attachment: They serve as crucial attachment points for numerous muscles of the chest (pectorals), back (latissimus dorsi, erector spinae), neck (scalenes), and upper limbs, playing major roles in movement, core posture, and forced respiration.
Comparative Anatomy (Non-Human Context)
To fully understand rib evolution and function, we briefly note comparative anatomy:
- Snakes: Ribs extend almost the entire length of their elongated trunk and are highly mobile, aiding fundamentally in locomotion. (Note on common misconception: The phrase sometimes used casually that ribs act as "inside feet" is anatomically incorrect for snakes, as they are inherently limbless; their ribs are purely part of their axial skeleton, though they are manipulated to grip the ground).
- Fish: Ribs primarily provide rigid attachment for massive swimming muscles and offer some protection against extreme external pressure (including immense hydrostatic pressure in deep-water marine species).
6. Classification of Ribs
There are 12 pairs of ribs in humans, intricately classified using two main overlapping systems:
A. Classification by Sternum Articulation
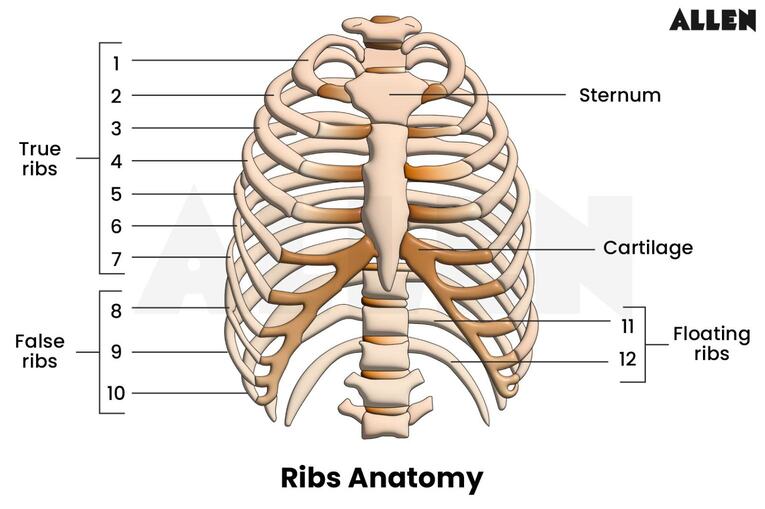
- True Ribs (Vertebrosternal Ribs) [Ribs 1-7]: Each true rib articulates directly with the sternum via its own dedicated, individual costal cartilage.
- False Ribs (Vertebrochondral Ribs) [Ribs 8-10]: These ribs do not directly articulate with the sternum. Instead, their costal cartilages attach to the costal cartilage of the rib immediately superior to them (typically the 7th costal cartilage acts as the anchor point), thereby indirectly articulating with the sternum. This fusion creates the palpable "costal margin" of the lower chest.
- Floating Ribs (Vertebral/Free Ribs)[Ribs 11-12]: These ribs have absolutely no anterior attachment to the sternum or to the cartilages of other ribs. Their cartilaginous tips end freely, floating in the posterior abdominal musculature.
B. Classification by Structural Features
Ribs are further classified by whether they share a standard anatomical blueprint or possess weird, unique features.
These share a common set of defining anatomical features:
- Head: The posterior, expanded end of the rib. It features two distinct articular facets (demifacets), separated by a bony crest. The inferior facet articulates with the superior costal facet on the body of its numerically corresponding vertebra. The superior facet articulates with the inferior costal facet on the body of the vertebra superior to it.
- Neck: The flattened, constricted portion extending laterally from the head.
- Tubercle: A bony prominence located at the junction of the neck and shaft. It has two parts:
- Articular part: A smooth facet that articulates with the transverse process of its numerically corresponding vertebra (forming a costotransverse joint).
- Non-articular part: A roughened elevation for the strong attachment of the costotransverse ligament.
- Angle: The point of greatest curvature of the rib, located just lateral to the tubercle. It also serves as an attachment point for the iliocostalis muscles.
- Shaft (Body): The main, elongated, curved part of the rib. It is smooth on its superior border and sharp on its inferior border.
- Costal Groove: Located along the inferior inner surface of the shaft. This crucial groove provides a protected pathway for the intercostal vein, artery, and nerve (V.A.N. – running from superior to inferior).
- Anterior End: Roughened and slightly hollowed to articulate firmly with the costal cartilage.
These possess unique features that distinguish them from typical ribs:
- First Rib (Rib 1): The shortest, broadest, and most sharply curved of all ribs.
Flattening: It is horizontally flattened, presenting superior and inferior surfaces (unlike other ribs which have medial and lateral surfaces).
Head: Has only ONE articular facet for articulation exclusively with the body of the T1 vertebra.
Features: Possesses a prominent Scalene Tubercle on its superior surface for the scalenus anterior muscle. Anterior to this tubercle is a shallow groove for the Subclavian Vein; posterior to it is a deeper groove for the Subclavian Artery and the lower trunk of the Brachial Plexus. - Second Rib (Rib 2): Longer and less curved than the first rib.
Head: Has two articular facets.
Feature: Displays a massive roughened Tuberosity for the Serratus Anterior on its outer lateral surface. - Tenth Rib (Rib 10): Similar to the first rib, its head usually has only ONE articular facet, articulating solely with the body of the T10 vertebra.
- Eleventh Rib (Rib 11): Head has only ONE articular facet (T11). No Neck. No Tubercle. (Does not articulate with transverse process). Costal groove is extremely shallow or absent.
- Twelfth Rib (Rib 12): Head has only ONE articular facet (T12). No Neck. No Tubercle. No Costal Groove. Often much shorter than the 11th rib.
Joints of the Ribs
The ribs form several critical articulations, permitting the massive flexibility required for respiration.
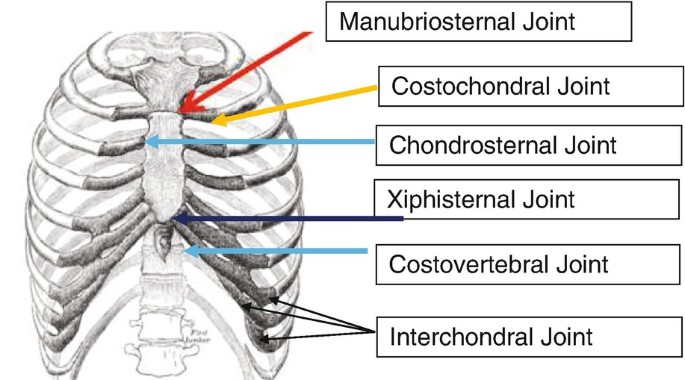
Costovertebral Joints (Posterior Articulations)
- A. Joints of the Heads of the Ribs (Synovial plane joints):
- Typical Ribs (2-9): Head articulates with two vertebral bodies and the intervening disc.
- Atypical Ribs (1, 10, 11, 12): Head articulates with only one vertebral body (its own number).
- Movement: Allow limited gliding movements for "pump-handle" and "bucket-handle" respiratory mechanics.
- B. Costotransverse Joints (Synovial plane joints):
- Articulations: Between the tubercle of the rib and the transverse process of its corresponding vertebra.
- Presence: Present for ribs 1-10. Ribs 11 and 12 completely lack tubercles and transverse process articulations.
Sternocostal Joints (Anterior Articulations)
- A. Costochondral Joints: Primary cartilaginous joints (synchondroses) between the rib bone and its costal cartilage. Zero movement is possible here.
- B. Chondrosternal (Sternocostal) Joints:
- 1st Rib: Forms a primary cartilaginous joint with the manubrium (immovable).
- Ribs 2-7: Form synovial plane joints with the sternum, allowing crucial gliding during heavy breathing.
- C. Interchondral Joints: Formed between the costal cartilages of ribs 8, 9, and 10. Mostly synovial plane joints.
Clinical Notes on Ribs and Thoracic Trauma
- Flail Chest: A catastrophic, life-threatening condition resulting from multiple rib fractures in two or more places on the same side, or sternum fractures combined with rib fractures. This physically detaches a segment of the chest wall.
Pathology: "Paradoxical Movement". During inspiration (negative pressure), the flail segment is sucked wildly inward. During expiration (positive pressure), it bulges outward. This wildly inefficient movement impairs ventilation and is almost always associated with severe underlying lung contusion. - Rib Grafts: Ribs are a premier source of autologous bone grafts (bone harvested from the patient's own body). Their curved shape and rich cancellous (spongy) bone content make them perfect for reconstructing defects.
Examples: Used extensively to replace the mandible (lower jawbone) following a mandibulectomy for cancer. Also used in complex facial reconstruction and spinal fusion surgeries. - Rib Contusion vs Deep Internal Injury: A rib contusion is a severe bone and muscle bruise caused by blunt trauma, resulting in extreme localized pain but no fracture.
Important Clinical Correction: If a medical report notes "small hemorrhage below peritoneum" following chest trauma, this is NOT a simple rib contusion. The peritoneum lines the abdominal cavity. Hemorrhage there strongly indicates that a fractured lower rib (e.g., Ribs 9-11) has physically pierced the diaphragm and lacerated an intra-abdominal organ (like the liver or spleen).
7. Vertebrae: General Features and Thoracic Specifics
The vertebrae are irregular bones forming the spinal column, providing structural support, encasing the spinal cord, and anchoring back muscles.
A. General Features of a Typical Vertebra
- Vertebral Body (Anterior): The massive, cylindrical anterior portion that bears the structural weight of the body.
- Vertebral Arch (Posterior): (Note to correct common anatomical misunderstandings: The body is ALWAYS anterior, and the arch is ALWAYS posterior). The arch is formed by two pedicles (struts attached to the body) and two laminae (flat plates meeting in the back).
- Processes (7 in total): Arising from the vertebral arch, serving as muscle anchors and joint surfaces:
- Spinous Process (1): Projects strictly posteriorly (the bumps you feel down your spine).
- Transverse Processes (2): Project laterally from the junction of the pedicle and lamina.
- Superior Articular Processes (2): Project upward with smooth facets to meet the vertebra above.
- Inferior Articular Processes (2): Project downward to meet the vertebra below.
- Vertebral Foramen: The large central opening. Stacked together, they form the vertebral canal housing the spinal cord.
B. Regions of the Vertebral Column (Total 33 Vertebrae)
Cervical (C1-C7), Thoracic (T1-T12), Lumbar (L1-L5), Sacral (S1-S5 fused), Coccygeal (Co1-Co4 fused).
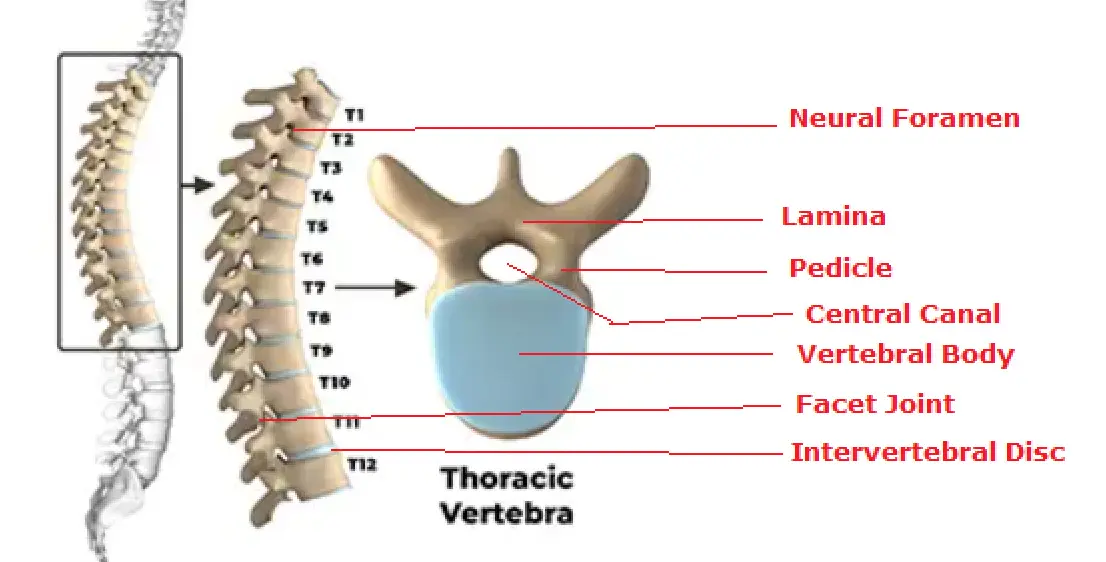
C. Distinctive Features of Thoracic Vertebrae (T1-T12)
Thoracic vertebrae are uniquely adapted to hold the rib cage.
- Vertebral Body: Characteristically heart-shaped when viewed from above.
- Vertebral Foramen: Generally smaller and distinctly circular.
- Spinous Process: Exceptionally long and slender. They slope sharply inferiorly (downwards), aggressively overlapping the vertebra below like roof tiles. This architectural design effectively limits potentially damaging hyperextension of the mid-back.
- Costal Facets on Bodies (The Defining Feature): ALL thoracic vertebrae have articular facets (or demifacets) on the lateral sides of their bodies for articulation with rib heads. Typical thoracic vertebrae (T2-T9) have two demifacets per side (superior and inferior). Atypical ones (T1, T10-T12) often have a single full facet.
- Costal Facets on Transverse Processes: T1-T10 possess articular facets on their transverse processes to hold the rib tubercles. T11 and T12 completely lack these.
8. Anatomy of a Typical Intercostal Space
An intercostal space is the anatomical gap between two adjacent ribs. The thorax contains 11 such spaces on each side. Each space is heavily defended by three muscular layers and contains a vital neurovascular bundle.
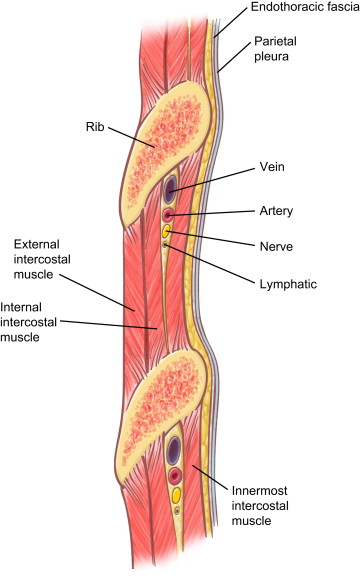
Muscle Layers of the Space
The space is filled by the External Intercostals (inspiration), Internal Intercostals (expiration), and Innermost Intercostals.
The Neurovascular Bundle (V.A.N)
This bundle runs along the inferior margin of the superior rib, deeply protected within the costal groove. It runs strictly between the Internal Intercostal and Innermost Intercostal muscle layers. The arrangement from superior to inferior is Vein, Artery, Nerve.
1. Intercostal Nerves
These are the massive ventral rami of the first eleven thoracic spinal nerves (T1-T11). The T12 nerve is unique and called the subcostal nerve.
- Type: Mixed nerves (carrying both motor signals to muscles and sensory signals from the skin).
- Branches:
- Motor Branches: Supply intercostal, subcostal, and transversus thoracis muscles.
- Collateral Branch: Runs along the superior border of the rib below to supply local periosteum and pleura.
- Lateral Cutaneous Branch: Pierces the side of the chest to supply sensation to the skin of the lateral thorax and abdomen. Divides into anterior and posterior branches.
- Anterior Cutaneous Branch (Terminal): Pierces the chest near the sternum to provide sensation to the front of the chest.
- Lower Nerves (T7-T12): These don't stop at the chest! They cross the costal margin and dive into the anterior abdominal wall, supplying the abdominal muscles (obliques, transversus abdominis) and skin down to the groin.
2. Intercostal Arteries
Each space receives massive collateral blood flow from two directions.
- Posterior Intercostal Arteries (11 pairs):
Spaces 1 & 2: Fed by the superior intercostal artery (a branch of the costocervical trunk from the subclavian artery).
Spaces 3-11: Fed directly by large branches off the descending Thoracic Aorta. (The 12th is the subcostal artery, also from the aorta). - Anterior Intercostal Arteries:
Spaces 1-6: Branch directly off the Internal Thoracic Artery (Internal Mammary Artery) running vertically behind the sternum.
Spaces 7-9: Branch from the musculophrenic artery.
Note: Spaces 10 and 11 completely lack an anterior arterial supply due to the absence of long cartilages.
3. Intercostal Veins
Venous drainage is highly complex and asymmetrical between the right and left sides of the body due to embryological development.
- Anterior Veins: Drain forward into the internal thoracic and musculophrenic veins, ultimately reaching the brachiocephalic veins.
- Posterior Veins (The Asymmetry):
- 1st Space: Drains straight up into the vertebral or brachiocephalic vein.
- Spaces 2-4 (Right): Unite to form the Right Superior Intercostal Vein, dumping into the Azygos Vein.
- Spaces 2-4 (Left): Unite to form the Left Superior Intercostal Vein, dumping into the Left Brachiocephalic Vein.
- Spaces 5-11 (Right): Dump directly into the main Azygos Vein.
- Spaces 5-8 (Left): Dump into the Accessory Hemiazygos Vein (which then crosses the spine to join the Azygos).
- Spaces 9-11 (Left): Dump into the Hemiazygos Vein (which also crosses to join the Azygos).
9. Thoracic Inlet and Thoracic Outlet Syndromes
The Suprapleural Membrane (Sibson's Fascia)
The Thoracic Inlet is roofed by a tough, dense fascial layer called the Suprapleural Membrane (Sibson's Fascia). It forms a fibrous tent over the apex of the lung.
- Attachments: Posteriorly to the transverse process of C7. Laterally to the inner medial border of the 1st rib. Anteriorly to the manubrium.
- Function: When you take a deep breath, negative pressure is created in the chest. Without this tough membrane, the suction would drag the delicate cervical pleura and lung apex violently up into the neck. It provides rigid structural integrity. The subclavian vessels and brachial plexus pass safely superior to (outside of) this membrane.
Thoracic Outlet Syndrome (TOS)
While anatomists call the top of the chest the "Inlet", clinicians refer to the anatomical space where nerves and vessels exit the neck and enter the arm as the "Thoracic Outlet". Compression here causes severe pathology.
- Location of Compression: The Scalene Triangle (between anterior and middle scalene muscles and the 1st rib), Costoclavicular Space (under the collarbone), or Pectoralis Minor Space.
- Causes: Congenital Cervical Rib (an extra rib growing from C7), anomalous fibrous tissue bands, massive muscle hypertrophy (in weightlifters), or clavicle fractures.
- Clinical Presentations:
- Neurogenic TOS: Crushing of the brachial plexus. Causes severe radiating pain, tingling (paresthesia), and muscle wasting in the hand.
- Arterial TOS: Crushing of the Subclavian Artery. The arm turns cold, pale, and suffers ischemic fatigue, especially when raised.
- Venous TOS (Paget-Schroetter syndrome): Crushing of the Subclavian Vein. The arm becomes massively swollen, heavy, and cyanotic (blue) due to blood pooling.
10. The Diaphragm
The diaphragm is a massive, dome-shaped musculofibrous septum serving as the definitive border between the thoracic and abdominal cavities. It is the absolute primary muscle of respiration. (Note: It is a characteristic feature of all mammals, including placentals, monotremes, and marsupials).
Structure and Anatomy
- Peripheral Muscular Part: Skeletal muscle fibers originating from the xiphoid process, the lower six ribs, and the lumbar vertebrae. They all sweep upward and inward.
- Central Tendon: A tough, aponeurotic, trilobate (trefoil shaped) sheet in the absolute center. It has no bony attachments; it is the target that the muscles pull upon.
- The Domes: It possesses a Right and Left dome. The Right dome is significantly higher than the left because the massive, solid Liver occupies the space directly beneath it, pushing it upward.
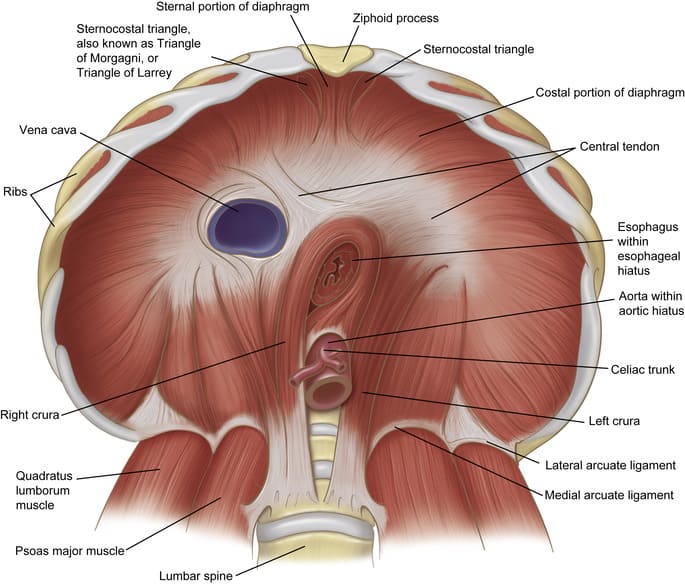
Major Diaphragmatic Apertures (Openings)
To maintain bodily function, the barrier must allow structures to pass through. There are three major hiatuses:
| Aperture | Vertebral Level | Anatomical Location | Critical Structures Passing Through |
|---|---|---|---|
| 1. Caval Opening | T8 | Strictly within the rigid Central Tendon. | Inferior Vena Cava (IVC) (Intimately fused to the margins to hold the vein open during breathing), Terminal branches of the Right Phrenic Nerve, Hepatic lymphatic vessels. |
| 2. Esophageal Hiatus | T10 | Within the muscular part, formed specifically by a sling of the Right Crus. | Esophagus, Vagus Nerves (Anterior & Posterior Trunks), Esophageal branches of the Left Gastric Artery/Vein. (The muscle acts as a physiological sphincter to prevent acid reflux). |
| 3. Aortic Hiatus | T12 | Technically posterior to the diaphragm, formed by the crura and the spine. | Aorta, Azygos Vein, Thoracic Duct. (Being strictly behind the diaphragm ensures the high-pressure aorta is not crushed every time the muscle contracts). |
Minor Openings: The Crura allow Splanchnic Nerves to pass. The Foramina of Morgagni (Larrey's spaces) anteriorly allow the Superior Epigastric vessels to pass. Sympathetic trunks pass behind the medial arcuate ligaments.
Actions of the Diaphragm
- Respiration (Inspiration): Contraction pulls the central tendon downward, flattening the domes. This dramatically increases thoracic vertical dimension, creating a vacuum that pulls air into the lungs. Relaxation causes passive exhalation.
- Increased Intra-abdominal Pressure: By contracting simultaneously with the abdominal wall, the diaphragm acts as a solid roof to build immense pressure in the abdomen. This is absolutely essential for Forced Expiration (sneezing/coughing), Defecation, Urination, Parturition (childbirth "pushing"), Vomiting, and stabilizing the trunk during heavy weight lifting (the Valsalva Maneuver).
- Thoracoabdominal Pump: The rhythmic up-and-down movement creates alternating pressure gradients that physically milk venous blood back to the heart and pump lymphatic fluid up the thoracic duct.
Nerve Supply: Exclusively innervated by the right and left Phrenic Nerves (Spinal roots C3, C4, C5). They supply motor function to the muscle and sensory input to the central tendon, pleura, and pericardium.
Clinical Correlates of the Diaphragm
- Congenital Diaphragmatic Hernia (CDH): A devastating birth defect where the diaphragm fails to close completely during embryogenesis (most commonly on the posterior left side, known as a Bochdalek hernia). Consequence: Intestines, stomach, and spleen protrude aggressively through the hole into the thoracic cavity. This physically crushes the developing fetal lung, leading to deadly Pulmonary Hypoplasia and respiratory failure at birth.
- Hiatal Hernia: Acquired stretching of the esophageal hiatus. A portion of the stomach bulges upward into the chest cavity, leading to severe acid reflux and chest pain.
- Traumatic Tear (Diaphragmatic Rupture): Sudden, extreme abdominal compression (e.g., steering wheel impact in a car crash) causes the diaphragm to burst. Abdominal organs violently herniate into the chest, crushing the lungs and strangulating the bowel.
- Diaphragmatic Paralysis: Caused by severing or crushing the Phrenic nerve (e.g., by a growing lung cancer).
Unilateral Paralysis: The patient may be asymptomatic at rest but struggles to breathe during exercise. Features "Paradoxical Movement": during inspiration, the healthy side pulls down, creating a vacuum that sucks the paralyzed side UP into the chest.
Bilateral Paralysis: A catastrophic event often caused by high cervical spine injury (above C3). The patient absolutely requires mechanical ventilation to survive.
List of References
The anatomical principles, definitions, classifications, and clinical correlations detailed in this comprehensive module guide are synthesized from universally accepted medical curricula and reflect the precise details outlined in standard literature. Primary references include:
- Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2018). Clinically Oriented Anatomy (8th ed.). Lippincott Williams & Wilkins.
- Standring, S. (Ed.). (2020). Gray's Anatomy: The Anatomical Basis of Clinical Practice (42nd ed.). Elsevier.
- Drake, R. L., Vogl, A. W., & Mitchell, A. W. M. (2019). Gray's Anatomy for Students (4th ed.). Elsevier.
- Snell, R. S. (2011). Clinical Anatomy by Regions (9th ed.). Lippincott Williams & Wilkins.
- Netter, F. H. (2019). Atlas of Human Anatomy (7th ed.). Elsevier.
- Tortora, G. J., & Derrickson, B. (2017). Principles of Anatomy and Physiology (15th ed.). Wiley.