
Nasal Polyposis Lecture Notes
I. Definition of Nasal Polyps
- Etymology: The word "Polyp" is a Latin word meaning polypus, i.e., "many footed".
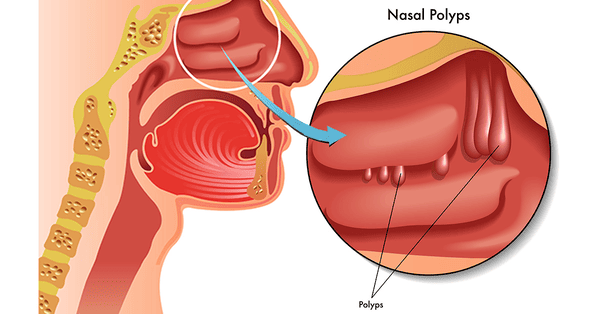
- Definition: The polypus is a projection of hypertrophied edematous mucous membrane. They are benign, soft, teardrop-shaped growths that develop in the nasal lining.
- These are not true tumors but rather an inflammatory overgrowth of the tissue lining the nasal cavity.
- Histology: It consists of loose fibroedematous tissue covered with columnar ciliated epithelium.
- Types: They are broadly divided into two main types:
- Bilateral ethmoidal polypi.
- Antrochoanal polyp.
II. Epidemiology
- The prevalence of nasal polyps (NP) in the population has been grossly estimated as 1–4%.
- It increases with age, reaching a peak in those aged 50 years and older.
- Gender Ratio: Male to Female ratio is 2:1.
- Nasal polyposis occurs with a high frequency in groups of patients having specific airway diseases.
- Genetic inheritance has been proposed as a possible etiology of NP.
III. Ethmoidal Polyps
A. Aetiology & Associated Diseases
The aetiology of nasal polyposis is very complex. They may arise in inflammatory conditions of the nasal mucosa (rhinosinusitis), disorders of ciliary motility, or due to abnormal composition of nasal mucus (e.g., cystic fibrosis). Various diseases associated with the formation of nasal polypi are:
- Chronic rhinosinusitis: Polypi are seen in chronic rhinosinusitis of both allergic and nonallergic origin. Nonallergic rhinitis with eosinophilia syndrome (NARES) is a form of chronic rhinitis associated with polypi.
- Asthma: Seven per cent (7%) of the patients with asthma of atopic or non-atopic origin show nasal polypi.
- Aspirin intolerance: Some patients with aspirin intolerance may show polypi. Samter's Triad consists of: nasal polypi, bronchial asthma, and aspirin intolerance/sensitivity.
- Cystic fibrosis: Twenty per cent (20%) of patients with cystic fibrosis form polypi. It is due to abnormal mucus.
- Allergic fungal sinusitis: Almost all cases of fungal sinusitis form nasal polypi.
- Kartagener syndrome: This consists of bronchiectasis, sinusitis, situs inversus, and ciliary dyskinesis.
- Young syndrome: It consists of sinopulmonary disease and azoospermia.
- Churg–Strauss syndrome: Consists of asthma, fever, eosinophilia, vasculitis, and granuloma.
- Nasal mastocytosis: It is a form of chronic rhinitis in which nasal mucosa is infiltrated with mast cells but few eosinophils. Skin tests for allergy and IgE levels are normal.
B. Pathogenesis & Site of Origin
- Pathogenesis: Nasal mucosa, particularly in the region of the middle meatus and turbinate, becomes edematous due to the collection of extracellular fluid (ECF) causing polypoidal change.
- Polypi which are sessile in the beginning become pedunculated due to gravity and excessive sneezing.
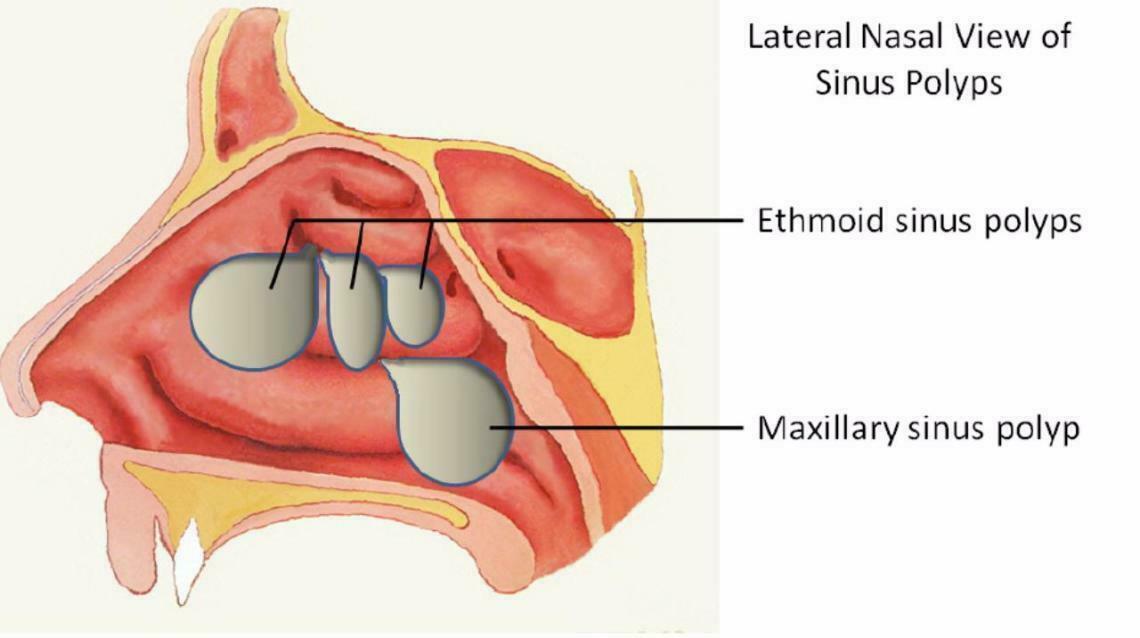
- Site of Origin: Multiple nasal polypi always arise from the lateral wall of the nose, usually from the middle meatus.
- Common sites include: uncinate process, bulla ethmoidalis, ostia of sinuses, and the medial surface and edge of the middle turbinate.
- Note: Allergic nasal polypi almost never arise from the septum or the floor of the nose.
C. Pathology & Histologic Findings
- In early stages, the surface of nasal polypi is covered by pseudostratified ciliated columnar epithelium like that of normal nasal mucosa.
- Later, it undergoes a metaplastic change to transitional and squamous type on exposure to atmospheric irritation.
- There is thickening of the epithelial basement membrane.
- The submucosa (stroma) is highly edematous, showing large intercellular spaces filled with serous fluid.
- Vascularization is poor and it lacks innervation.
- There is hyperplasia of the seromucous gland when compared with the inferior or middle turbinate.
- Eosinophils are the most commonly found inflammatory cell in NP (found in 80-90% of polyps).
- Another inflammatory cell, the neutrophil, occurs in 7% of cases. This type of NP associates with Cystic Fibrosis (CF), primary ciliary dyskinesia, or Young syndrome.
D. Symptoms & Signs
Symptoms:
- Multiple polypi can occur at any age but are mostly seen in adults.
- Nasal stuffiness / Nasal obstruction: Leading to total nasal obstruction; often the presenting symptom. Difficulty breathing through the nose, feeling like the nose is blocked.
- Anosmia / Loss of smell: Partial or total loss of sense of smell, along with loss of taste.
- Postnasal drip & Discharge: Mucus dripping down the back of the throat. Nasal discharge may be watery (allergy), yellowish, mucoid, or purulent (pus) due to associated sinusitis.
- Headache & Facial pain: Aching, pressure, or fullness in the face, especially around the sinuses, due to associated sinusitis.
- Sneezing: Due to associated allergy (along with nasal congestion and runny nose).
- Snoring & Sleep apnea: Loud breathing during sleep or pauses in breathing due to obstruction.
- Mass protruding from the nostril.
Signs:
- Polypi appear as smooth, glistening masses, often pale in color (described as grey fleshy masses that look like freshly skinned grapes).
- They may be sessile or pedunculated.
- They are insensitive to probing and do not bleed on touch.
- Often they are multiple and bilateral.
- Protruding masses from the nostril may appear pink and vascular, simulating a neoplasm.
- Long-standing cases present with broadening of the nose and increased intercanthal distance.
- Nasal cavity may show purulent discharge due to associated sinusitis.
E. Staging & Diagnosis
Probing of a solitary ethmoidal polyp may be necessary to differentiate it from hypertrophy of the turbinate or a cystic middle turbinate.
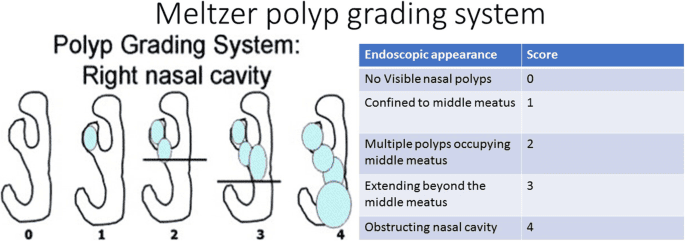
Staging Polyps (Meltzer et al):
- Stage I: Limited to the extent of the middle turbinate.
- Stage II: Extending beyond the limit of the middle turbinate.
- Stage III: Approaching the inferior turbinate.
- Stage IV: Going up to the floor of the nose.
Diagnosis & Investigations:
- Physical/Clinical examination: Diagnosis can be easily made by inspection of the nasal cavity.
- Nasal endoscopy: A thin, flexible tube with a camera is inserted into the nose to visualize the polyps.
- CT scan or MRI of paranasal sinuses: Essential to exclude bony erosion and expansion suggestive of neoplasia. It shows the size and location of the polyps and helps to plan surgery.
- Important: Simple nasal polypi may sometimes be associated with malignancy underneath, especially in people above 40 years, and this must be excluded by histological examination.
Differential Diagnosis of Ethmoidal Polyps:
- Antrochoanal polypi
- Squamous or transitional cell papilloma
- Meningocele / meningoencephalocele
- Enlarged turbinates
- Malignancy of nose / PNS
- Nasopharyngeal fibroma
- Granulomatous masses
- Bleb of mucus plug
IV. Antrochoanal Polyp (Killian’s Polyp)
A. Aetiology & Pathogenesis
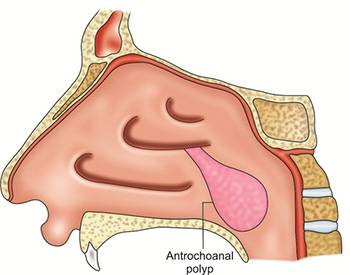
- This polyp arises from the mucous membrane of the floor and medial wall of the maxillary sinus close to the accessory ostium.
- It comes out of the sinus and starts growing towards the choana and nasal cavity.
- Three parts of the polyp:
- Antral: which is a thin stalk.
- Nasal: which is flat from side to side.
- Choanal: which is round and globular.
- Aetiology: The exact cause is unknown, but nasal allergy coupled with sinus infection is incriminated.
- They are commonly seen in adolescence.
- For an unknown reason, ACP predominates in the male population.
- Usually, they are single and unilateral.
B. Symptoms, Signs & Diagnosis
- Symptoms:
- Unilateral nasal obstruction is the presenting symptom.
- Obstruction may become bilateral when the polyp grows into the nasopharynx and starts obstructing the opposite choana.
- Voice may become thick and dull due to hyponasality.
- Nasal discharge, mostly mucoid, may be seen on one or both sides.
- Conductive deafness due to eustachian tube dysfunction.
- Snoring.
- Signs:
- As the antrochoanal polyp grows posteriorly, it may be missed on anterior rhinoscopy initially.
- Posterior rhinoscopy may show a smooth, greyish-white, spherical mass in the choana, sometimes projecting below the soft palate.
- It is soft and can be moved up and down with a probe. A large polyp may protrude from the nostril with a pink congested look on its exposed part.
- Diagnosis:
- X-rays of paranasal sinuses may show opacity of the involved antrum.
- X-ray (lateral view), soft tissue nasopharynx, reveals a globular swelling in the postnasal space. It is differentiated from angiofibroma by the presence of a column of air behind the polyp.
- CT scan PNS, particularly osteomeatal complex (coronal and axial sections).
V. Differences: Antrochoanal vs. Ethmoidal Polyps
| Antrochoanal Polyp | Ethmoidal Polyps |
|---|---|
| Common in children / adolescents. | Common in adults. |
| Aetiology is infection. | Aetiology allergic/multifactorial. |
| Single mass and trilobed. | Multiple, like a bunch of grapes. |
| Unilateral. | Bilateral. |
| Site of origin is maxillary sinus near the ostium. | Ethmoidal sinuses, uncinate process, middle turbinate and middle meatus. |
| Recurrence is uncommon, if removed completely. | Recurrence is common. |
VI. Management of Nasal Polyps
A. Conservative / Medical Management
Medical treatment aims to treat the cause, addressing underlying conditions like allergies, sinusitis, or aspirin sensitivity.
- Antihistamines: Early polypoidal changes with edematous mucosa may revert to normal with antihistaminics and control of allergy.
- Saline irrigation: Using saline solution to flush out the nasal passages.
- Antibiotics: Prescribed for any concurrent bacterial sinus infections.
- Intranasal Corticosteroids (INS): E.g., Betamethasone 50mg instilled twice daily into each nostril for 4 weeks, with the patient lying flat for 3 minutes after instillation.
- Benefits: Reduce polyp size, increase nasal patency, reduce rhinitis symptoms, reduce loss of sense of smell, reduce recurrence, and provide safety.
- Side effects of INS: Excoriation and bleeding. Beclomethasone dipropionate nasal spray is associated with increased intraocular pressure. Delay in growth in prepubescent children has led to an FDA warning on all INS.
- Systemic Corticosteroids: Can be given as tablets or depot-injections.
- Oral prednisolone: 25mg/daily for 10-14 days.
- Depot-injection: corresponds to 100mg prednisolone.
- This may serve as a "medical polypectomy".
- Risks: Insomnia, personality change, truncal obesity, weight gain, glaucoma, cataracts, osteoporosis (>3 months usage), peptic ulcer disease, increased infection incidence.
- Contraindications: Exclude patients with hypertension, peptic ulcer, diabetes, pregnancy, and tuberculosis.
B. Surgical Management
Removal of the polyps through surgery may be necessary if polyps are large, recurrent, or unresponsive to medical treatment.
Surgical Options:
- Polypectomy: One or two pedunculated polyps can be removed with a snare.
- Procedure: Local anesthesia is achieved by spraying lignocaine 2% into the nose and adrenaline 1:100,000; wait for 5 minutes. Open nostrils using a nasal speculum under good lighting. Pass a polypectomy snare, maneuver it to catch the polyp, and remove its base. Repeat the process until all are removed. Pack the nose if excessive bleeding occurs. General anesthesia may be used for complex cases or poor tolerance.
- Intranasal ethmoidectomy: When polypi are multiple and sessile, they require uncapping of the ethmoidal air cells by the intranasal route.
- Extranasal ethmoidectomy: Indicated when polypi recur after intranasal procedures and surgical landmarks are ill-defined. Approach is through the medial wall of the orbit by an external incision, medial to the medial canthus.
- Jansen Horgan’s transantral ethmoidectomy: Done in case maxillary antra also needs to be cleared. Ethmoids are approached through the medial wall of maxillary antra.
- Antrum washout or Antrostomy: Procedures to clear out the sinuses and improve drainage. For antrochoanal polyps, avulsion (nasal/oral route) is used. Caldwell-Luc operation was historically used for recurrences to remove the root and drain the sinus.
- Endoscopic Sinus Surgery (FESS): Functional Endoscopic Sinus Surgery has superseded other modes of polyp removal. Done with various endoscopes (0°, 30°, and 70° angulation). Polypi are removed accurately, ethmoid cells are removed, and drainage/ventilation is provided to maxillary, sphenoidal, or frontal sinuses.
- Microdebrider: Polypectomy using a microdebrider is a modern addition in the surgical treatment of nasal polypi.
VII. Points to Remember & Red Flags
- If a polypus is red and fleshy, friable and has a granular surface, especially in older patients, it suggests malignancy.
- A simple nasal polyp may masquerade as a malignancy underneath. Hence, all polypi should be subjected to histopathology.
- A simple polyp in a child may be a glioma, an encephalocele or a meningoencephalocele. It should always be aspirated and the fluid examined for CSF. Careless removal would result in CSF rhinorrhoea and meningitis.
- Multiple nasal polypi in children may be associated with mucoviscidosis (Cystic Fibrosis).
- Epistaxis and orbital symptoms associated with a polyp should always arouse the suspicion of malignancy.
- Potential complications of nasal polypi include anosmia, cranial neuropathies, osteitis, and proptosis.
VIII. Causes of Nasal Obstruction
| Unilateral Obstruction | Bilateral Obstruction |
|---|---|
|
Vestibule: Furuncle, Vestibulitis, Stenosis of nares, Atresia, Nasoalveolar cyst, Papilloma, Squamous cell carcinoma. Nasal cavity: Foreign body, Deviated nasal septum (DNS), Hypertrophic turbinates, Concha bullosa, Antrochoanal polyp, Synechia, Rhinolith, Bleeding polypus of septum, Benign/malignant tumours, Unilateral sinusitis, Unilateral choanal atresia. |
Vestibule: Bilateral vestibulitis, Collapsing nasal alae, Stenosis of nares, Congenital atresia of nares. Nasal cavity: Acute/chronic rhinitis, Rhinitis medicamentosa, Allergic rhinitis, Hypertrophic turbinates, DNS, Nasal polypi, Atrophic rhinitis, Rhinitis sicca, Septal haematoma/abscess, Bilateral choanal atresia. Nasopharynx: Adenoid hyperplasia, Large choanal polyp, Thornwaldt’s cyst, Adhesions between soft palate and posterior wall, Large tumours. |
IX. Prevention
- Avoiding triggers: Identifying and avoiding allergens and irritants, such as dust mites, pollen, smoke, and strong odors.
- Managing underlying conditions: Actively treating sinusitis, allergies, asthma, and other conditions that contribute to chronic inflammation.
- Regular nasal hygiene: Using saline sprays, nasal irrigation, and other methods to keep the nasal passages clear and wash away allergens.
I. Nursing Care Plan for Nasal Polyps
| No. | Nursing Diagnosis | Interventions & Rationale |
|---|---|---|
| 1 | Ineffective Airway Clearance related to nasal obstruction from polyp overgrowth and excessive thick secretions. |
|
| 2 | Acute Pain / Impaired Comfort related to sinus pressure, facial pain, and headaches associated with nasal polyps and sinusitis. |
|
| 3 | Disturbed Sleep Pattern related to nocturnal nasal obstruction, snoring, and potential sleep apnea. |
|
II. Pre-Operative Care (Tailored for Polypectomy / FESS)
- Admission & Procedure Explanation: Explain the polypectomy or FESS procedure to the patient. Discuss the use of endoscopes and assure them that there are typically no external incisions.
- Informed Consent: Ensure the patient signs the surgical consent form after the surgeon has explained the risks and benefits.
- Baseline Assessment & Coagulation Studies: Obtain vital signs. Crucially, check bleeding profiles (PT, PTT, INR), as the nasal mucosa is highly vascular and FESS involves operating near critical structures.
- Anesthesia Preparation: For local anesthesia cases, explain the use of topical sprays (lignocaine/adrenaline). For general anesthesia, ensure standard NPO (Nil Per Os) guidelines are strictly followed.
- Removal of Prosthetics: Have the patient remove dentures, glasses, and jewelry.
- Psychological Support: Reassure the patient, especially regarding the post-operative sensation of nasal packing, which can be claustrophobic for some.
- IV Access: Establish a peripheral IV line for fluids and pre-operative medications (e.g., prophylactic antibiotics or anxiolytics).
III. Post-Operative Care (Tailored for Polypectomy / FESS)
- Immediate Reception & Vital Signs: Receive the patient from the PACU. Monitor BP and pulse closely. Tachycardia and hypotension may indicate excessive concealed bleeding.
- Positioning: Place the patient in a Semi-Fowler's position (head elevated 30-45 degrees). Rationale: This minimizes facial edema, reduces venous pressure in the head (decreasing bleeding risk), and aids drainage.
- Bleeding Observation: Monitor the nasal drip pad (mustache dressing) for excessive bright red bleeding. A small amount of blood-tinged serosanguinous drainage is normal. Assess the back of the throat with a penlight for continuous swallowing, a key sign of posterior hemorrhage.
- Airway & Breathing: Since the nose will likely be packed with gauze or sponges, the patient must breathe through their mouth. Monitor oxygen saturation. Provide humidified oxygen via face tent if needed to prevent mucosal drying.
- Pain Management: Administer prescribed analgesics. Apply ice packs to the bridge of the nose or cheeks to reduce pain, swelling, and bleeding.
- Oral Hygiene: Provide frequent mouth care and sips of water (once gag reflex returns and patient is not nauseated) to relieve severe dry mouth caused by obligatory mouth breathing.
- Neurological Checks (Crucial for FESS): Monitor for visual changes (double vision, loss of vision), periorbital swelling, or clear watery nasal discharge (rhinorrhea). Rationale: The ethmoid sinuses are adjacent to the orbits and the cribriform plate; surgical breaches can cause optic nerve damage or CSF leaks.
IV. Advice on Discharge or Health Education
- Nasal Packing Management: If discharged with nasal packing, instruct the patient not to manipulate or pull at the packing. Inform them of the scheduled removal date.
- Activity Restrictions: Strictly avoid nose blowing, strenuous exercise, heavy lifting, and bending over for 1-2 weeks to prevent dislodging clots and causing hemorrhage.
- Sneeze with Mouth Open: Instruct the patient to sneeze with their mouth open to prevent high pressure build-up in the nasal cavities.
- Nasal Irrigations: Teach the patient how to perform sterile saline nasal irrigations (once packing is removed) to clear out crusts and blood clots, promoting mucosal healing.
- Medication Compliance: Emphasize the strict continuation of intranasal corticosteroids, oral antibiotics, or antihistamines as prescribed to prevent polyp recurrence.
- Dietary Advice: Maintain adequate hydration. Avoid very hot liquids or spicy foods for a few days, as steam and spices can cause vasodilation and trigger nosebleeds.
- Danger Signs (When to Return): Educate the patient to report immediately to the ER if they experience:
- Excessive, continuous bright red bleeding that does not stop with ice or pressure.
- Clear, watery fluid dripping from the nose (potential CSF leak).
- High fever, severe headache, or stiff neck (signs of meningitis).
- Any visual changes or severe swelling around the eyes.