
Diarrhoea is the passage of more than three loose or liquid stools in 24 hours. It is important to understand that diarrhoea is a symptom, not a disease itself. It is the body's natural defence mechanism to flush out harmful germs, toxins, or irritants from the gastrointestinal tract.
- Their immune systems are still developing.
- They have not yet built immunity to many common germs.
- They explore their environment by putting things in their mouths (hand-to-mouth stage).
- Their gut microbiome is still maturing.
Most episodes of acute diarrhoea last a few days to one week. Diarrhoea is often accompanied by:
- Fever: The body's systemic response to fighting infection.
- Nausea and vomiting: Due to stomach irritation (gastroenteritis).
- Abdominal cramps: Gut muscles contracting violently (hypermotility) to push out contents.
- Dehydration: The most dangerous complication, caused by the loss of too much water and vital electrolytes (sodium, potassium).
To truly understand diarrhoea, you must know the two main mechanisms:
- Secretory Diarrhoea: Toxins (like from Cholera or E. coli) force the gut cells to actively pump chloride and water into the gut lumen. The gut is "weeping" fluid.
- Osmotic Diarrhoea: Viruses (like Rotavirus) destroy the tips of the gut villi. The child cannot absorb nutrients (like lactose). These unabsorbed nutrients stay in the gut and act like a sponge, pulling water out of the body and into the stool.
These are the most common causes of diarrhoea in children.
- Rotavirus: The leading cause of severe diarrhoea in infants and young children worldwide. It is highly contagious and spreads through the faecal-oral route (contaminated hands, surfaces, food, or water). It causes watery diarrhoea, vomiting, and fever, and can lead to severe dehydration. (Prevention note: The Rotarix vaccine given at 6 and 10 weeks has drastically reduced these numbers in Uganda).
- Norovirus: Often called the "winter vomiting bug." It spreads rapidly in crowded places like schools and hospitals. Causes sudden onset of vomiting and diarrhoea.
- Adenovirus: Another common viral cause, particularly in children under 2 years.
Remember the acronym "RNA":
Rotavirus
Norovirus
Adenovirus
Bacteria cause diarrhoea by invading the gut lining (causing inflammation and bleeding) or by producing toxins that force the gut to secrete water.
| Bacteria | Key Features & Pathophysiology |
|---|---|
| Salmonella | Found in raw eggs, poultry, unpasteurised milk. Causes fever, abdominal pain, bloody diarrhoea. Invades the mucosa. |
| Shigella | Highly contagious; even a few bacteria can cause illness. Causes dysentery (bloody, mucoid stools with severe abdominal cramps). Secretes Shiga-toxin which causes severe mucosal ulceration. |
| Campylobacter | Most common bacterial cause worldwide. Found in undercooked poultry, unpasteurised milk. |
| E. coli | Several types: ETEC (traveller's diarrhoea, watery), EHEC (bloody diarrhoea, can cause kidney failure), EIEC (dysentery-like). |
| Staphylococcus aureus | Produces pre-formed toxins in contaminated food (cream pastries, mayonnaise). Causes rapid-onset vomiting and diarrhoea within 2-6 hours. |
| Parasite | Key Features |
|---|---|
| Giardia lamblia | Found in contaminated water. Causes chronic, foul-smelling, greasy diarrhoea (steatorrhea) with bloating and malabsorption. Common in areas with poor water sanitation. (It coats the intestinal wall, preventing fat absorption). |
| Cryptosporidium | Resistant to chlorine; outbreaks occur in swimming pools. Causes watery diarrhoea, especially in immunocompromised children (e.g., HIV+ children). |
| Entamoeba histolytica | Causes amoebic dysentery (bloody diarrhoea with abdominal pain). (Treated with Metronidazole). |
These are systemic infections where the germ is not in the gut, but the body responds with diarrhoea as part of the illness.
| Condition | Why It Causes Diarrhoea |
|---|---|
| Malaria | Toxins from parasites affect the gut; high fever increases gut motility. |
| Pneumonia | Systemic inflammation; swallowed respiratory secretions (mucus) irritate the gut; antibiotics used for treatment disrupt gut flora. |
| Measles | Virus directly damages gut lining; severe immune suppression allows secondary gut infections. |
| Septicaemia | Blood infection. Toxins circulate systemically and affect gut function and blood flow. |
| Otitis media | Ear infection. Swallowed pus from ear drainage; antibiotics used for treatment. |
| UTI | Urinary tract infection. Systemic inflammatory response; antibiotics. |
| Meningitis | Systemic toxins; reduced gut blood flow. |
Exclusive breastfeeding is recommended for the first 6 months of life. Early weaning (starting solids before 6 months) causes diarrhoea because:
- The infant's gut is immature – digestive enzymes are not fully developed to handle complex foods.
- The gut lining is permeable – allowing undigested proteins to pass through, causing irritation and allergies.
- Poor hygiene during food preparation leads to contamination.
- Bottle feeding is particularly risky because bottles are notoriously difficult to clean properly, and bacteria multiply rapidly in leftover milk trapped in the teat.
Peak age: 6 to 18 months – when most mothers start weaning and children begin crawling and exploring.
- A. Malnutrition: Kwashiorkor (protein deficiency) and Marasmus (severe calorie deficiency) both cause severe atrophy (shrinking) of the gut lining. This leads to malabsorption diarrhoea – a vicious cycle where diarrhoea worsens malnutrition, and malnutrition worsens diarrhoea.
- B. Indigestible Foods: Foods like sorghum, maize, and fibrous vegetables are difficult for young children to digest. Herbs and traditional remedies given to infants can severely irritate the delicate gut lining.
| Medication | Mechanism |
|---|---|
| Laxatives | Deliberately increase bowel movements (often given accidentally or inappropriately). |
| Antibiotics | Kill beneficial gut bacteria (normal flora), allowing harmful, resistant bacteria (like Clostridium difficile) to overgrow and secrete toxins. |
| Iron supplements | Can cause gastric irritation and loose, dark/black stools in some children. |
- Caused by toxins produced by bacteria in contaminated food (not the live bacteria invading the gut).
- Rapid onset: Usually within 2-6 hours of eating.
- Symptoms: Sudden vomiting, diarrhoea, sometimes fever. Usually resolves within 24 hours as the body naturally clears the toxin.
- Common sources: Reheated rice (Bacillus cereus), undercooked meat, contaminated salads.
| Condition | Description |
|---|---|
| Irritable Bowel Syndrome (IBS) | Functional gut disorder; abdominal pain relieved by defecation; alternating constipation and diarrhoea. |
| Crohn's Disease | Chronic inflammation of any part of the gut; causes diarrhoea, weight loss, abdominal pain, blood in stool. |
| Food Allergies | Immune reaction to proteins (e.g., cow's milk protein allergy); causes diarrhoea, vomiting, eczema, blood in stool. |
| Celiac Disease | Autoimmune reaction to gluten (wheat, barley, rye); damages small intestine villi, causing severe malabsorption, bloating, and chronic diarrhoea. |
In many Ugandan communities, certain deeply rooted beliefs exist about diarrhoea causes. As nurses, we must respectfully educate while understanding these beliefs:
| Belief | Reality / Nursing Education Point |
|---|---|
| Breastfeeding while pregnant causes diarrhoea | Not true. However, pregnant mothers may have reduced milk supply, leading to the introduction of contaminated supplemental feeds. Ensure proper hygiene and adequate nutrition. |
| Teething causes diarrhoea | Teething does not directly cause diarrhoea. But during teething, children drool more, put dirty objects/fingers in their mouths to soothe the gums, and may start weaning – all of which introduce germs. |
| Crawling causes diarrhoea | Crawling itself does not cause diarrhoea. But crawling babies explore their environment, pick up dirty objects off the floor, and ingest germs (faecal-oral route). |
| "False Teeth" (Ebinyo) | A mythical condition where communities believe un-erupted canine teeth cause diarrhoea and fever. In reality, the child usually has a febrile illness like malaria or pneumonia that is causing the extra-intestinal diarrhoea. Dangerous practice: Traditional healers gouge out the tooth buds with unsterile instruments, leading to massive haemorrhage, septicaemia, and death. |
Nursing Role: Never dismiss cultural beliefs rudely. Explain the scientific cause while acknowledging the community's concerns to build trust.
| Assessment | What to Look For | What It Means |
|---|---|---|
| General condition | Lethargic, unconscious, restless, irritable | Indicates the severity of illness and neurological impact of dehydration. |
| Eyes | Sunken eyes | Classic sign of dehydration (loss of fluid from the fat pads behind the eyes). |
| Mouth and tongue | Dryness, stickiness, coated tongue | Reflects intracellular dehydration; poor oral intake. |
| Skin pinch (turgor test) | Pinch skin on abdomen – does it spring back slowly? | Poor skin turgor = significant loss of interstitial fluid. |
| Thirst/Drinking | Not able to drink, drinking poorly, drinking eagerly | Eager = Moderate dehydration. Unable to drink = Severe dehydration (Emergency). |
| Urine output | Decreased or absent urine (anuria) | Severe dehydration; the kidneys are shutting down to conserve water. |
| Anterior Fontanelle | Sunken fontanelle (soft spot on head in infants < 18 months) | A highly reliable sign of moderate to severe dehydration in babies. |
- Locate the skin on the child's abdomen (side of the belly, halfway between umbilicus and flank).
- Pinch the skin and subcutaneous fat between your thumb and forefinger for 1-2 seconds.
- Release and observe how quickly it returns to normal.
- Immediate return (<2 seconds): Normal hydration.
- Slow return (2+ seconds): Some dehydration.
- Very slow return (>5 seconds): Severe dehydration.
| Classification | Signs (Look for TWO or more of the following) | Severity & Action |
|---|---|---|
| NO DEHYDRATION | Not enough signs to classify as some or severe dehydration. | Mild – can be managed at home (Plan A). |
| SOME DEHYDRATION | Two or more of: 1. Restless / irritable 2. Sunken eyes 3. Drinks eagerly / thirsty 4. Skin pinch goes back slowly |
Moderate – needs ORS in clinic (Plan B). |
| SEVERE DEHYDRATION | Two or more of: 1. Lethargic / unconscious 2. Sunken eyes 3. Not able to drink or drinking poorly 4. Skin pinch goes back very slowly |
EMERGENCY – needs immediate IV fluids (Plan C). |
Goal: Prevent dehydration and treat at home.
| Action | Details |
|---|---|
| Extra fluids | Give more fluids than usual to replace what is lost. Use ORS, clean water, breast milk, diluted fresh fruit juice, or cereal porridge. |
| Zinc supplements | Give for 10-14 days. (Physiology: Zinc repairs the damaged gut epithelium, reduces severity and duration of the current episode, and prevents future episodes for up to 3 months). |
| Continue breastfeeding | Breast milk is the best fluid – it provides nutrition, antibodies, and perfectly balanced water. |
| Continue feeding | Do not stop regular foods. Give small, frequent, highly nutritious meals to prevent malnutrition. |
| Home-made ORS (SSS) | Teach mothers: 6 level teaspoons of sugar + ½ level teaspoon of salt dissolved in 1 litre of clean, boiled water. |
| Hygiene education | Handwashing, safe water storage, proper food handling, safe disposal of child's stool. |
| When to return | Teach danger signs: blood in stool, persistent vomiting, fever, worsening condition, child not drinking/feeding. |
1. Give extra fluid (as much as the child will take).
2. Continue feeding (never starve a child with diarrhoea; the gut needs food to heal).
3. Know when to return (recognize the danger signs).
Goal: Rehydrate with ORS over 4 hours in a health facility.
You cannot just give plain water to a severely dehydrated child; it won't be absorbed fast enough. ORS contains exact ratios of Sodium and Glucose. In the gut wall, there is a special pump called the SGLT-1 (Sodium-Glucose Linked Transporter). This pump ONLY works if it grabs one molecule of sodium and one molecule of glucose at the exact same time. When it pulls them into the blood, water follows rapidly by osmosis! This is why adding sugar to salt water saves lives.
| Weight | Age | Amount of ORS in 4 Hours |
|---|---|---|
| < 5 kg | < 4 months | 200–400 ml |
| 5–< 8 kg | 4–< 12 months | 400–600 ml |
| 8–< 11 kg | 12 months–< 2 years | 600–800 ml |
| 11–< 16 kg | 2–< 5 years | 800–1200 ml |
| 16–30 kg | 5–15 years | 1200–2200 ml |
- If the child wants more ORS than the calculated volume, give more.
- For infants under 6 months who are not breastfeeding, also give 100–200 ml of clean water to prevent hypernatremia.
- Give frequent small sips from a cup or spoon (do not use bottles).
- If the child vomits, wait 10 minutes, then continue more slowly.
- Continue breastfeeding whenever the child wants.
- Reassess the child using LOOK and FEEL.
- Reclassify dehydration status.
- Choose Plan A (if resolved), Plan B (if still some dehydration), or Plan C (if worsened) accordingly.
- If child is 6 months or older, give freshly prepared foods.
- Cereal or starchy food mixed with pulses, vegetables, meat/fish.
- Add 1–2 teaspoons of vegetable oil to each serving (for dense calories).
- Fresh fruit juice or mashed banana (to replenish lost potassium).
- Offer food at least 6 times a day.
- After diarrhoea stops, give an extra meal a day for 2 weeks to catch up on lost nutrition.
⚠️ THIS IS A MEDICAL EMERGENCY
- Start IV fluids IMMEDIATELY.
- If no IV access can be secured, pass a nasogastric tube (NGT) and give ORS at 20ml/kg/hr, or consider intraosseous (IO) access.
- Transfer to hospital URGENTLY if at a lower-level clinic.
- Encourage mother to continue giving ORS by mouth during transport if the child can drink.
| Age | First Give (Rapid Volume Expansion) | Then Give (Deficit Replacement) |
|---|---|---|
| Infants under 12 months | 30 ml/kg in 1 hour | 70 ml/kg in 5 hours |
| Children 12 months to 5 years | 30 ml/kg in 30 minutes | 70 ml/kg in 2.5 hours |
- Reassess every 1–2 hours. Check radial pulse, consciousness, and breathing.
- If hydration status is not improving, increase the IV drip rate.
- Give ORS by mouth (5 ml/kg/hour) as soon as child can drink safely without choking – usually after 3–4 hours for infants, or 1–2 hours for older children.
- Reassess completely after 6 hours (infants) or 3 hours (children). Reclassify and choose appropriate plan (A, B, or C).
- Monitor vital signs every 15 minutes until a strong pulse is present.
- Investigations: Stool microscopy and culture, blood slide for malaria.
- Administer antibiotics only if bacterial infection (like bloody dysentery or cholera) is suspected or confirmed.
- Maintain nutrition: Start feeding as soon as child is stable and can eat safely.
- Infection control: Disinfect surfaces, isolate if highly infectious (e.g., Cholera/Rotavirus).
| Strategy | Explanation / Rationale |
|---|---|
| Exclusive breastfeeding for 6 months | Protects against infections; provides maternal IgA antibodies directly to the gut; inherently clean and safe from water contamination. |
| Discourage bottle feeding | Bottles are notoriously hard to clean; bacteria grow in the rubber teats and leftover milk. Use cups and spoons instead. |
| Boiled drinking water | Boiling kills bacterial, viral, and parasitic germs; makes water safe for preparing feeds and drinking. |
| Proper food storage | Cooked food should be eaten within 2 hours or refrigerated to prevent toxin-producing bacteria (like Staph aureus or Bacillus cereus) from multiplying. |
| Hand hygiene | Wash hands with soap and water at 5 critical times: after using toilet, after cleaning a child's bottom/stool, before eating, before feeding a child, and before preparing food. |
| Proper waste disposal | Use latrines. Prevents flies from carrying faeces to food, and prevents contamination of community water sources. |
| Prevent malnutrition | Well-nourished children have intact gut linings and stronger immune systems to fight off invading pathogens. |
| Immunization | Ensure the child receives the Rotavirus vaccine (at 6 and 10 weeks in Uganda) and the Measles vaccine (at 9 months) which protect against diseases that heavily feature diarrhoea. |
Case: A 2-year-old child weighing 12 kg is brought to the clinic. The mother states the child has had 6 watery stools today. On assessment, the child is irritable, has sunken eyes, and drinks ORS eagerly from a cup. The skin pinch goes back slowly (in 2 seconds).
- What is the WHO classification of dehydration?
- What Treatment Plan will you use?
- How much ORS will you administer in the first 4 hours?
Answers:
- Some Dehydration (Child has 3 signs: irritable, sunken eyes, drinks eagerly).
- Plan B.
- Looking at the table for a 12 kg, 2-year-old child: Give 800–1200 ml of ORS over 4 hours.
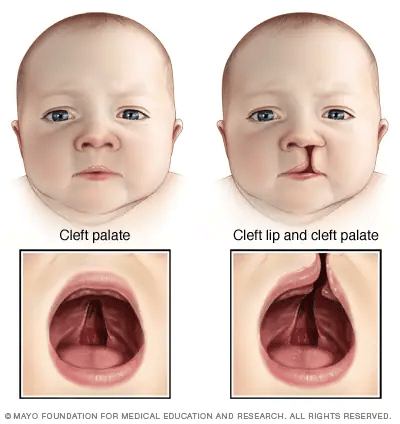
- Cleft Lip: A physical split or separation of the two sides of the upper lip. It appears as a gap or opening that may extend from the lip up to the base of the nose, and may involve the upper jaw bone and gum.
- Cleft Palate: A split in the roof of the mouth (the palate), which separates the mouth from the nose. It can involve the soft palate (back), hard palate (front), or both.
- Both conditions can occur on one side (unilateral) or both sides (bilateral).
During early pregnancy (weeks 4–7), the tissues that form the lip and palate fail to fuse together properly. There is not enough tissue, or the tissue does not join correctly. Specifically, the maxillary prominences fail to fuse with the medial nasal prominences. If this happens early (week 5-6), you get a cleft lip. If it happens slightly later (week 7-9) when the palatal shelves are supposed to zip together, you get a cleft palate.
| Cause | Explanation / Clinical Detail |
|---|---|
| Unknown (most cases) | No specific cause identified in the majority of cases (multifactorial). |
| Hereditary/Genetic | If one parent has a cleft, the risk is higher. If a sibling has a cleft, future children have an increased risk. Often associated with syndromes (e.g., Pierre Robin sequence). |
| Maternal medications | Anti-seizure drugs (phenytoin, valproate), methotrexate (for cancer/arthritis), some acne medications (isotretinoin) act as teratogens during the critical first trimester. |
| Maternal infections/illness | Viruses like rubella, or exposure to certain chemicals during pregnancy. |
| Nutritional deficiencies | Folic acid deficiency heavily increases the risk (just like with neural tube defects). |
| Environmental factors | Smoking, alcohol, radiation exposure during pregnancy restrict blood flow to the developing fetal face. |
- A. Feeding Problems: The palate normally seals the nasal cavity from the mouth during swallowing. With a cleft palate, milk and food can enter the nose. Babies cannot create suction on a regular nipple because air leaks through the cleft. This leads to poor intake, frustration, and inadequate nutrition.
- B. Hearing Loss: The Eustachian tube (connects middle ear to throat) does not function properly because the palatal muscles that normally pull it open are detached. Fluid builds up behind the eardrum (otitis media with effusion). This causes conductive hearing loss and recurrent ear infections. If untreated, can lead to permanent hearing damage.
- C. Dental Abnormalities: Small, missing, extra, or crooked teeth. Defects in the alveolar ridge (bone supporting teeth). Teeth may be displaced, rotated, or fail to erupt properly.
- D. Speech Difficulties: Air escapes through the nose instead of the mouth. Sounds like "p," "b," "t," "d," "k," "g" are difficult to produce (because they require building up pressure in the mouth). Speech may sound hypernasal (too much air through nose).
- E. Psychological Effects: Parents (especially mothers) may feel guilt, shame, or sadness. Older children may experience bullying or low self-esteem. Family support and counselling are essential.
| Aspect | Management & Physiology |
|---|---|
| Feeding | Minor cleft lip: may still suck. Combined cleft lip and palate: cannot suck effectively. Express breast milk and feed by cup, spoon, or special feeding bottle (e.g., Haberman feeder, Pigeon bottle - these have one-way valves so the baby only has to chew, not suck, to get milk). |
| Hygiene | Strict hygiene of feeding utensils to prevent diarrhoea and respiratory infections. Clean the cleft with sterile water after feeding to prevent crusting. |
| Artificial palate | In specialised units, a dental plate (obturator) may be fitted to help the baby suck until surgery. |
| Weight monitoring | Regular weighing until baby reaches 4.5 kg – minimum weight for safe surgery. |
| Surgery timing | Cleft lip: Repaired at 3–6 months. Cleft palate: Repaired at 12–18 months (bones need to be stronger; earlier repair may restrict mid-facial bone growth, but delaying too long hurts speech development). |
| Post-surgical care | Arm restraints (No-No's) to prevent baby touching sutures; soft diet; pain management; wound care (clean suture line with saline); monitor for bleeding or airway obstruction. |
| Multidisciplinary Follow-up | Speech therapy (after palate repair), regular audiology (hearing) checks, and orthodontic dental assessment as the child grows. |
Surgeons traditionally wait until the infant meets the "Rule of 10s" to ensure they can survive general anaesthesia safely:
- At least 10 weeks old
- At least 10 pounds in weight (approx 4.5 kg)
- At least 10 g/dL of Haemoglobin
Definition: Tongue tie is a congenital condition where the frenulum (the thin piece of skin connecting the underside of the tongue to the floor of the mouth) is unusually short, thick, or tight. This restricts tongue movement.
| Age Group | Problem | Explanation / Physiology |
|---|---|---|
| Newborns/Infants (Breastfeeding) | Cannot open mouth wide enough; slides off breast; poor milk transfer; causes severe maternal nipple pain/damage. | The tongue needs to lift and extend over the lower gum to grasp the breast and create a vacuum seal. A tied tongue cannot do this. |
| Bottle-fed infants | Cannot form seal around teat; milk leaks out; swallows excessive air. | Leads to severe colic, discomfort, and poor weight gain. |
| Older children | Speech difficulties (especially "l," "r," "t," "d," "th" sounds). Eating difficulties. | Tongue cannot reach the roof of the mouth or the upper teeth. Cannot efficiently move food to the back of the mouth for chewing. |
- Procedure: A quick, simple procedure where the frenulum is snipped with sterile scissors.
- Timing: Can be done in newborns (minimal pain, few nerve endings and blood vessels in the frenulum) or later if diagnosed late.
- Anaesthesia: Usually none needed in very young infants; local or general anaesthetic required for older children.
- Aftercare: Breastfeed immediately! This comforts the baby, acts as a natural analgesic, checks feeding improvement, and the sucking motion acts as gentle tongue exercises to prevent re-attachment.
- Frenuloplasty: More extensive surgical release if the frenulum is very thick or posterior – requires stitches.
- Oesophageal Atresia (OA): A congenital defect where the oesophagus (food pipe) does not form properly. The upper part ends in a blind pouch and does not connect to the stomach.
- Tracheo-Oesophageal Fistula (TOF): An abnormal connection (fistula) between the oesophagus and the trachea (windpipe). This means food and saliva can enter the lungs, or stomach acid can splash into the lungs.
During a normal pregnancy, the fetus swallows amniotic fluid, absorbs it in the gut, and urinates it back out. If the fetus has Oesophageal Atresia, it cannot swallow the fluid. Therefore, the fluid builds up excessively in the womb. A mother presenting with Polyhydramnios (too much amniotic fluid) on ultrasound is a massive red flag that the baby might have OA!
| Type | Description |
|---|---|
| Type A (8%) | Both upper and lower oesophagus end in blind pouches – NO TOF. |
| Type B (1%) | Upper pouch connects to trachea (dangerous aspiration immediately); lower pouch blind. |
| Type C (85%) | Upper pouch blind; lower pouch connects to trachea – MOST COMMON. (Air fills the stomach causing a bloated abdomen). |
| Type D (1%) | Both upper and lower pouches connect to trachea. |
| Type E (4%) | Oesophagus is intact but has a TOF (H-type fistula). Less obvious at birth, causes recurrent pneumonias later. |
- Excessive drooling: Saliva cannot pass to the stomach; it pools in the mouth and overflows.
- Coughing, choking, cyanosis (The 3 Cs) with the first feed: Milk enters the blind pouch and instantly overflows/spills into the trachea and lungs.
- Inability to pass nasogastric tube (NGT): Key Diagnostic Test! Attempt to pass a 10F catheter through the nose into the stomach. In OA, it will hit a wall and coil in the upper oesophageal pouch at 10–12 cm.
- Respiratory distress: Aspiration of saliva/milk into lungs.
- Scaphoid (sunken) abdomen OR Bloated abdomen: Scaphoid if Type A (no air reaches stomach). Bloated if Type C (every time the baby breathes, air goes through the fistula into the stomach).
- Pre-Operative Care:
- Suction upper pouch continuously: (Replogle tube) Prevents saliva aspiration into lungs.
- Nurse in semi-upright position (30–45°): Crucial for Type C! Keeps stomach acid from refluxing up the lower fistula into the lungs.
- NPO / IV fluids / Antibiotics / Warmth: Standard emergency neonatal prep.
- Gastrostomy: A surgical opening directly into the stomach may be placed early for feeding and to decompress the stomach air.
- Surgical Management: Primary repair (thoracotomy to join the two ends and tie off the fistula) if the gap is short. Staged repair if the gap is too wide.
- Complications: Aspiration pneumonia, Oesophageal stricture (scarring at surgical site causes narrowing/dysphagia), Tracheomalacia (weak tracheal cartilage causes a "honking" seal-like cough), recurrent fistula, severe Gastro-oesophageal reflux (GOR).
Definition: Pyloric stenosis is the narrowing of the pylorus (the muscular valve at the outlet of the stomach that opens into the duodenum). This is caused by hypertrophy (thickening) and hyperplasia of the pyloric circular muscle, which completely clamps down and prevents the stomach from emptying properly.
- Males are affected 4–5 times more than females (especially first-born males).
- The pyloric muscle thickens and elongates, severely narrowing the pyloric canal.
- The stomach must work extremely hard to push food through this tiny hole. This causes the stomach muscle itself to hypertrophy, leading to visible peristaltic waves across the baby's belly.
- Eventually, the stomach fails to push milk through. The stomach fills up, and the milk is violently vomited back up.
| Sign / Symptom | Explanation / Physiology |
|---|---|
| Projectile vomiting | Forceful ejection of stomach contents up to 1 metre away! Occurs shortly after feeding. It is non-bile-stained because the blockage is before the bile duct entry in the duodenum. |
| Hunger after vomiting | The "Hungry Vomiter". The stomach is completely empty, and the intestines haven't received any food, so the baby frantically wants to feed again immediately. |
| Weight loss & Constipation | Inadequate nutrition reaching the intestines. Little or no stool is produced because no food is getting through. |
| Dehydration | No tears when crying, dry mouth, sunken fontanelle, decreased urine output. |
| Visible peristaltic waves | Left-to-right wave seen across the upper abdomen as the stomach fights to contract against the blockage. |
| Palpable "olive" mass | The hugely thickened pylorus muscle can be felt physically; it feels exactly like a small, firm olive in the right upper quadrant or epigastrium. |
Question: Why do blood tests in Pyloric Stenosis show Hypochloraemic Hypokalaemic Metabolic Alkalosis?
Physiology Answer:
1. The baby vomits massive amounts of pure stomach acid (Hydrochloric Acid - HCl).
2. Losing H+ (acid) causes the blood to become alkaline (Metabolic Alkalosis). Losing Cl- causes Hypochloraemia.
3. Because the baby is vomiting, they become severely dehydrated. Dehydration causes blood pressure to drop, which triggers the kidneys to activate the RAAS system to save Sodium and Water.
4. In order to save Sodium, the kidneys are forced to pee out Potassium in exchange. This leads to severe Hypokalaemia (low potassium).
Conclusion: You MUST correct the electrolytes and hydration with IV fluids before you ever send this baby to surgery, or they will die of cardiac arrest on the operating table due to the low potassium.
- Diagnosis: Clinical exam (olive mass). Ultrasound is the Gold Standard – shows thickened pyloric muscle (>3–4 mm) and elongated pylorus (>14–16 mm). Barium meal X-ray shows the "String sign" (thin stream of barium squeezing through the narrowed pylorus).
- Pre-Op: NPO (Nil Per Os), NGT for gastric decompression. CRITICAL: Correct dehydration over 24-48 hours using Normal Saline with added Potassium. Never operate before correcting this!
- Surgical Management: Pyloromyotomy (Ramstedt's Procedure). A longitudinal incision is made strictly through the outer muscle layers of the pylorus, splitting it open like a hotdog bun, without cutting the inner mucosa. This widens the channel.
- Post-Op: Keep NPO until fully awake. After 6 hours, give 5ml of boiled water/glucose water. Gradually advance to breastmilk/formula. Expected outcome is excellent; baby goes home in a few days.
Definition: Imperforate anus is a congenital condition where the anus (opening for stool) is absent, narrowed, or misplaced. The rectum (last part of the large intestine) does not connect properly to the outside of the body. This is part of a spectrum of ARMs.
- Low lesions: The rectum descends fully through the pelvic floor muscles but ends just under the skin. May present as a tiny stenosis or a blind pouch where the anus should be.
- High lesions: The rectum ends high up in the pelvis, completely missing the sphincter muscles. It often forms an abnormal fistula to the bladder or urethra (in boys), or the vagina (in girls), causing stool to leak out of the genitals.
- Persistent cloaca: Most severe (only in females). The rectum, vagina, and urinary tract all fail to separate and join into a single common exit channel.
If a baby has an imperforate anus, you MUST urgently check them for other congenital defects, because these defects happen together during early embryology. Remember VACTERL:
V - Vertebral anomalies (spine defects, missing vertebrae)
A - Anal atresia (Imperforate Anus - ARM)
C - Cardiac (heart) defects (e.g., VSD, ASD)
T - Tracheo-Oesophageal fistula
E - Esophageal atresia
R - Renal (kidney) anomalies (missing or deformed kidneys)
L - Limb anomalies (e.g., missing radius bone in the arm)
- Physical examination at birth: The most crucial step. No anal opening; anal opening in wrong place; or only a small dimple where the anus should be.
- Passage of meconium: Meconium may pass through the urethra or vagina (indicating a high fistula), or not at all.
- "Wink" reflex test: Stroking the perianal skin should cause the hidden sphincter muscles to twitch (anal wink). If absent, it indicates a high lesion missing sphincter muscles.
- Invertogram X-ray: A classic test. A coin is taped to the baby's anal dimple. The baby is held upside down for 1–2 minutes so swallowed air rises to the very end of the rectum. The X-ray shows the distance between the trapped air in the rectum and the coin on the skin (determines high vs. low lesion).
- Renal ultrasound & Echocardiogram: Mandatory to rule out VACTERL anomalies.
- Immediate Mgmt: NPO, IV fluids, NGT decompression (to prevent bowel rupture from obstruction), and IV Antibiotics (critical if stool is leaking into the urinary tract).
- Surgical Mgmt for Low Lesions: Anoplasty – surgical creation of an anus in the correct position; usually done as a single immediate procedure.
- Surgical Mgmt for High Lesions: Requires 3 stages.
- 1. Colostomy on day 1 to save the baby's life and allow stool to exit the abdomen.
- 2. Definitive repair (PSARP) at 3–12 months to pull the rectum down through the center of the pelvic muscles.
- 3. Colostomy closure months later once the new anus has healed.
- Post-Op Care: Dilatation! After anoplasty, parents must dilate the new anus daily with graduated metal dilators (Hegar dilators) to prevent severe scar tissue stricture. Monitor bowel management (constipation and faecal incontinence are lifelong struggles for these children).
| Mnemonic | Meaning |
|---|---|
| "RICE" for diarrhoea causes | Rotavirus, Infections, Contaminated food/water, Environmental |
| "SOS" for dehydration signs | Sunken eyes, Offer drink (poorly), Skin pinch (slow) |
| "VACTERL" for ARM associations | Vertebral, Anal, Cardiac, Tracheo-Oesophageal, Esophageal, Renal, Limb |
| "Pyloric PS" | Projectile vomiting, Small "olive" mass, Male baby |
- Know the WHO dehydration classification perfectly – this is tested frequently.
- Understand ORS preparation (6 sugar, half salt in 1 Litre) and administration – practical exam favourite.
- Remember Plan A, B, and C – know exactly when to use each based on the "Look and Feel" signs.
- Pyloric stenosis – classic presentation: male, 2–6 weeks, projectile non-bilious vomiting, palpable "olive", metabolic alkalosis.
- Cleft palate feeding – cup/spoon feeding, Haberman bottles, upright position.
- Oesophageal atresia – Polyhydramnios in mother, 3 Cs (cough, choke, cyanosis), NGT coiling, continuous suction, surgical emergency.
- Imperforate anus – Always inspect the perineum at birth, watch for meconium in urine, check for associated VACTERL anomalies.