
It is important to differentiate between these two commonly confused medical terms before discussing the specific pathology of the adenoids:
| Term | Definition |
|---|---|
| Adenitis | A general term referring to the inflammation of a gland or a lymph node anywhere in the body. For example, cervical adenitis refers to the swelling and inflammation of lymph nodes in the neck. |
| Adenoiditis | A specific term referring exclusively to the inflammation and enlargement of the adenoids (the pharyngeal tonsils) located in the nasopharynx. |
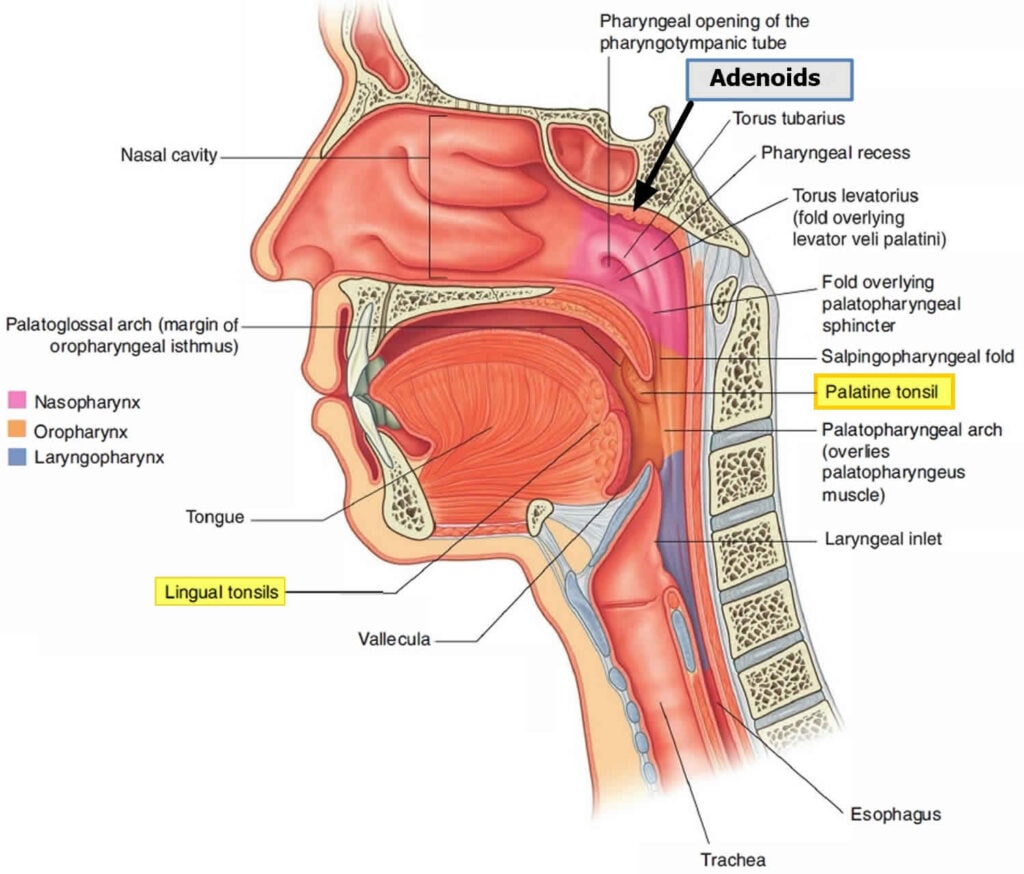
- Adenoids (also known as pharyngeal tonsils) are small masses of lymphatic tissue located at the back of the throat just above the tonsils, in the nasopharynx (the area just behind the nose).
- They are part of the lymphatic system and the immune system, helping the body to fight infection by trapping and destroying pathogens (particularly bacteria and viruses).
- They store white blood cells and antibodies.
- Tonsils and adenoids act as the first line of defense in the throat against inhaled or ingested pathogens.
- They start to grow from birth and reach their maximum size at the age of 5.
- At the age of 7 years old, they start to shrink away, and by adulthood, they disappear completely.
Adenoiditis is the inflammation and enlargement of the adenoid tissue, usually caused by an infection. It is a communicable disease that spreads through airborne respiratory droplets and saliva. If the adenoids are infected with pathogens and allergens, it causes adenoiditis. The condition often follows an episode of acute tonsillitis and is broadly classified into acute and chronic adenoiditis.
- It occurs predominantly in children below 15 years of age.
- The condition is especially common in children under 7 years old.
- The incidence decreases with age. The condition is rare after 15 years of age, although not unheard of.
- Adenoiditis is a very common disease, with approximately 10 million cases reported each year.
- Recurring infections in the throat, neck, and head.
- Infection of the tonsils (tonsillitis).
- Children are generally more susceptible to adenoiditis than adults.
The condition is primarily caused by infections from various viral and bacterial agents:
- Bacterial Causes:
- Group A beta-hemolytic streptococcus (Streptococcus pyogenes): The most frequent culprit behind adenoiditis, which is the same bacteria often responsible for strep throat.
- Streptococcus pneumoniae
- Moraxella catarrhalis
- Staphylococcus aureus
- Viral Causes:
- Adenovirus
- Rhinovirus
- Paramyxovirus
- Epstein-Barr virus (EBV)
- The process begins due to trauma or infections in the nasopharynx.
- This leads to the inflammation of the adenoid tissue.
- Inflammation triggers the release of inflammatory mediators.
- This results in localized tissue edema, pain, heat, and redness.
- This cascade culminates in the clinical condition of Adenoiditis.
Swollen adenoids can physically block or restrict airways. Adenoiditis is sometimes accompanied by tonsillitis, and repeated bouts may lead to permanently enlarged adenoids. Common clinical features include:
- Nasal Obstruction or Difficult Breathing: The enlarged adenoids block the nasal passages, leading to a stuffy feeling and forcing the patient into mouth breathing.
- Jaw Deformities & Facial Changes: In children, continuous mouth breathing due to nasal obstruction leads to prominent teeth and thin upper lips. Generally, children will develop a "long face" (often termed adenoid facies) if there is chronic adenoiditis.
- Foul Smelling Breath: Due to mouth breathing and trapped mucus/bacteria.
- Voice Impairment: Including a distinctly nasal speech.
- Fever and Malaise: Systemic signs of an underlying infection.
- Sore Throat and Difficulty Eating: Pain caused by inflammation can make eating very difficult, particularly for children.
- Earache and Hearing Loss: The adenoids are located near the openings of the Eustachian tubes, which connect the middle ear to the back of the throat. Inflammation can block these tubes, leading to fluid buildup in the middle ear and subsequent hearing loss.
- Glue Ear: The accumulation of thick, sticky fluid in the middle ear behind the eardrum, a common consequence of chronic adenoiditis blocking the Eustachian tube.
- Snoring and Sleep Apnea: Adenoid enlargement can heavily obstruct the airway during sleep, resulting in noisy breathing, snoring, and in severe cases, sleep apnea (where breathing temporarily stops).
- Recurrent Cough and Discharging Cough: Mucus from the inflamed adenoids can drain down the throat, causing a post-nasal drip and a persistent cough with phlegm.
The diagnosis of adenoiditis relies on a combination of clinical assessment and specific investigations:
- History Collection: A thorough medical history assessing symptoms, onset, and recurrence.
- Physical Examination: A careful examination of the throat can reveal the presence of enlarged, inflamed adenoids.
- Throat Swabs / Throat Swab Culture: Taken to determine the specific bacterial or viral pathogens causing the infection.
- Blood Test and Blood Culture: To identify systemic infection markers and isolate pathogens.
- X-rays of Head and Neck: A lateral view X-ray of the neck soft tissue is highly effective at demonstrating the narrowing of the nasopharynx due to enlarged adenoids.
- Posterior Rhinoscopy: Direct visualization of the back of the nasal cavity.
- Nasopharyngoscopy: Passing a flexible scope through the nose to view the adenoids.
- CT scan: To determine the exact size of the adenoids and the full extent of the infection or anatomical blockage.
The approach to managing adenoiditis depends heavily on the severity of the symptoms and the patient's age. If symptoms are mild and not significantly impacting daily life, conservative treatment may be sufficient.
- Viral Adenoiditis: Treatment with analgesics or antipyretics is often sufficient to manage symptoms while the virus runs its course.
- Bacterial Adenoiditis (Underlying Infection): If an underlying bacterial infection is suspected or confirmed via culture, antibiotics are prescribed. Common antibiotics include Amoxicillin, Cephalosporins, or Ampicillin (often used at a dosage of 500mg-1g every 6 hours).
- Antihistamines: Medications like Chlorphenamine can help reduce inflammation and congestion. The dosage is typically 4 mg orally t.d.s, adjusted according to age, for a period of 7 days.
- Topical Nasal Steroids: Nasal sprays containing corticosteroids (like Betamethasone) can effectively reduce local inflammation and improve nasal breathing.
- Pain Management: Pain relief can be achieved with analgesics like Paracetamol (PCT) 500mg-1g three times a day, or Tramadol 75 mg for more severe pain.
- Mouth Care: Encouraging good oral hygiene practices, such as regular brushing and flossing, can help prevent secondary infections and promote healing.
Adenoidectomy is the surgical removal of the adenoids. Note: Because adenoids naturally shrink as a child grows older, surgery is generally considered a last resort. It is typically performed after the age of one year if conservative treatment fails.
- Four or more episodes of recurrent adenoiditis.
- Persisting symptoms even after 2 full courses of antibiotic therapy.
- Sleep disturbance with severe nasal airway obstruction (e.g., Sleep Apnea).
- Persistent nasal speech impacting development or quality of life.
While adenoiditis is usually a temporary condition, it can lead to significant complications if left untreated:
- Ear infections (Otitis Media): Blocked Eustachian tubes can result in recurrent ear infections and the development of GLUE EAR.
- Sinusitis: The swollen tissues can block the sinus cavity, leading to secondary sinus infections.
- Pneumonia and Bronchitis: Lower respiratory tract infections can occur if infected mucus is aspirated.
- Recurrent Infections: Persistent inflammation can increase overall susceptibility to repeated infections in the respiratory system.
- Quinsy (Peritonsillar Abscess): A rare complication where an abscess forms in the tissue surrounding the tonsils, requiring immediate drainage.
- Mastoiditis: In severe cases, the infection can spread from the middle ear to the mastoid bone located behind the ear, causing dangerous inflammation.
| No. | Nursing Diagnosis | Interventions & Rationale |
|---|---|---|
| 1 | Ineffective Airway Clearance related to nasal obstruction, enlarged adenoids, and excessive mucus production. |
|
| 2 | Acute Pain related to the inflammation of the pharyngeal tonsils and throat tissues. |
|
| 3 | Impaired Swallowing / Imbalanced Nutrition: Less than body requirements related to severe throat pain upon swallowing. |
|
- Admission & Explanation: Inform the patient and parents about the nature of the surgery, its purpose, and what to expect post-operatively to reduce fear and anxiety.
- Informed Consent: Ensure the patient (or parent/guardian) provides written consent for both admission and the surgical procedure.
- Baseline Assessment & Vital Labs: Check baseline vital signs (temperature, pulse, BP, respiration). Crucially, evaluate laboratory tests assessing bleeding and clotting times (e.g., PT, PTT) because the adenoid bed is highly vascular and prone to bleeding.
- Physical Examination: Assess weight, height, and nutritional status to ensure overall health. Check for loose teeth, which is a vital step in pediatric patients to prevent tooth dislodgement and aspiration during intubation.
- Counseling and Reassurance: Provide emotional support. Address patient questions and provide access to spiritual care/religious leaders if desired.
- Site Preparation & Obstacle Removal: Ensure all jewelry, dentures, and prosthetics are removed to prevent complications in the theater.
- NPO (Nil Per Os): Food and drink are strictly withheld according to the doctor's orders to prepare for surgery and prevent aspiration during anesthesia.
- IV Line & Rehydration: Insert an IV line to administer fluids and medications, ensuring adequate hydration prior to surgery.
- Premedication & Procedures: Administer prescribed pre-anesthetic medications. Perform any requested procedural preparations (though NGT or catheterization is rare for standard adenoidectomy).
- Rest and Sleep: Encourage patients to rest. Meanwhile, prepare the post-operative bed with necessary equipment like oxygen and suction apparatus.
- Reception from Theater: Receive the patient from the operating room and take handover instructions from the surgical team. Transfer them to a warm, comfortable bed.
- Positioning (Crucial Airway Management): Position the patient on their side (lateral position) or prone with the head turned to the side. Rationale: This position facilitates the drainage of blood and oral secretions out of the mouth, preventing pooling at the back of the throat and eliminating the risk of aspiration.
- Bleeding and Shock Monitoring: Closely observe for signs of hemorrhage. Specifically, watch the patient for continuous, frequent swallowing. This is a classic sign of concealed bleeding (the patient is swallowing blood pooling from the surgical site). Inspect the throat and vomitus for fresh, bright red blood.
- Vital Signs: Monitor temperature, pulse, BP, respiration, and oxygen saturation regularly. Tachycardia, restlessness, or hypotension may indicate internal bleeding.
- Pain Management: Administer prescribed analgesics to provide comfort. Avoid NSAIDs like aspirin, which can interfere with platelet function and increase the risk of post-operative bleeding.
- Nutrition & Fluid Balance: Administer IV fluids and maintain a strict fluid balance chart. Once the patient is fully awake and the gag reflex has returned, initiate cold, clear fluids. Avoid red or brown colored liquids as these can be confused with blood if the patient vomits. Progress to a soft, non-irritating diet. Avoid hot, spicy, or scratchy foods (like toast or chips) that could dislodge clots.
- Wound Care & Hygiene: Surgical incisions are internal, so there is no external dressing. Assist with general body hygiene and keep the bed clean and dry. Use gentle saline mouth rinses if ordered to keep the oral cavity clean.
- Comfort Measures: An ice collar may be applied to the neck to reduce edema, promote vasoconstriction, and decrease bleeding risk.
- Psychological Care & Physiotherapy: Provide emotional support. Encourage breathing exercises and early mobility, while ensuring the patient gets adequate rest and sleep to promote healing.
- Explanation of Surgery & Prevention: Ensure the patient and parents have a clear understanding of the surgery, the underlying condition, and hygiene measures to prevent secondary infections.
- Treatment Completion: Strongly emphasize the importance of finishing the prescribed treatment plan, especially antibiotic courses.
- Dietary Restrictions: Advise continuing a soft, cool diet for several days. Explain the benefits of a balanced diet for overall health and recovery, but warn against hard or acidic foods.
- Activity Restriction: Patients should engage in light exercise but must avoid strenuous activities, heavy lifting, or vigorous nose blowing and coughing, as this increases pressure in the head and can dislodge healing blood clots.
- Symptom Education: Inform parents that referred ear pain is a very common occurrence a few days after adenoid/tonsil surgery and does not necessarily mean there is an ear infection. Bad breath is also a normal part of the healing process.
- Danger Signs (When to Return): Instruct the patient or parents to seek immediate medical attention if they notice any fresh bleeding from the mouth or nose, a persistent high fever, or if pain prevents the child from drinking, leading to risk of dehydration.
- Follow-up Appointment: Stress the critical importance of attending scheduled follow-up appointments to monitor surgical healing.
- Rest and Sleep: Adequate rest and sleep are encouraged for optimal healing at home.
Quick Quiz
Table of Contents
ToggleENT Tumors Quiz
Medical Nursing - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
ENT Tumors Quiz
Medical Nursing
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.