
An adverse drug reaction is a broad term encompassing any unwanted, uncomfortable, or dangerous effect caused by a drug. Understanding ADRs, their classifications, and underlying pharmacological mechanisms is a cornerstone of safe clinical practice and patient care.
- Definition of terms associated with Adverse Drug Reactions (ADRs).
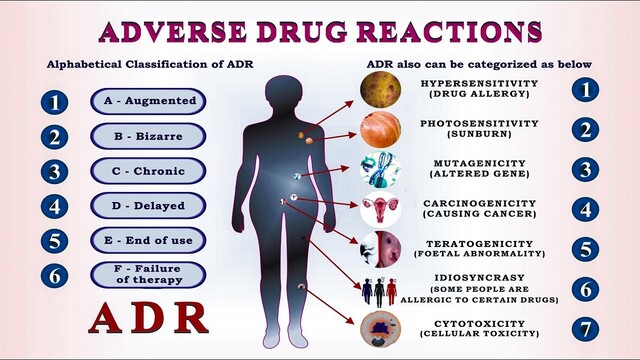
- Classification of ADRs.
- Discussion on each type of ADR with comprehensive pharmacological examples.
It is crucial to differentiate between an event and a reaction to establish causality in pharmacovigilance.
- Adverse Event (AE) / Effect or Experience: Any untoward medical occurrence that may present during treatment with a pharmaceutical product but which does not necessarily have a causal relationship with this treatment.
- Adverse Drug Event (ADE): An AE which happens in a patient taking a drug.
- Adverse: Untoward, unintended, possibly causing harm (noxious).
- Adverse Drug Reaction (ADR): Any noxious change which is suspected to be due to a drug, occurs at doses normally used in man, requires treatment or decrease in dose, or indicates caution in future use of the same drug. Therefore, an adverse drug reaction is an ADE in which a causal association is suspected or established between the drug and the event.
- Drug Administered: The patient is given a medication.
- New Condition/Symptom (ADE): The patient develops an untoward clinical manifestation.
- Drug Suspected? (Yes): The clinician suspects the drug is responsible.
- Check Literature:
- Documented: If the reaction is documented for the product or similar class of products → Highly suggestive of ADR.
- Not documented in literature: The physician must test via dechallenge and rechallenge.
- Dechallenge/Rechallenge Process (for undocumented effects):
- Drug Continued: Worsening of symptoms occurs. The clinician must ask: Are there any other possible causes? (Concomitant therapy, underlying conditions).
- Drug Discontinued (Dechallenge): If symptoms improve, this is a Positive (+ve) Dechallenge.
- Drug Restarted (Rechallenge): If symptoms recur upon re-administration, this is a Positive (+ve) Rechallenge, confirming the ADR.
Adverse drug reactions can be classified using several parameters to aid in diagnosis, reporting, and management.
- Acute: Occurs in < 60 minutes (e.g., Anaphylaxis).
- Sub-acute: Occurs in 1 to 24 hours (e.g., Maculopapular rash).
- Latent: Occurs in > 2 days (e.g., Drug-induced liver injury, teratogenesis).
- Minor ADRs: No therapy, antidote, or prolongation of hospitalization is required.
- Moderate ADRs: Requires a change in drug therapy, specific treatment, or prolongs hospital stay by at least 1 day.
- Severe ADRs: Potentially life-threatening, causes permanent damage, or requires intensive medical treatment.
- Lethal: Directly or indirectly contributes to the death of the patient.
The Wills and Brown classification system categorizes ADRs alphabetically from A to H, and U.
- Type A (Augmented)
- Type B (Bizarre)
- Type C (Chemical)
- Type D (Delayed)
- Type E (Exit / End of treatment)
- Type F (Familial)
- Type G (Genotoxicity)
- Type H (Hypersensitivity)
- Type U (Unclassified)
- Reactions which can be predicted from the known pharmacology of the drug.
- Dose-dependent.
- Can be alleviated by a dose reduction.
- Anticoagulants → Bleeding: Drugs like Warfarin (Vitamin K antagonist) or Heparin (activates antithrombin III) have a primary therapeutic action of preventing clot formation. An augmented effect of this known pharmacology naturally leads to spontaneous bleeding or hemorrhage if the dose is too high (e.g., high INR/aPTT).
- Beta Blockers → Bradycardia: Medications like Metoprolol or Propranolol competitively block beta-1 adrenergic receptors in the heart, preventing sympathetic (epinephrine/norepinephrine) stimulation. While intended to lower blood pressure or control arrhythmias, exaggerated blockade excessively slows the SA node, causing predictable bradycardia.
- Nitrates → Headache: Nitroglycerin is converted to nitric oxide (NO), stimulating cGMP and causing smooth muscle relaxation. While intended for coronary arteries to treat angina, it also causes profound vasodilation of the meningeal and cerebral blood vessels, predictably leading to a throbbing headache.
- Prazosin → Postural hypotension: Prazosin is an alpha-1 adrenergic antagonist. It blocks the receptors that normally maintain venous and arterial tone. When a patient stands, the inability of the blood vessels to constrict (due to alpha-1 blockade) causes blood to pool in the lower extremities, leading to a precipitous drop in blood pressure (orthostatic/postural hypotension).
- Cannot be predicted from the pharmacology of the drug.
- Not dose-dependent.
- Host-dependent factors (like genetics or immunological state) are important in predisposition.
- Penicillin → Anaphylaxis: The beta-lactam ring of penicillin can act as a hapten, binding to host proteins and triggering an unpredictable, massive IgE-mediated mast cell degranulation (Type I hypersensitivity) in susceptible individuals, leading to anaphylactic shock.
- Anticonvulsants → Hypersensitivity: Drugs like Phenytoin or Carbamazepine can cause unpredictable immune-mediated reactions such as Stevens-Johnson Syndrome (SJS), Toxic Epidermal Necrolysis (TEN), or DRESS syndrome. This is often linked to specific HLA genotypes (e.g., HLA-B*1502) affecting how the host metabolizes toxic arene oxide intermediates.
- Biological characteristics can be predicted from the chemical structure of the drug or its metabolite.
- Paracetamol (Acetaminophen) → Hepatotoxicity: Paracetamol is normally metabolized by glucuronidation and sulfation. However, a minor pathway via CYP450 enzymes produces a highly toxic, highly reactive intermediate metabolite called NAPQI (N-acetyl-p-benzoquinone imine). In overdose, glutathione stores are depleted, and NAPQI covalently binds to hepatic cellular proteins, causing predictable centrilobular hepatic necrosis.
- Occur after many years of treatment or post-exposure.
- Can be due to drug or metabolite accumulation.
- Chemotherapy → Secondary tumours: Alkylating agents (e.g., Cyclophosphamide) directly cross-link and damage DNA. While they kill primary cancer cells, the cumulative genetic mutations in healthy stem cells can lead to secondary malignancies, such as leukemia, emerging years later.
- Phenytoin during pregnancy → Teratogenic effects: Exposure in utero can lead to "Fetal Hydantoin Syndrome," characterized by craniofacial anomalies (cleft lip/palate), hypoplastic nails, and developmental delays, manifesting as the child grows.
- Antipsychotics → Tardive dyskinesia: Long-term use of typical antipsychotics (e.g., Haloperidol) causes chronic blockade of dopamine (D2) receptors in the nigrostriatal pathway. Over years, this leads to an unpredictable up-regulation and hypersensitivity of these receptors, resulting in delayed, involuntary, repetitive body movements.
- Analgesics → Nephropathy: Chronic, long-term use of NSAIDs inhibits vasodilatory prostaglandins in the kidneys, leading to chronic renal ischemia, papillary necrosis, and chronic interstitial nephritis ("analgesic nephropathy") over years of accumulated use.
- Occur on withdrawal, especially when a drug is stopped abruptly.
- Phenytoin withdrawal → Seizures: Abrupt cessation of an anticonvulsant removes the pharmacological suppression of neuronal firing. The central nervous system experiences "rebound excitability," which can precipitate severe withdrawal seizures or status epilepticus.
- Steroid withdrawal → Adrenocortical insufficiency: Exogenous corticosteroids (e.g., Prednisone) exert negative feedback on the Hypothalamic-Pituitary-Adrenal (HPA) axis, shutting down endogenous cortisol production. If stopped abruptly, the atrophied adrenal glands cannot produce enough cortisol to meet physiological demands, leading to a life-threatening acute adrenal crisis.
- Unwanted but often unavoidable, pharmacodynamic effects that occur at therapeutic doses.
- Predicted from the pharmacological profile of a drug.
- Known to occur in a given percentage of drug recipients.
- Atropine (preanaesthetic) → Dryness of mouth: Atropine is a muscarinic acetylcholine receptor antagonist used to reduce airway secretions during surgery. Because it systemically blocks muscarinic receptors, it unavoidably blocks M3 receptors in the salivary glands, causing a dry mouth.
- Acetazolamide (diuretic) → Acidosis: A carbonic anhydrase inhibitor that forces the renal excretion of bicarbonate to induce diuresis. The loss of the body's primary buffer (bicarbonate) naturally leads to a mild metabolic acidosis.
- Promethazine (anti-allergic) → Sedation: It is a first-generation H1 receptor antagonist intended to block peripheral histamine to stop allergies. However, it is highly lipophilic, crosses the blood-brain barrier, and blocks central H1 receptors, leading to significant sedation.
- Estrogen (Anti-ovulatory / Contraceptive) → Nausea: Estrogen acts centrally on the chemoreceptor trigger zone (CTZ) in the brainstem and can irritate the gastric lining, causing a high incidence of nausea as a side effect.
- Codeine (anti-tussive) → Constipation → Used in Traveller's diarrhea: Codeine acts on mu-opioid receptors. In the medullary cough center, it stops coughing. In the GI tract, it decreases peristalsis. While constipation is an unwanted side effect when treating a cough, this exact pharmacodynamic effect is therapeutically exploited to treat diarrhea.
Occasionally, "adverse" effects may be exploited to develop an entirely new indication for a drug.
- Minoxidil: Originally developed as a potent potassium-channel-opening vasodilator for severely hypertensive patients. An unwanted side effect was hypertrichosis (hair growth). It was subsequently developed as a topical treatment for alopecia.
- Sildenafil: Initially developed as an antianginal medication to dilate coronary arteries. Its pronounced effect on alleviating erectile dysfunction (by inhibiting PDE-5 and increasing cGMP in the corpus cavernosum) led to a new drug indication.
- Sulfonamides: Used as antibacterials, they were found to produce hypoglycemia and acidosis as side effects. This led directly to the development of Hypoglycemic Sulfonylureas (for diabetes) and the Carbonic Anhydrase inhibitor Acetazolamide (for glaucoma/diuresis).
Indirect consequences of a primary action of the drug.
- Tetracyclines → Suppression of bacterial flora → Superinfections: These broad-spectrum antibiotics kill normal, healthy gastrointestinal and vaginal flora. This secondary disruption allows opportunistic, resistant pathogens (like Candida albicans or Clostridium difficile) to overgrow, causing superinfections.
- Corticosteroids → Weaken host defence → Activation of latent tuberculosis: Steroids profoundly suppress cell-mediated immunity (T-cells and macrophages). This indirect effect allows dormant granulomas containing Mycobacterium tuberculosis to break open and reactivate.
Result of excessive pharmacological action of the drug due to over dosage or prolonged use. Overdosage may be:
- 1. Absolute: Accidental, homicidal, or suicidal ingestion of a massive dose.
- 2. Relative: Normal dose given to a patient with impaired clearance (e.g., Gentamycin in a patient with Renal failure, leading to toxic accumulation and ototoxicity/nephrotoxicity).
- Extension of therapeutic effect:
- Barbiturates → Coma: (Over-facilitation of GABA-A receptors depressing the entire CNS).
- Digoxin → Complete A-V block: (Excessive vagal tone and Na/K ATPase inhibition completely stopping atrioventricular conduction).
- Heparin → Bleeding: (Excessive anticoagulation).
- Functional alteration:
- Atropine → Delirium: (Excessive central anticholinergic toxicity leads to hallucinations and delirium, independent of its intended peripheral effects).
- Drug induced tissue damage:
- Paracetamol → Hepatic necrosis: (Via toxic NAPQI metabolite).
- Appearance of characteristic toxic effects of a drug in an individual at therapeutic doses.
- It is the converse of tolerance and indicates a very low threshold of the individual to the drug's normal actions.
- Triflupromazine (single dose) → Muscular dystonias in some individuals (acute extrapyramidal symptoms from standard D2 blockade).
- Carbamazepine (few doses) → Ataxia in some individuals (excessive sodium channel blockade in the cerebellum at low doses).
- Chloroquine (single tablet) → Vomiting and abdominal pain in some individuals.
- Genetically determined abnormal reactivity to a chemical.
- Certain bizarre drug effects due to peculiarities of an individual for which no definite genotype has been described are also included.
- The drug interacts with some unique feature of the individual, not found in the majority of subjects, and produces an uncharacteristic reaction.
- Barbiturates → Excitement and mental confusion in some individuals (paradoxical reaction).
- Quinine → Cramps, diarrhea, asthma, vascular collapse in some individuals (severe idiosyncratic reaction known as Cinchonism).
- Chloramphenicol → Aplastic anemia in rare individuals (idiosyncratic, non-dose-dependent bone marrow failure due to genetic susceptibility affecting mitochondrial protein synthesis).
Immunologically mediated reaction producing stereotype symptoms, unrelated to the pharmacodynamic profile of the drug. Generally occurs even with much smaller doses.
- Type I: Immediate, anaphylactic (IgE-mediated)
- Penicillins → Anaphylaxis
- Type II: Cytotoxic antibody (IgG, IgM-mediated)
- Methyldopa → Hemolytic anemia (Drug binds to RBC membrane; IgG antibodies attack and destroy the red blood cells).
- Type III: Serum sickness (IgG, IgM Antigen-antibody complex)
- Procainamide-induced lupus (Complexes of drug and antibodies deposit in tissues and joints, causing systemic lupus erythematosus-like symptoms).
- Note: Types I, II, and III constitute Humoral immunity.
- Type IV: Delayed hypersensitivity (T cell-mediated)
- Contact dermatitis (Topical drug exposure activates localized T-cells leading to delayed skin inflammation).
- Note: Type IV constitutes Cell-mediated immunity.
Cutaneous reaction resulting from drug-induced sensitization of the skin to UV radiation. The reactions are of two types:
- Phototoxic: Drug or its metabolite accumulates in the skin, absorbs light, and undergoes a photochemical reaction resulting in local tissue damage (sunburn-like, i.e., erythema, edema, blistering, hyperpigmentation).
- Tetracyclines (esp. Demeclocycline), Tar products, Nalidixic acid, Fluoroquinolones, Sulfones, etc.
- Photo allergic: Drug or its metabolite induces a cell-mediated immune response which on exposure to light (longer wave length) produces a papular or eczematous contact dermatitis-like picture.
- Sulfonamides, Sulfonylureas, Griseofulvin, Chloroquine, Chlorpromazine.
Drugs capable of altering mood and feelings are liable to repetitive use to derive euphoria, withdrawal from reality, social adjustment, etc.
- Psychological dependence: Individual believes that optimal state of well being is achieved only through the actions of the drug. (e.g., Opioids, Cocaine).
- Physical dependence: Altered physiological state produced by repeated administration of a drug which necessitates the continued presence of the drug to maintain physiological equilibrium. Discontinuation of the drug results in a characteristic withdrawal (abstinence) syndrome. (e.g., Opioids, Barbiturates, Alcohol, Benzodiazepines).
- Drug abuse: Use of a drug by self medication in a manner and amount, that deviates from the approved medical and social patterns in a given culture at a given time. Refers to any use of an illicit drug.
- Drug addiction: Compulsive drug use characterized by overwhelming involvement with the use of a drug.
- Drug habituation: Less intensive involvement with the drug, withdrawal produces only mild discomfort.
- Habituation and addiction imply different degrees of psychological dependence.
Sudden interruption of therapy with certain drugs result in adverse consequences, mostly in the form of worsening of the clinical condition for which the drug was being used.
- Corticosteroid → Adrenal insufficiency
- β-blockers → Worsening of angina, precipitation of Myocardial Infarction (MI) (Due to up-regulation of beta receptors during chronic blockade; abrupt withdrawal leaves the heart hypersensitive to endogenous catecholamines).
- Clonidine → Severe HTN, restlessness, sympathetic over activity (Alpha-2 agonist withdrawal removes central sympathetic inhibition, causing a massive rebound catecholamine release).
Capacity of a drug to cause foetal abnormalities when administered to the pregnant mother. Drugs can affect the foetus at 3 stages:
- Fertilization and implantation (Conception to 17 days): Failure of pregnancy which often goes unnoticed (all-or-nothing effect).
- Organogenesis (18 days to 55 days): Most vulnerable period, major structural deformities are produced.
- Growth and development (> 56 days): Developmental and functional abnormalities can occur.
- Thalidomide → Phocomelia, multiple defects (Thalidomide acts as an angiogenesis inhibitor, preventing proper blood vessel formation required for limb bud development in the fetus).
- Anticancer drugs → Cleft palate, hydrocephalus, multiple defects (Directly disrupts DNA synthesis and rapid cell division in the developing embryo).
- ACE inhibitors → Hypoplasia of organs (lungs, kidney) (Blocks the fetal renin-angiotensin system, causing severe fetal hypotension, renal failure, and oligohydramnios, which restricts lung development).
Capacity of a drug to cause genetic defects and cancer respectively. Chemical carcinogenesis generally takes several (10-40) years to develop.
- Anticancer drugs (Direct DNA damage/alkylation).
- Radio-isotypes (Radiation-induced chromosomal breaks).
- Estrogens (Proliferative stimuli on hormone-sensitive tissues like endometrium/breast).
- Tobacco (Contains numerous chemical carcinogens like benzopyrenes).
Also called Iatrogenic (Physician induced) diseases. Functional disturbances caused by drugs which persist even after the offending drug has been withdrawn and largely eliminated.
- Salicylates (Aspirin), Corticosteroids → Peptic ulcer (Aspirin inhibits COX-1, depleting protective gastric prostaglandins. Corticosteroids decrease gastric mucosal cell renewal).
- Phenothiazines, other antipsychotics → Parkinsonism (Chronic dopamine D2 receptor blockade in the basal ganglia mimics the pathology of Parkinson's disease).
- Isoniazid → Hepatitis (Metabolized into toxic hydrazine metabolites that damage hepatocytes).
- Hydralazine → DLE (Discoid / Drug-induced Lupus Erythematosus) (Alters host proteins in slow acetylators, triggering an autoimmune antibody response against the host's own DNA).
- Adverse Drug Reactions (ADRs) are adverse events with a causal link to a drug.
- Types of Classification of ADRs:
- Onset of event: Acute (<60 minutes), Sub-acute (1-24 hrs) and Latent (>2 days).
- Type of reaction: Type A (Augmented), B (Bizarre), C (Chemical), D (Delayed), E (Exit), F (Familial), G (Genotoxicity), H (Hypersensitivity), U (Unclassified).
- Severity: Minor, Moderate, Severe, Lethal ADRs.
- Others: Side effects, Secondary effects, Toxic effects, Intolerance, Idiosyncrasy, Drug allergy, Photosensitivity, Drug Dependence, Drug Withdrawal Reactions, Teratogenicity, Mutagenicity, Carcinogenicity, Drug induced disease (Iatrogenic).
- Bhushanam T., V. (n.d.). Adverse Drug Reactions [PDF Presentation slides].
- Brunton, L. L., Hilal-Dandan, R., & Knollmann, B. C. (2017). Goodman & Gilman's The Pharmacological Basis of Therapeutics (13th ed.). McGraw-Hill Education. (Used for pharmacological expansions).
- Katzung, B. G. (2017). Basic & Clinical Pharmacology (14th ed.). McGraw-Hill Education. (Used for pharmacological expansions).
- World Health Organization (WHO). (2002). Safety of Medicines: A guide to detecting and reporting adverse drug reactions. WHO Press.
Quick Quiz
Table of Contents
ToggleAdverse Reactions Quiz
Pharmacology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Adverse Reactions Quiz
Pharmacology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.