
Palliative care plays a role in modern healthcare systems, extending profound benefits to patients, families, and communities.
- Alleviation of Physical and Emotional Suffering: Through precise symptom management, palliative care ensures that patients do not endure unnecessary pain, nausea, or breathlessness, fundamentally improving their daily comfort.
- Enhanced Quality of Life: By focusing on the patient's immediate goals and comfort rather than purely curative measures, it maximizes the quality of the time a patient has remaining.
- Reduction of Healthcare Costs and Hospital Admissions: Effective palliative care provided at home or in hospice settings drastically reduces emergency room visits and intensive care unit (ICU) admissions, preventing the use of futile and expensive medical interventions.
- Comprehensive Family Support: It prevents caregiver burnout by offering respite, education, and emotional support. It also formally addresses the psychological toll on the family during illness and continues with structured bereavement support after death.
- Promotion of Patient Autonomy: Palliative care champions the patient’s right to make informed decisions about their own body, including Advance Care Planning, ensuring medical care aligns with their personal values and cultural beliefs.
- Prevention of Complicated Grief: By preparing families for the realities of the dying process and providing structured aftercare, palliative care reduces the incidence of severe, prolonged psychological trauma in surviving relatives (especially orphaned children).
- Affirms Life
- Says "YES" to, supports, confirms, celebrates. Palliative care says: "Your life still matters. You are still valuable."
- How nurses affirm life: Talk to the patient (not just about disease), ask about family/memories, celebrate small victories, treat them as a PERSON, and use their name.
- Regards Dying as a Normal Process
- Dying is a natural part of life, like birth. It is not a failure of medicine or a punishment from God.
- How nurses show this: Do not act afraid around dying patients, don't whisper, be honest, allow natural death, and support the family.
- Neither Hastens Nor Postpones Death
- Does NOT give medicine to kill the patient (euthanasia) OR give medicine to keep them alive at all costs (futile treatment).
- DOES focus on comfort, stops harmful treatments, and allows natural death. (Example: Removing a ventilator from a terminal patient suffering with no chance of recovery is NOT hastening death — it is stopping futile treatment.)
- Relieves Pain and Other Distressing Symptoms
- Addresses physical suffering (pain, nausea, constipation, dyspnea, fatigue, insomnia, etc.).
- How nurses relieve symptoms: Give medicine on time every time, use non-drug methods, assess regularly, and believe the patient!
- Integrates Psychological and Spiritual Aspects of Care
- Brings together mind, body, and spirit into ONE care plan.
- Example: Nurse gives morphine (physical) + listens to fears (psychological) + calls chaplain (spiritual). All three reduce the overall "total pain".
- Offers Support Systems for Patients to Live Actively Until Death
- Patients should not just lie in bed. They should make decisions, see family, enjoy hobbies, and feel useful.
- How nurses support active living: Ask "What would you like to do today?", help them sit up, encourage eating favorite foods.
- Offers Support Systems for Families During Illness and Bereavement
- During illness: Practical help (teaching care), emotional help, financial advice, respite care.
- During bereavement: Grief counseling, home visits, child support, memorial services.
Ethics are the rules of right and wrong in healthcare. The 4 main principles in Palliative Care are:
- A. Beneficence ("Do Good"): Always act in the patient's best interest. (e.g., Giving morphine to relieve pain).
- B. Non-maleficence ("Do No Harm"): Benefit must outweigh harm. (e.g., Morphine causes constipation, but the pain relief outweighs it. Treat the constipation!).
- C. Autonomy ("Patient's Right to Decide"): The patient can refuse treatment, choose where to die, and who visits. In Uganda, family dynamics are strong, but always ask the patient what they want first!
- D. Justice ("Fairness"): Treat all patients equally regardless of wealth, tribe, religion, gender, or disease.
Attributes are the CHARACTERISTICS or features that define something. Like ingredients in a recipe, without these attributes, care is just "general care," not palliative care.
- Treating the WHOLE person: Body (physical), Mind (psychological), Heart (emotional), Soul (spiritual), Social world, and Cultural identity.
- Example: Treating a 45-year-old mother with cervical cancer involves giving morphine (body), listening to fears (mind), paying school fees for kids (social), praying (soul), and respecting her wish to use a traditional healer (culture).
- Pain: Assess (0-10), use WHO ladder (Step 1 to Step 3), give BY THE CLOCK, prevent pain, manage side effects.
- Symptoms: Nausea (anti-emetics), Constipation (laxatives), Breathlessness (oxygen/morphine), Delirium (haloperidol), etc.
Talking clearly, listening, breaking bad news gently, and coordinating so that the doctor, nurse, pharmacist, social worker, and chaplain all know the plan and avoid duplication or gaps.
The patient is at the CENTER of everything. Care revolves around their goals, choices, and culture, not a "one-size-fits-all" hospital routine.
In Uganda, family provides food, bathing, turning, and meds. They suffer physical exhaustion, financial strain, and grief. Provide them education, respite, counseling, and practical help.
Unbroken care from diagnosis ➔ hospital ➔ home ➔ hospice ➔ home ➔ bereavement. No gaps where the patient is forgotten.
Planning for the future BEFORE it happens (where to die, what treatments to refuse, who makes decisions). In Uganda, this must be done gently respecting cultural norms.
Grief is normal. Palliative care provides immediate support at death, early bereavement (calls/visits), and ongoing support (support groups, checking on orphans). Watch for complicated grief (suicidal thoughts, inability to function for months).
Different professionals working TOGETHER (Doctors, Nurses, Social Workers, Chaplains, Pharmacists, Physios, Dietitians, Traditional Healers). Sharing information and making joint decisions.
Knock before entering, ask permission to touch, keep patient covered, use preferred names, don't talk as if they aren't there. At end of life: clean body, peaceful environment, respect rituals.
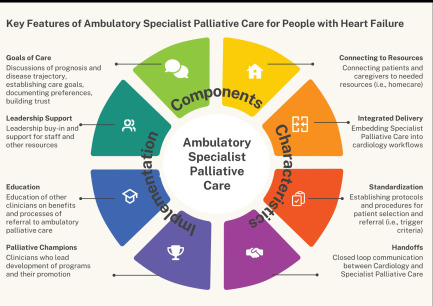
Palliative care has two components:
- Step 1: Mild Pain (Score 1-3)
- Medicines: Paracetamol (1g every 4-6h), Ibuprofen, Aspirin.
- Move to Step 2 if: Pain is not controlled after 24-48 hours.
- Step 2: Moderate Pain (Score 4-6)
- Medicines: Weak opioids like Codeine (30-60mg every 4-6h), Tramadol (50-100mg every 6-8h).
- Side effects: Constipation (ALWAYS give laxatives), Nausea, Drowsiness.
- Step 3: Severe Pain (Score 7-10)
- Medicine: Morphine (The gold standard). Oral liquid, tablets, or injections.
- Rules for Morphine: Start low (2.5-5mg every 4 hrs) and titrate up. NO maximum dose. Give BY THE CLOCK. Treat constipation and nausea. Give breakthrough doses.
- MYTH: "Morphine kills patients." TRUTH: When given correctly, it relieves pain and does NOT hasten death.
- MYTH: "Morphine causes addiction." TRUTH: Patients taking it for pain do NOT become addicted. They use it for relief, not to get "high".
- MYTH: "If you start, you can never stop." TRUTH: It can be tapered and stopped if pain improves.
- MYTH: "Save it for the very end." TRUTH: Start it immediately when pain is severe, regardless of life expectancy.
- Non-drug methods: Positioning, heat/cold, massage, distraction, relaxation.
- Adjuvants: Steroids (dexamethasone), Antidepressants (amitriptyline), Anticonvulsants (gabapentin).
| Symptom | Common Causes | Management |
|---|---|---|
| Nausea/Vomiting | Medicines, bowel obstruction, anxiety | Metoclopramide, haloperidol, ondansetron, small meals |
| Constipation | Morphine, immobility, dehydration | Laxatives (senna, bisacodyl), fluids, fiber |
| Breathlessness | Heart failure, lung disease, anxiety | Morphine, oxygen, positioning, fan, calm environment |
| Confusion/Delirium | Infection, dehydration, meds, brain mets | Haloperidol, treat cause, calm reorientation |
| Bedsores | Pressure, immobility, poor nutrition | Turn every 2 hours, wound care, keep skin dry |
Supportive care addresses psychological, social, spiritual, and cultural needs.
- Anxiety & Fear: Listen, provide calm environment, Diazepam if severe. Address fears of pain, dying alone, and the afterlife.
- Depression & Hopelessness: Counseling, Amitriptyline (helps pain/sleep too). Reframe hope to small goals.
- Anger: Do not take it personally. Acknowledge feelings ("I see you are angry. That is understandable.") Give choices to return control.
Address: Financial problems, poor housing, family conflicts, stigma/isolation, orphaned children, and legal issues (writing a will). Connect them to NGOs, legal aid, and community support.
- Not just religion—it's about meaning, purpose, forgiveness, and love.
- Assessment: "What gives your life meaning?" "Are you at peace?" (Do NOT impose your own beliefs).
- Support religious expression, address spiritual distress (feeling abandoned by God), and help them find realistic hopes.
Uganda has 50+ tribes. Culture affects how illness is understood (curse vs natural), who makes decisions, and burial customs. Work WITH traditional healers, respect diets, and learn local phrases.
Stages of Grief (Kubler-Ross):
- Denial ("The doctor is wrong.")
- Anger ("Why did God do this?")
- Bargaining ("If I pray, maybe God will bring him back.")
- Depression (Deep sadness, withdrawal.)
- Acceptance ("He is gone. I will miss him, but I can continue.")
Provide home visits, support groups, and special programs for orphans.
This is the MAIN goal. It is NOT about living as long as possible, but living as WELL as possible. Every nursing action should ask: "Does this improve their quality of life?"
Body + Mind + Heart + Soul + Social + Culture = WHOLE person.
Many disciplines working together through regular meetings, shared care plans, and clear communication.
They are in the MIDDLE. Care is planned WITH them, not FOR them. They are the experts on their own lives. (e.g., Compromising on turning a patient if they only feel comfortable on their right side).
Small details make a BIG difference. Noticing dry lips (apply balm), hot room (open window), exhaustion in family (arrange respite), or empty morphine bottles (order more early).
Palliative care cannot function without essential drugs, the most important being Morphine.
- Other essentials: Paracetamol, Haloperidol, Metoclopramide, Diazepam, Amitriptyline, Dexamethasone, Hyoscine, Laxatives.
- Nurses must advocate for these drugs, ensure safe storage, report stockouts, and educate prescribers.
- Peace: Inner calm, no fear.
- Comfort: Physical ease, no pain.
- Dignity: Respect, worth. Achieved by speaking softly, respecting privacy, honoring rituals, and allowing choices.
- World Health Organization (WHO). (2020). Palliative Care Fact Sheet. Geneva: WHO.
- African Palliative Care Association (APCA). (2018). Standards for Providing Quality Palliative Care across Africa. Kampala: APCA.
- Ministry of Health Uganda. (2021). National Palliative Care Policy and Clinical Guidelines. Kampala: Government of Uganda.
- Cherny, N., Fallon, M., Kaasa, S., Portenoy, R. K., & Currow, D. C. (Eds.). (2015). Oxford Textbook of Palliative Medicine (5th ed.). Oxford University Press.
- Kübler-Ross, E. (1969). On Death and Dying. Macmillan.
Quick Quiz
Roles and Attributes Quiz
Palliative Care - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Roles and Attributes Quiz
Palliative Care
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.