
Inhalation is the breathing of air vapor or volatile medicine into the lungs.
- Dry inhalation: Oxygen Administration: this is given when the respiratory capacity is diminished as in chest injuries, pneumonia and cardiac failure.
- Moist/steam inhalation: It is used in case of inflammation of air passages and the nasal sinuses. These are given to:
- Warm and moisten the air breathed in and relieve irritation e.g. in bronchitis, after tracheotomy and other chest conditions.
- To relieve inflammation and coughing e.g. in colds.
- To relieve congestion and oedema e.g. in sinusitis and acute laryngitis.
- Nebuliser: this produces vapors which is inhaled by the patient for example in asthma to relieve spasms of the bronchial tubes or for the relief of chest pain in angina pectoris. Other indications include Respiratory diseases eg asthma, pneumonia, Airway obstruction, Nasal congestion, Nasal bleeding, Chest injuries and Cardiac failure.
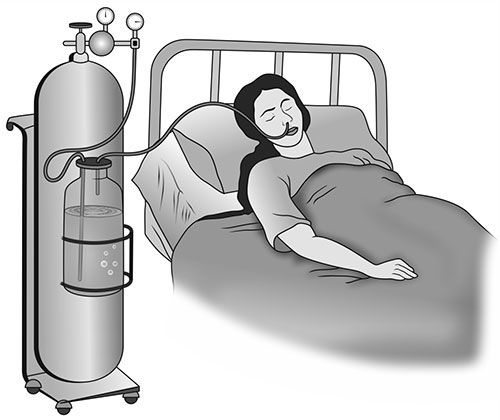
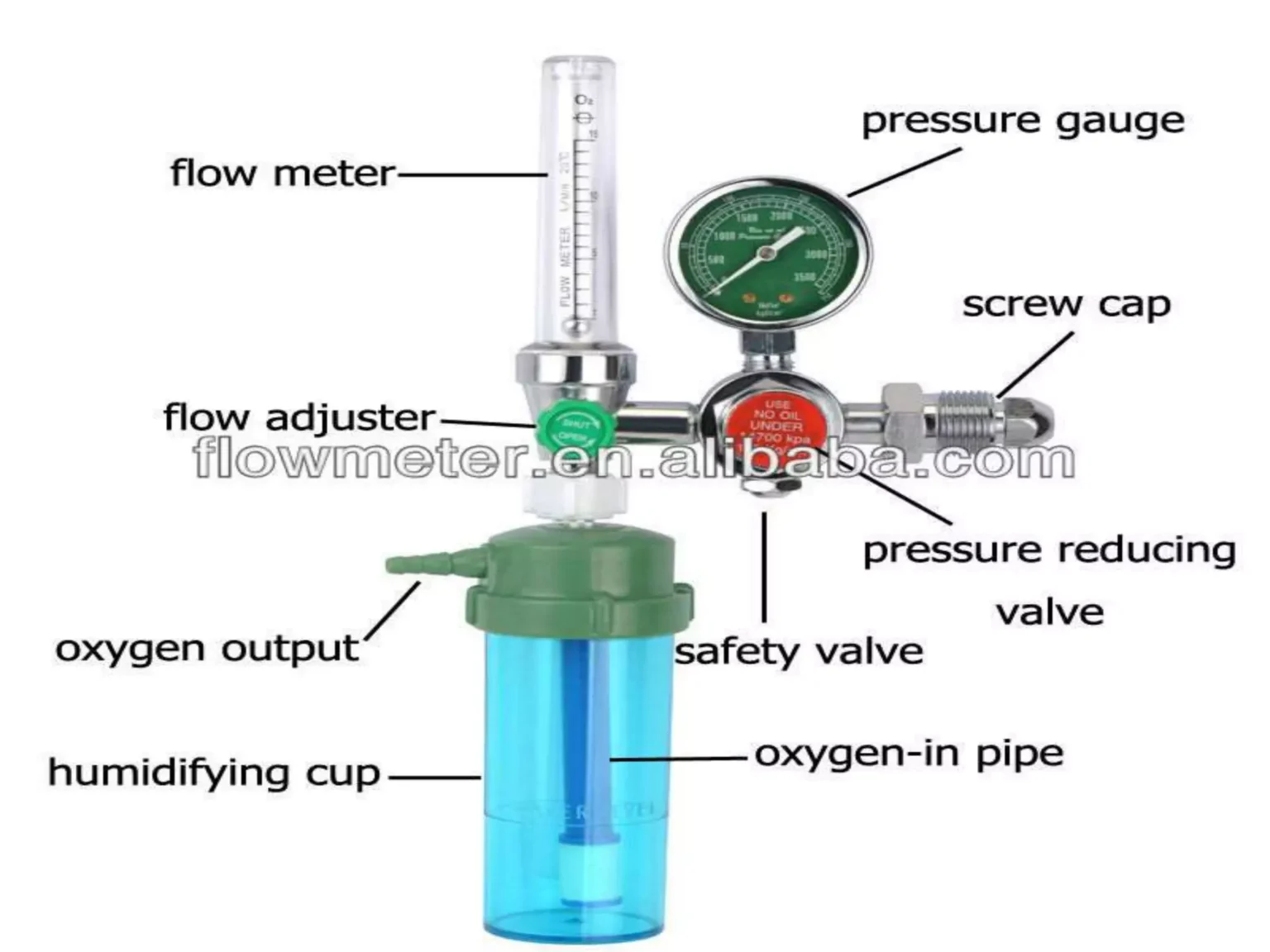
- Oxygen administration) Parts of an Oxygen Cylinder
Oxygen is a fundamental necessity for human survival, and in clinical settings, it is treated as a highly critical medication. The administration of oxygen must be carefully assessed, implemented, and monitored to ensure optimal patient outcomes while avoiding potential toxicity.
The concepts of oxygenation and oxygen inhalation form the foundation of respiratory therapy. The ambient room air we breathe contains about 21% oxygen. When a patient's condition compromises their ability to extract or utilize this baseline oxygen, supplemental therapy becomes necessary.
Oxygenation refers to the addition of oxygen to any system, including the human body. In clinical practice, oxygenation may also refer to the active process of treating a patient with supplemental oxygen, or combining a medication or other substances with oxygen (such as in nebulization).
Oxygen Inhalation is the specific clinical method of supplying a higher concentration of oxygen than what is naturally found in the surrounding environmental atmosphere. This is achieved through various specialized delivery devices.
- Oxygen is administered whenever there is a documented deficiency in the blood, often visibly manifested by cyanosis (bluish discoloration of the skin and mucous membranes).
- Normal Parameters: Normal oxygen concentration (saturation) in the blood should ideally be maintained at more than 90% to 95% depending on the patient's baseline health and underlying conditions.
- To Supply Oxygen: To provide adequate supplemental oxygen in conditions where there is significant interference with the normal oxygenation of blood (e.g., alveolar-capillary blockages, hypoventilation).
- To Reduce Respiratory Distress: Supplemental oxygen decreases the work of breathing, alleviating the physical effort and distress experienced by the patient.
- To Reduce Effects of Anoxemia: By increasing the oxygen tension in the alveoli and blood, it mitigates the systemic cellular damage caused by profound anoxemia (lack of oxygen in arterial blood).
Oxygen therapy is indicated in a wide variety of acute and chronic clinical scenarios. Key indications include:
- Breathlessness (Dyspnea): Subjective feeling of difficult or labored breathing.
- Obstructed Airway: Blockages due to physical growths, tumors, or anatomical swellings like an enlarged thyroid gland (goiter).
- Cyanosis: A late sign of severe hypoxemia requiring immediate intervention.
- Cardiac Failure: The heart's inability to pump effectively leads to poor systemic perfusion and secondary tissue hypoxia.
- Respiratory Distress: From conditions like asthma, COPD exacerbations, pneumonia, or acute respiratory distress syndrome (ARDS).
- Shock: Hypovolemic, cardiogenic, or septic shock states where cellular oxygen demand outpaces systemic supply.
- After Severe Hemorrhage: Significant blood loss reduces the hemoglobin available to carry oxygen, necessitating supplemental O2 to saturate the remaining hemoglobin fully.
- Anemia: Severe reduction in red blood cells impairs oxygen transport capacity.
- Patient under Anesthesia: To maintain adequate oxygenation when respiratory drive is chemically suppressed.
- Asphyxia: Severe deprivation of oxygen to the body that arises from abnormal breathing (e.g., choking, drowning).
- Poisoning: Specifically, carbon monoxide (CO) poisoning, where high-flow oxygen is required to displace CO from hemoglobin.
- Post-Operative Period: To support recovery as patients emerge from anesthesia and metabolize medications.
- Insufficient O2 in the Atmosphere: High altitudes or confined spaces with poor ventilation.
Hypoxia is defined as a decreased oxygen concentration in the blood and at the cellular/tissue level. It is a critical state that, if left untreated, rapidly leads to cellular dysfunction and tissue death.
Clinical manifestations of hypoxia can be divided into early and late signs. It is crucial for nurses to recognize these signs promptly:
- Restlessness and Anxiety: Often the earliest indicators of hypoxia as the brain becomes mildly oxygen-deprived.
- Decreased Level of Consciousness: Confusion, lethargy, or coma can develop as hypoxia worsens.
- Lack of Concentration: Cognitive impairment and dizziness.
- Increased Fatigue: Extreme tiredness as cellular energy production shifts to less efficient anaerobic pathways.
- Tachypnea: Increased rate and depth of respiration as the body attempts to draw in more oxygen.
- Tachycardia and Elevated BP: An increased pulse rate and elevated blood pressure occur initially as a compensatory sympathetic nervous system response.
- Pallor: Paleness of the skin due to peripheral vasoconstriction.
- Cyanosis: A late and critical sign. It is a bluish discoloration of the skin, nail beds, and mucous membranes indicating high levels of deoxygenated hemoglobin.
- Dyspnea: Subjective feeling of shortness of breath.
- Clubbing of the Nails: A chronic sign of long-term hypoxia. The normal angle of the nail bed becomes distorted and enlarged (greater than 180 degrees), often seen in chronic respiratory or cardiac diseases.
- Wall Outlet: Centralized piped oxygen supply commonly found in hospital wards, intensive care units, and emergency departments. It provides a continuous, high-pressure source.
- Portable Cylinder: Oxygen compressed into metal tanks of various sizes. Essential for patient transport, home care, or as emergency backups during power or central system failures.
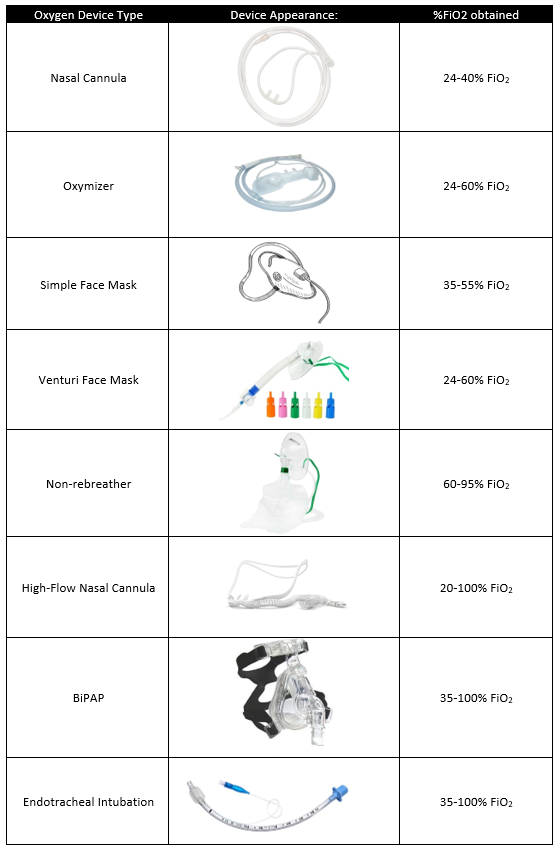
Oxygen delivery devices are broadly categorized by the concentration (FiO2) they can deliver. Selecting the right device depends on the patient's precise clinical requirements.
The nasal cannula consists of a thin, flexible tube with two small nozzles (prongs) that protrude directly into the patient's nostrils.
- Flow Rate & Concentration: Used to administer 2 to 6 Liters per minute (L/min), delivering an oxygen concentration (FiO2) of approximately 24% to 45%.
- Setup: Connected to an oxygen source equipped with a flow meter and a humidifier.
- Advantages: It is lightweight, comfortable, and allows the patient to carry out daily activities such as eating, drinking, and speaking without removing the device.
- Disadvantages: Easily dislodged during sleep or movement. It can cause drying and irritation of the nasal mucosa, making humidification vital at higher flow rates (>4 L/min).
Face masks fit over the patient's nose and mouth. There are four primary types utilized in clinical practice:
- Simple Face Mask:
- Application: Applicable for providing moderate oxygen therapy. Contains exhalation ports on the sides to allow exhaled CO2 to escape.
- Flow Rate & Concentration: 5 to 8 L/min delivering an oxygen concentration between 40% to 60%.
- Precaution: Flow rates must be at least 5 L/min to flush exhaled carbon dioxide out of the mask and prevent rebreathing.
- Partial Rebreather Mask:
- Application: A simple face mask equipped with a reservoir bag attached to the base.
- Mechanism: The reservoir bag collects the patient's exhaled air. The patient rebreathes the first 1/3rd of the expired air from the bag (which is rich in oxygen and from the anatomical dead space), mixing it with 100% source oxygen. This permits excellent oxygen conservation.
- Flow Rate & Concentration: 6 to 10 L/min delivering 60% to 90% oxygen concentration.
- Precaution: The reservoir bag must remain totally or partially inflated during inspiration. If it deflates completely, carbon dioxide buildup can occur.
- Non-Rebreather Mask:
- Application: Similar in appearance to a partial rebreather but features specific one-way valves.
- Mechanism: Two one-way valves prevent the patient from rebreathing the exhaled air; exhaled air escapes through the side ports. A valve between the mask and the bag prevents exhaled air from entering the oxygen reservoir.
- Flow Rate & Concentration: 10 to 15 L/min, designed to deliver the highest concentration of non-invasive oxygen, ranging from 95% to 100%.
- Venturi Mask:
- Application: A high-flow system designed to deliver a precise, predetermined oxygen concentration.
- Mechanism: It utilizes wide-bore tubing and color-coded adapters (jets) based on the Bernoulli principle. It provides accurate control of oxygen such that it does not rise too high (which could cause respiratory depression in certain COPD patients) but remains adequate to relieve anoxia.
- Flow Rate & Concentration: Delivers varying, exact concentrations from 24% to 60% at flow rates of 4 to 15 L/min depending on the adapter used.
- Color-Coded Adapters (Common Standard):
- Blue: 24% at 2 L/min
- White: 28% at 4 L/min
- Orange: 31% at 6 L/min
- Yellow: 35% at 8 L/min
- Red: 40% at 10 L/min
- Green: 60% at 15 L/min
- Oxygen Tent: A thin, clear plastic tent-like structure suspended over the patient. The sides are tucked firmly under the bed clothing of the patient to maintain the oxygen-rich environment. Usually used for delivering oxygen to infants and toddlers who will not tolerate masks or cannulas.
- Oxygen Hood / Head Box: Used for neonates and young infants. It is a clear plastic device kept entirely over the head of the baby. It helps in the highly efficient, controlled delivery of oxygen and humidity. Precaution: While placing the hood over the head of the child, ensure the rigid plastic edges do not rub against the child's chin, neck, or shoulder, which could cause skin breakdown.
- O2 cylinder with flow meter connected, or wall outlet access.
- Regulator gauge (if using a cylinder).
- Humidifier bottle filled with sterile distilled water.
- Cardex / Patient chart (to verify the physician's order).
- Cylinder with stand (for stability and safety).
- Opening key / wrench (for cylinder valves).
- Delivery device: Nasal cannula or O2 mask with connective tubing.
- Gauze pad / cotton balls (for cleaning nares/face).
- A bowl with plain water (to check O2 patency/flow visually if needed).
- Delivery devices: Nasal cannula, Nasal catheter, BLB oxygen mask, or simple face mask with connective tubes.
- Rubber tubing.
- Flowmeter and regulator gauge.
- Humidifier with sterile distilled water.
- Gallipot with gauze pads or cotton balls.
- A bowl with plain water (to check O2 patency/flow).
- Oxygen source (Wall outlet or portable Oxygen cylinder with stand).
- Opening key / wrench (for cylinder valves).
- Screen (for privacy).
- Cardex / Patient chart.
| Steps | Action | Rationale |
|---|---|---|
| 1 | Refer to the general rules. | Keeps standard practice and ensures safety guidelines are followed. |
| 2 | Determine the need for oxygen therapy in the patient and verify the physician’s order / prescription in the Cardex for rate, device used, and concentration. | Reduces risk of error in administration and ensures the right treatment is given to the right patient. |
| 3 | Explain the procedure to the patient and inform them how to co-operate. | Alleviates patient anxiety, gains compliance, and promotes safety. |
| 4 | Wash hands. | Standard infection control measure to prevent the transmission of microorganisms. |
| 5 | Turn and test the oxygen cylinder/source before bringing everything to the bedside. Check the condition of the oxygen pipe and flow meter. | Conserves time and energy by confirming functional supply before patient application. |
| 6 | Provide privacy using a screen and position the patient in a sitting up, semi-Fowler's, or on one side position if possible. | Promotes comfort. Elevating the head of the bed drops the diaphragm, allowing for maximum chest expansion and improved lung ventilation. |
| 7 | Clean the nostrils with a swab stick if the nostrils are blocked with secretions. | Ensures a patent airway. Blocked nares will prevent oxygen from reaching the lower respiratory tract. |
| 8 | Set up O2 equipment and humidifier. Attach rubber tubing, nasal cannula/catheter, or mask to the humidifier. | Ensures all components are securely connected to prevent leaks and ensure adequate delivery to the patient. |
| 9 | For nasal cannula use: Connect nasal cannulae to oxygen set up with humidification, check if oxygen is flowing out of prongs (can use the bowl of water to check flow). Regulate flow meter to prescribed level. | Humidification prevents dehydration of mucous membranes. Checking flow ensures the exact prescribed dosage is flowing through the system. |
| 10 | Place prongs in the patient’s nostrils 2 inches, place tubing over and behind each ear with adjuster comfortably under the chin OR place tubing around the patient’s head with the adjuster at the back or base of the head. Place gauze pads at the ear beneath the tubing as necessary. | Facilitates oxygen administration and patient comfort. Pads reduce irritation and prevent severe pressure ulcers from constant tubing pressure. |
| 11 | Encourage the patient to breathe through the nose, with the mouth closed. | Nose breathing provides for optimal delivery of oxygen to the patient. |
| 12 | For B.L.B mask / Reservoir mask use: Attach face mask to oxygen source, start the flow of oxygen at the specified rate. For a mask with a reservoir, allow oxygen to fill the bag before proceeding to the next step. | The bag is the primary oxygen supplier to the patient; it must be inflated to prevent carbon dioxide buildup. |
| 13 | Position the face mask over the patient’s nose and mouth, adjust the elastic strap around the patient’s head, and adjust the flow rate to avoid air leakage from the edges. | A loose or poorly fitting mask will result in oxygen loss and sub-therapeutic oxygen delivery. |
| 14 | Apply padding behind ears as well as the scalp where the elastic band passes. | Padding prevents skin irritation and breakdown from tight elastic bands. |
| 15 | Reassess patient’s respiratory status, including respiratory rate, effort, and lung sounds. Observe for oxygen saturation hourly (must be more than 90%). | Assesses the effectiveness of oxygen therapy and dictates if further clinical adjustments are needed. |
| 16 | Check for proper flow rate every four hours. Ensure that ports of the mask are open. | Flow meters can be accidentally altered. Open ports prevent CO2 rebreathing and suffocation. |
| 17 | Assess the client's face, ears, and nostrils every 8 hours. Sterile water-soluble lubricants can be used to keep the mucous membrane moist. | Oxygen is highly drying; frequent assessment and lubrication prevent mucosal damage and skin integrity issues. |
| 18 | Wash hands upon completion of patient contact. | Maintains strict infection control protocols. |
| 19 | Document relevant information in the patient’s record including time, flow rate, and observations made on the patient. Record any abnormal findings, outcomes, and SpO2 results, and report abnormalities. | Ensures accurate medical records. Prompt reporting ensures rapid medical intervention if the patient deteriorates. |
Oxygen therapy carries inherent risks, ranging from physiological toxicity to severe environmental fire hazards. Nurses must diligently enforce the following precautions:
- Prevent Oxygen Toxicity: Never deliver more than the prescribed concentration or flow rate. Prolonged exposure to high concentrations of oxygen can cause pulmonary oxygen toxicity, leading to alveolar damage and acute respiratory distress syndrome.
- Avoid Unauthorized Adjustments: Never increase or decrease the flow of oxygen while the cannula is merely resting in the patient's nostrils without a medical order. Always monitor SpO2 frequently to guide titration.
- Maintain Humidification: Ensure that the humidifier bottle is always at least 1/3rd full with sterile distilled water. Dry oxygen damages the mucosal lining, impairs ciliary action, and thickens respiratory secretions.
Oxygen supports and intensely accelerates combustion. While it does not burn on its own, it causes other materials to ignite easily and burn rapidly.
- No Smoking Rule: Promote strict safety measures. Inform the patient and all visitors that smoking is absolutely not permitted in the area of oxygen use.
- Signage: Place prominent "NO SMOKING / OXYGEN IN USE" signs on the patient's room door and near the bed.
- Fire Extinguishers: Always know the location of the nearest fire extinguisher close to the room.
- Electrical Safety: Do not use electrical appliances (such as electric razors, heating pads, or radios with frayed cords) close to the oxygen source to avoid accidental sparking.
- Avoid Oil and Grease: Oil or grease should never be used on the oxygen regulator, cylinder valves, or connections. Oil combined with pressurized oxygen can result in a violent, spontaneous explosion.
- Cylinder Storage: O2 cylinders should be stored securely upright at a low temperature, away from heat sources or direct sunlight.
- Frequent Changes: Oxygen therapy equipment is a potential source of bacterial contamination. Tubing, masks, and humidifiers should be changed frequently according to hospital policy.
- Nasal Cannula Hygiene: Change the nasal cannula every 8 hours, or more often if it becomes visibly soiled with mucous or blood.
- What is oxygenation, and how does it differ from oxygen inhalation?
- What are the primary medical indications for initiating oxygen inhalation?
- How is hypoxia defined, and what are its early versus late signs and symptoms?
- What are the different delivery systems of oxygen, and how do their FiO2 capacities differ?
- What are the crucial nursing steps to safely administer oxygen to a patient?
- What environmental and physiological precautions must be strictly enforced during oxygen administration?
- Health Learning Material Center. Institute of Medicine, Tribhuwan University. Fundamentals of Nursing (2nd ed. reprint, 2010). Kathmandu: Heidal Press, Dillibazar.
- Basvanthappa, B.T. (2004). Fundamentals of Nursing. New Delhi: Jaypee Brothers.
- Perry, A.G. and Potter, P.A. (2007). Basic Nursing Essentials For Practice (6th ed.). Mosby.
- Giri, M. and Sharma, P. (2013). Essential Fundamental Of Nursing (1st ed.). Kathmandu: Medhavi Publication.
- Pathak, S. and Devkota, R. (2011). A Textbook Of Fundamentals of Nursing (2nd ed.). Kathmandu: Vidyarthi Prakashan.
- Taylor, C.R. and Lillis, C. (2008). Fundamental Of Nursing (Volume 1). Lippincott William and Wilkins.
- Skidmere, L. Nursing Drug Reference (2009). Mosby.
