
A route of administration is defined as the path by which a drug, fluid, poison, or other substance is brought into contact with the body. The parenteral route represents a crucial method of administration, bypassing the gastrointestinal tract to deliver medications safely and effectively.
To ensure patient safety and prevent medication errors, strictly adhere to these fundamental rights:
- Right Patient: Verify the patient's identity before administration.
- Right Drug: Ensure the correct medication is selected.
- Right Dose: Confirm the precise amount prescribed.
- Right Time: Administer at the correct interval.
- Right Route: Confirm parenteral administration is appropriate.
- Right Documentation: Accurately record the administration immediately after.
The chosen route significantly impacts the overall clinical outcome. The significance of selecting the correct route lies in determining the speed and efficacy of drug action, as well as its overall absorption and bioavailability. An optimal route ensures rapid action, minimal adverse reactions, better tolerability, and the rapid delivery of therapeutic concentrations of the drug directly to the desired site of action.
- Drug-related factors: Physical and chemical properties, pH, and irritancy.
- Patient-related factors: Age, underlying conditions, consciousness level, and compliance.
- Therapeutic action desired: Need for local vs. systemic effects, or immediate vs. sustained release.
- Systemic: Introduces the drug directly into the systemic circulation for wide distribution.
- Local: Exerts action locally at the site of application before disseminating into circulation.
| Enteral (enteron – of intestine) | Parenteral (par – beyond; enteron) |
|---|---|
| Extends from the mouth to the rectum. | Delivers medication across the body's defence barriers. |
| Simple, safe, and typically no sterilization required. | Ideal for emergencies. Provides higher bioavailability. |
| Slow onset of action; affected by digestive juices, enzymes, and First-Pass Metabolism (FPM). | Rapid action, No FPM, bypasses gastric irritation, suitable for irritant drugs. |
| Not ideal for irritants or severe emergencies. | Painful, invasive, requires strict asepsis and skilled personnel; higher risk for adverse events. Provides absolute control over the actual dose of drug delivered into the body. |
Proper preparation is vital. Ensure the following items are correctly arranged before initiating any injection procedure:
- Top shelf:
- Small Tray.
- Sterile syringes and needles of all capacities and appropriate sizes.
- Prescribed sterile medications in ampoules or vials.
- Patient’s charts and medicine lists.
- Gallipot with swabs.
- Antiseptic solution in a gallipot.
- Ampoule file.
- Sterile water for injection.
- Injection dishes.
- Bottom shelf:
- Tourniquet.
- Cannula of appropriate gauge.
- Strapping.
- Pair of scissors.
- Clean gloves.
- Sharps Safety Box.
- Receiver for used swabs.
- Receiver for used gloves.
- Small pillow for supporting the arm.
- Macintosh and towel.
- Screen for privacy.
- Handwashing equipment.
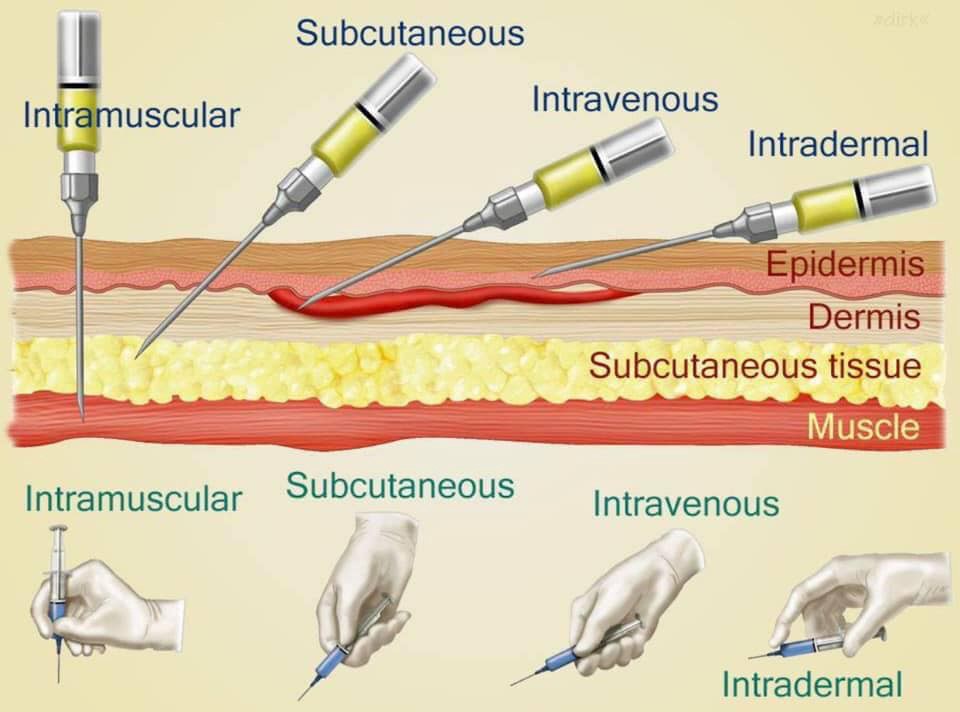
Intradermal injections are administered directly into the dermal layer of the skin. They are utilized for very small amounts of medication. The primary uses for this route include administering diagnostic tests (e.g., Mantoux test for tuberculosis, allergy testing) and the BCG vaccine.
| No. | Action | Rationale |
|---|---|---|
| 1 | Refer to general and medicine administration rules for injections. | Ensures adherence to foundational safety standards. |
| 2 | A tuberculin syringe or 1 ml syringe is used and needles. | Provides accurate measurement for minute volumes. |
| 3 | Identify the patient, put in a comfortable position. | Prevents errors and promotes patient cooperation. |
| 4 | Clean the skin with an antiseptic swab and allow the site to dry. | Exposes the selected site and minimizes infection risk. |
| 5 | If it is a BCG vaccination, clean the site with water. | Antiseptics may destroy the live attenuated BCG vaccine. |
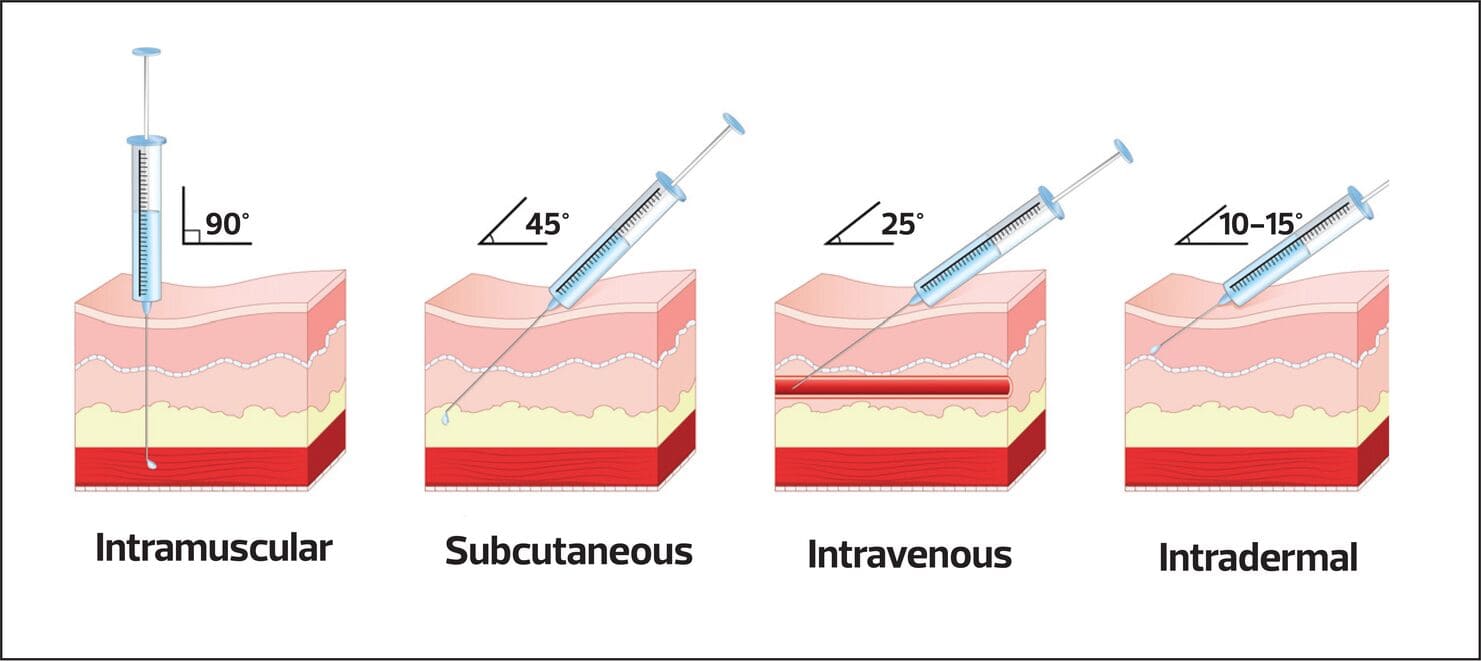
| 6 | Stretch the patient’s skin, draw it tight and introduce the needle at an angle parallel to the skin. | Facilitates entry specifically into the dermal layer. |
| 7 | Gently and slowly inject the medicine while observing for a small wheal to appear. | The wheal confirms correct placement within the dermis. |
| 8 | Carefully withdraw the needle. | Minimizes tissue trauma. |
| 9 | Do not massage the site after removing the needle. | This may alter the test results or disperse the medication prematurely. |
| 10 | Circle the area with a pen and record time, and request the patient not to wash the area until it is assessed for the intended outcome. | Necessary if it was for diagnostic purposes e.g., Mantoux test, to track the reaction area. |
| 11 | Inspect for signs of reaction when the stated duration of time has reached. | Allows for accurate interpretation of diagnostic tests. |
| 12 | Report and record results. | Maintains an accurate medical record and guides further treatment. |
| 13 | Clean away the used equipment. | Promotes environmental hygiene and safety. |
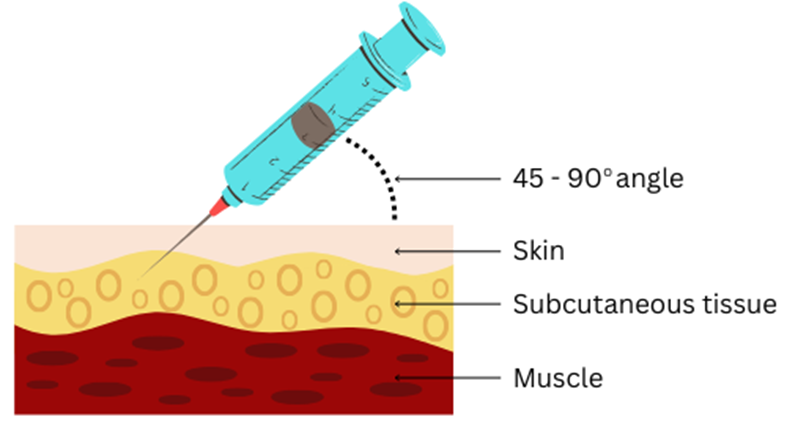
Subcutaneous (SC) injections deliver medication into the fatty tissue layer beneath the skin. This route allows for the sustained delivery of drugs. However, a notable disadvantage is the potential for local tissue bruising.
- Hypodermoclysis: Involves the continuous SC infusion of large amounts of fluids (500-1000ml). Historically used for infants and children, but it is rarely used nowadays.
- Insulin Pump: An external device that administers continuous or bolus insulin through a catheter inserted into the abdominal subcutaneous fat to help control blood sugar levels.
- Medi-Jector VISION: Currently FDA approved for insulin delivery, this uses pressure to create a micro-thin stream of insulin that penetrates the skin without a needle, depositing into the SC tissue in a fraction of a second.
- Biojector: Another needle-free device utilizing pressurized gas to drive medication through the skin into the SC tissue.
- PenJet: A new no-needle method of delivering SC drugs. It can deliver liquid or powdered drugs using compressed gas to force the drug through the skin. It is notably used to deliver the smallpox vaccine.
| No. | Action | Rationale |
|---|---|---|
| 14 | Help patient assume position depending on site selected. | Ensures free access to site. |
| 15 | Choose a suitable needle gauge; take a 1 ml or 2 ml syringe depending on the dosage. | Appropriate equipment prevents tissue damage and ensures accurate dosing. |
| 16 | Draw the medicine into the syringe. | Prepares the dose. |
| 17 | Expel the air by holding the syringe with the needle pointing up. | Prevents injection of air into the tissues. |
| 18 | Place the syringe in the injection dish. | Maintains sterility prior to injection. |
| 19 | Explain the procedure to the patient, asking him/her not to move while the injection is being given. | Encourages cooperation and allays anxiety. |
| 20 | Select the site and clean it with an antiseptic swab and let the area dry first. | Reduces microorganisms and prevents stinging from wet antiseptic. |
| 21 | Grasp and pinch or squeeze the patient’s skin gently between the finger and thumb of your left hand and insert the needle at an angle of 45°. | Provides for easy and less painful entry into subcutaneous tissue. |
| 22 | Pull back the (piston) plunger and inject the medicine slowly. | Determines if the needle is in a blood vessel. |
| 23 | When the medicine has been injected completely, place a swab over the needle and withdraw the needle quickly and smoothly. | Reduces discomfort. |
| 24 | If there is any bleeding at the site, apply firm gentle pressure with a swab until it stops. | Prevents hematoma formation. |
| 25 | Make the patient comfortable and record the medicine given on the patient’s treatment sheet. | Completes the documentation right of medication administration. |
| 26 | Discard syringe, gloves, and swabs appropriately and clear away the equipment. | Promotes infection control measures. |
Intramuscular injections deliver medication deep into the muscle tissue, which has a rich blood supply allowing for faster absorption than the SC route. Advantages include the ability to act as a solvent and minimizing leakage into surrounding tissues. Disadvantages may involve slower onset (compared to IV), potential for nerve damage, abscesses, and absorption fluctuations. The Z-track technique is highly recommended to prevent the medication from leaking back along the needle track into the subcutaneous tissue.
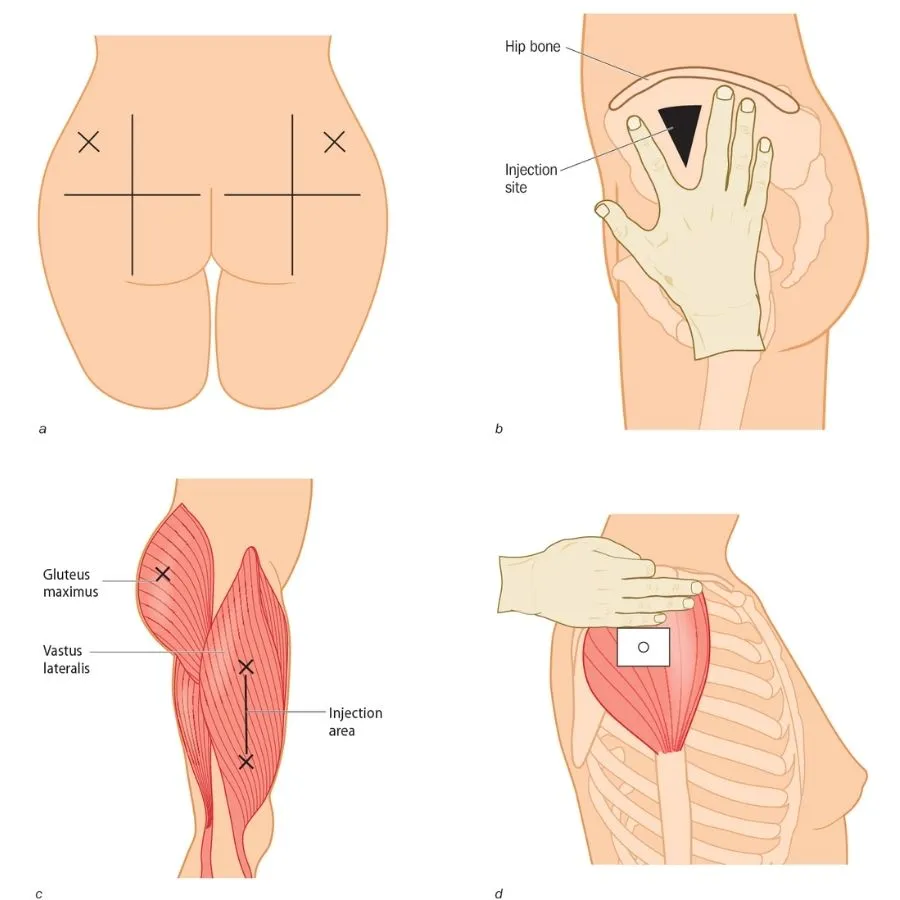
- Gluteal Muscle (Ventrogluteal & Dorsogluteal): The outer upper quadrant of the buttock (ventrogluteal) is considered the safest site, as it reliably avoids the sciatic nerve.
- Thigh Muscles (Rectus Femoris & Vastus Lateralis): The upper outer third of the thigh muscles provides an accessible and safe large muscle mass.
- Deltoid Muscle: Used for small injections (up to 2 ml) if the patient has enough muscle mass, but this site should be avoided whenever possible due to proximity to the radial nerve and brachial artery.
| No. | Action | Rationale |
|---|---|---|
| 27 | Observe the general nursing rules. | Ensures foundational standards of care. |
| 28 | Read the prescription carefully and check the medicine with the other nurse, including the amount to be given. | Double-checking minimizes the risk of medication errors. |
| 29 | Assemble syringe and needle, put on gloves. | Prepares for the procedure while maintaining personal protection. |
| 30 | Break open the top of the ampoule (by using a gauze swab or a file) or remove the top of the rubber cap. | Gains access to the medication while preventing injury from glass shards. |
| 31 | Reconstitute powdered medicines according to the instructions on the bottle. | Ensures the medication is in the correct administrable form. |
| 32 | Put on gloves and draw up the prescribed dose of the medicine. | Maintains sterility and secures the precise dosage. |
| 33 | Expel the air and remember that with antibiotics and multi-dose vials, the air is expelled into the container. | Ensures dosage accuracy and prevents positive pressure buildup in multi-dose vials. |
| 34 | Position the patient depending on the site chosen. | Proper positioning ensures muscle relaxation of the patient. |
| 35 | Select, locate, clean the site and allow it to dry. | Minimizes the introduction of pathogens into deep tissue. |
| 36 | Inject the medication; grasp and pinch the area surrounding the injection site or spread skin at site as appropriate. | Aids needle penetration in patients with thick muscles. |
| 37 | Hold the syringe between thumb and forefinger and pierce skin at a 90° angle and insert the needle. | Ensures the needle reaches the deep muscle layer. |
| 38 | Aspirate by holding the barrel steady with a non-dominant hand. | Helps to check if a needle is in a blood vessel. |
| 39 | If the blood does not appear in the syringe, inject the medication slowly and steadily. | Helps to disperse medication into muscle tissue, thus decreasing a patient’s discomfort. |
| 40 | Withdraw the needle slowly and steadily while supporting at the hub of the syringe and needle. With non-dominant hand support the skin surface using cotton swab for applying counter traction at the site. | Helps to reduce discomfort and prevent pulling of tissues when needle is withdrawn. |
| 41 | Apply gentle pressure at the site with a dry cotton swab but do not massage. | Massaging irritates tissues at the injection site. |
| 42 | Discard the un capped needle and syringe appropriately. | Promotes infection prevention and control. |
| 43 | Clear away, remove gloves and wash hands. | Prevents cross-contamination. |
| 44 | Record procedure including the name of medication, dose, site and response of the patient. | Reduces chances of medication errors. |
- Abscess Formation: Occurs when unsterile needles and syringes are used, or when oily substances are not injected deep enough. The injection site becomes inflamed and filled with pus.
Prevention: Strict adherence to aseptic technique, proper needle selection, and injecting oily substances deep into the muscle tissue. - Nerve Injury: Incorrectly positioning the needle can damage nearby nerves, causing pain, numbness, weakness, or paralysis.
Prevention: Thorough anatomical knowledge, correct landmark identification, and careful needle insertion. - Tissue Damage/Necrosis: Injecting too much medication, using irritating substances, or repeated injections in the same site can lead to tissue damage and cell death.
Prevention: Administering the correct dosage, choosing less irritating medications, and rotating injection sites regularly. - Hematoma: A hematoma forms when blood leaks into the surrounding tissue after the injection, causing a bruise or swelling.
Prevention: Applying pressure to the injection site after the injection. - Pain and Discomfort: Intramuscular injections can be painful, especially if the medication is irritating or the injection technique is not correct.
Prevention: Using proper injection technique, choosing a suitable needle size, and warming the medication to room temperature. - Allergic Reactions: Some individuals may have an allergic reaction to the medication or the ingredients in the solution.
Prevention: Thorough patient history, allergy testing, and careful observation. - Injection into a Blood Vessel: The needle may unintentionally enter a blood vessel, leading to potential complications like drug overdose or embolism.
Prevention: Aspirating (drawing back on the plunger) before injecting to ensure the needle is not intravascular. - Delayed-Onset Muscle Soreness: Medications can cause muscle soreness or stiffness appearing hours or days after injection.
Prevention: Staying hydrated and avoiding strenuous activity after the injection may help. - Infection: Improper sterile technique can lead to local infection.
Prevention: Strict adherence to aseptic technique. - Air Embolism: Rare, but air can be injected into the bloodstream, leading to respiratory distress or cardiac arrest.
Prevention: Proper technique to ensure no air is introduced into the syringe or needle.
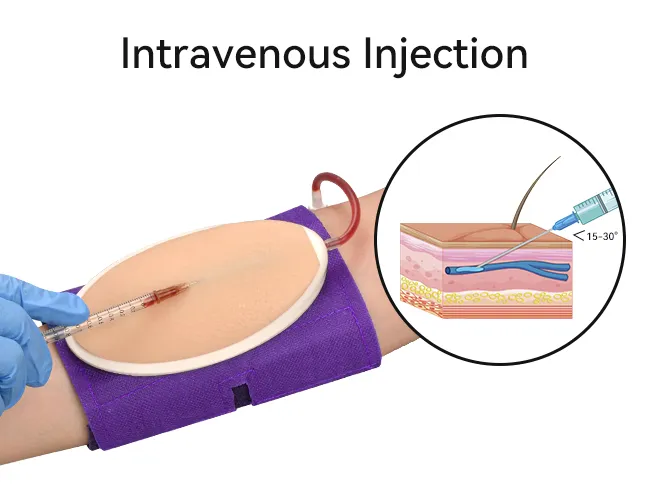
The Intravenous route is the most common parenteral route. It delivers drugs directly into the systemic circulation, providing 100% bioavailability. Types of IV administration include Bolus, Push, Slow injection, Infusion, and Central Venous Administration.
Disadvantages to consider: Susceptibility to severe Adverse Drug Reactions, requires strict asepsis, risk of inadvertent administration of wrong dose/drug, irritation leading to thrombophlebitis or cellulitis, potential injury to deeper structures, air embolism, necrosis, inability to administer suspensions or emulsions safely, and it strictly requires skilled personnel.
| No. | Action | Rationale |
|---|---|---|
| 45 | Prepare the injection tray and take it to the patient’s bedside. | Ensures all necessary items are available for the procedure. |
| 46 | Identify the patient and explain the procedure to the patient. | Alleys anxiety. |
| 47 | Screen the bed and put on gloves. | Provides privacy. |
| 48 | Place a small pillow and a protective sheet under the patient’s arm. | Promotes comfort and protects the beddings. |
| 49 | Expose the patient’s forearm and anterior surface of the elbow. | Ensures easy access to the injection site. |
| 50 | Inspect the selected vein, if it is visible and clear; apply a tourniquet or a sphygmomanometer cuff around the patient’s upper arm and inflate sufficiently about 8 to 10 cm above the site. | Helps to distend and enlarge the vein. |
| 51 | Request the patient to close and open the fist for a minute. | Promotes venous filling and visibility. |
| 52 | Clean the area with an antiseptic and dry with a sterile swab. | Reduces microorganisms. |
| 53 | Expel air from the syringe. | Ensures accurate dosing and prevents air embolism. |
| 54 | Hold the patient’s arm and with your left thumb exert pressure about 3 cm below the chosen site and make the skin tight. | Stabilizes the vein and reduces movement. |
| 55 | Insert the needle at an angle of 15-45 degrees with its bevel up then quickly and steadily insert into the vein. Pull back the piston slightly if blood is aspirated. | Ensures that the needle is in the vein. |
| 56 | Remove the tourniquet or deflate the cuff and inject the medicine slowly. | Prevents excessive pressure in the vein and ensures proper delivery of medication. |
| 57 | When the medicine is injected, put a swab over the site and withdraw the needle. | Minimizes bleeding and ensures cleanliness. |
| 58 | Apply pressure at the site with a swab for some seconds to make sure there is no bleeding. If oozing continues, apply a swab and a piece of strapping. | Prevents bleeding. |
| 59 | Record the medicine in the patient’s chart and clear away. | Ensures accurate medical records and maintains order. |
| Back of the Hand | Forearm | Lower Extremity |
|---|---|---|
Dorsal metacarpal veins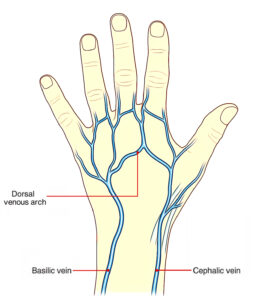 |
Basilic vein Cephalic vein 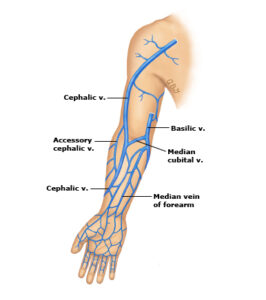 |
Dorsal venous plexus Medial and lateral marginal veins in the foot Femoral and saphenous vein in the thigh 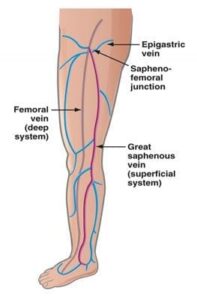 |
- Incorrect IV Site Placement: Inserting the IV into the wrong vessel (e.g., artery instead of vein) can lead to severe consequences.
- Medication Errors: Misidentification of medications, incorrect dosages, or incompatible mixing can result in serious adverse reactions.
- Rapid Administration and Undesired Effects: Delivering medications too quickly can lead to undesirable effects like hypotension, cardiac arrhythmias, allergic reactions, and fluid overload.
- Thrombophlebitis: Inflammation of a vein, often with a blood clot, due to frequent IV injections, improper technique, or certain medications.
- Circulatory Overload: Infusing too much fluid too quickly can overwhelm the circulatory system, leading to fluid buildup and strain on the heart and lungs.
- Embolism: A blood clot, air bubble, or foreign matter blocking a blood vessel can occur due to thrombophlebitis, improper placement, or air entering the line.
- Shock: Severe allergic reactions, blood loss, or sepsis can lead to a life-threatening decrease in blood flow to vital organs.
- Infiltration/Extravasation: When IV fluids leak out of the vein into the surrounding tissues, causing pain, swelling, and tissue damage.
- Phlebitis: Inflammation of a vein without a clot, often caused by irritation from the IV catheter or medication.
- Air Embolism: Air entering the bloodstream through the IV line can travel to the heart or lungs, causing blockage and leading to respiratory distress or cardiac arrest.
- Catheter-Related Bloodstream Infection (CRBSI): A serious complication where bacteria enter the bloodstream through the IV catheter, leading to fever, chills, and sepsis.
- Nerve Damage: Incorrect placement of the IV catheter can damage nerves in the area, resulting in pain, numbness, or weakness.
- Hematoma: Bleeding into the surrounding tissues from the IV puncture site, appearing as a bruise.
- Phlebosclerosis: Hardening of the vein due to repeated IV punctures or irritation from the catheter.
(Ordered Volume in mL × Drop Factor) / (Number of Hours × 60 minutes)

Example: If the doctor prescribes 1000 mls of 5% dextrose infusion to run over 10 hours, and the infusion set has a drop factor of 20, the calculation is: (1000 × 20) / (10 × 60) = 20000 / 600 = 33.3 drops per minute.
- Height of the Infusion Bottle: Raising the infusion bottle higher will increase the rate of flow, and lowering it will decrease the rate.
- Patency of Infusion Set and Needle: A blood clot in the needle may stop the infusion. This may occur when there is a delay in changing the emptied infusion bottle.
- Kinking of the Tubing or Faulty Position of the Needle: When the needle is against or away from the vein wall, it may affect the flow.
- Tight Splint: A tight splint on or above the infusion needle will restrict the flow rate.
- Blocked Air Vent: A blocked air vent will cause the infusion to stop running.
- Accurate Record Keeping: Keep an accurate record, including the time of starting the infusion, type of fluid, amount, and the prescribed rate of flow.
- Frequent Assessment: Assess the patient at frequent intervals for signs of abnormal reactions such as pain, sweating, restlessness, or change of color.
- Regular Site Inspection: Inspect the site at regular intervals for signs of infiltration.
- Condition Monitoring: Take and record the patient’s condition regularly.
- Daily Cleansing: If the infusion is running for some days, cleanse the area around the injection site with sterile gauze daily.
Administration proceeds directly into an artery via a catheter to specifically target the area being treated. This route requires specialized equipment such as intra-arterial ports. Because arteries possess high pressure, delivery usually requires an infusion pump or a pressure cuff.
Involves administering substances directly into the peritoneal space (the abdominal cavity). It is predominantly utilized for infusions such as peritoneal dialysis. This route is considered risky due to the potential for severe intra-abdominal infections and organ injury.
Fluid and medication administration is driven directly into the bone marrow space. The bone marrow presents a non-collapsible entry point, making it highly valuable in pediatric resuscitation and emergencies when intravenous access is impossible. Specialized devices like the EZ-IO are used.
Involves injecting medication directly into the ventricle of the heart. This extremely invasive route is utilized exclusively in life-threatening situations (such as cardiac arrest). The landmark for injection is typically the left 4th Intercostal space along the Midclavicular Line.
Medication is applied locally into the joint space, primarily for joint pain relief. Patients typically experience initial local discomfort before profound palliation of their symptoms occurs.
These routes introduce medications into the sheath surrounding the spinal cord, widely used for anaesthesia and specific antibiotics:
- Subarachnoid: Involves the instillation of a drug directly into the Cerebrospinal Fluid (CSF) after puncturing the dura and arachnoid membranes. There is free communication of the CSF in and out of the brain, making drug spread rapid. It is safely performed only in the lumbar spaces.
- Epidural: Medication is introduced into the potential space situated just above the dura mater. Because this space safely ends at the foramen magnum, injections can technically be performed across all spinal spaces. It is exceptionally well-suited for continuous nerve blocks.
- Combined Delivery Systems: Techniques such as the Combined Spinal Epidural or implanted Intrathecal Pain Pumps provide highly effective, sustained relief for severe, chronic pain conditions.
Drugs are administered directly into the respiratory tree. Formulations include aerosols, dry powders, nebulized solutions, and gases.
- Local Effect: Primarily for respiratory distress. Effectiveness is heavily dependent on particle size, optimally ranging between < 0.5μ and > 20μ.
- Systemic Effect: Used heavily in General Anaesthesia utilizing gaseous and volatile agents. Notable historical implementations include Exubera (an inhaled systemic insulin).
Aerosols or fluids are instilled directly into the nose. The massive vascular network in the nasal mucosa provides rapid absorption. However, repeated use can lead to mucosal dystrophy, and it is a common route of drug abuse. Modern devices enhancing delivery include Optinose and the Mucosal Atomization Device.
- Conjunctival: Administered to the eye using specialized delivery systems like Occuserts and Lacriserts.
- Otic: Applied into the ear canal.
- Vaginal: Includes solutions, emulsions, ointments, and pessaries.
- Urethral: Instilled directly into the urethra.
- Endotracheal: Critical emergency drugs can be administered via the endotracheal tube, commonly remembered by the drugs: Adrenaline, Atropine, Diazepam, and Naloxone.
Provides sustained delivery of drugs through the skin layer into the systemic circulation, lowering the risk of side effects by maintaining steady drug levels. The drug must be potent, otherwise, the required patch size becomes impractically large.
- Adhesive Patches: Rely on a drug reservoir continuously permeating a release membrane. Rate of absorption depends on the site, thickness/integrity of the stratum corneum, molecular size, membrane permeability, skin hydration, lipid solubility, and local blood flow.
- Iontophoresis: A non-invasive technique that employs a mild electric current to actively drive charged drugs through the skin.
- Phonophoresis: Relies on the movement of drug molecules through the skin forcefully driven under the influence of ultrasound waves.
Ultimately, no single route is ideal for all medications in all circumstances. Selecting the correct parenteral or non-parenteral route requires a comprehensive clinical assessment of the drug’s properties, the patient's status, and the precise therapeutic action required.
While the parenteral route bypasses the gastrointestinal tract and first-pass metabolism, each specific pathway presents unique clinical benefits and risks. Below is a summary of the most commonly utilized parenteral routes.
| Route | Advantages | Disadvantages |
|---|---|---|
| Intravenous (IV) |
|
|
| Intramuscular (IM) |
|
|
| Subcutaneous (SC) |
|
|
| Intradermal (ID) |
|
|
- Berman, A., Snyder, S. J., & Frandsen, G. (2020). Kozier & Erb's Fundamentals of Nursing: Concepts, Process, and Practice (11th ed.). Pearson.
- Potter, P. A., Perry, A. G., Stockert, P. A., & Hall, A. M. (2021). Fundamentals of Nursing (10th ed.). Elsevier.
- World Health Organization (WHO). (2010). WHO Best Practices for Injections and Related Procedures Toolkit. World Health Organization.
- Brunton, L. L., Hilal-Dandan, R., & Knollmann, B. C. (2017). Goodman & Gilman's: The Pharmacological Basis of Therapeutics (13th ed.). McGraw-Hill Education.
- Lynn, P. (2018). Taylor's Clinical Nursing Skills: A Nursing Process Approach (5th ed.). Wolters Kluwer.