
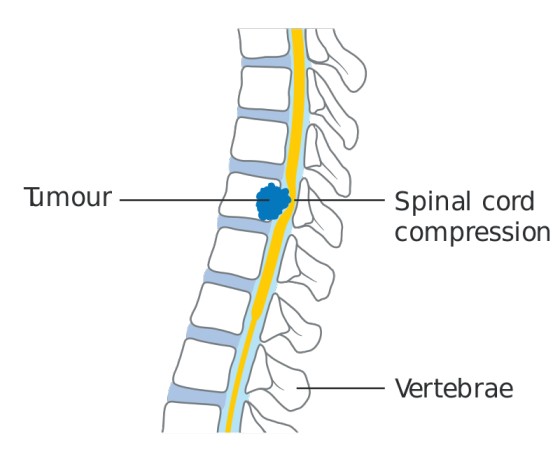
Spinal cord compression (SCC) is a medical emergency in which the spinal cord is compressed by an external mass, leading to neurological symptoms that can rapidly progress to permanent paralysis if not treated urgently.
In palliative care, SCC is one of the most feared emergencies because:
- It can steal a patient's remaining independence in hours or days.
- It causes severe, unrelenting pain.
- It leads to paralysis, loss of bladder and bowel control, and pressure sores.
- It transforms a mobile patient into a bedridden, fully dependent person.
- The window for effective treatment is narrow — permanent damage occurs if treatment is delayed.
| Reason | Explanation |
|---|---|
| Rapid progression | Symptoms can worsen from back pain to complete paralysis in days or even hours. |
| Permanent damage | Nerve tissue does not regenerate well. Paralysis may be irreversible after 24-48 hours. |
| Devastating impact on quality of life | A patient who was walking and toileting independently becomes bedridden, catheterized, and dependent. |
| Requires immediate, coordinated action | Steroids, radiotherapy, and analgesia must start urgently. Delays cause permanent harm. |
| Affects prognosis and care planning | The patient's remaining life changes dramatically. Goals of care must be re-discussed urgently. |
| Cause | Percentage | Explanation |
|---|---|---|
| Vertebral metastases invading the epidural space | 85-90% | Cancer spreads to the vertebrae (bones of the spine). The tumor grows backward into the epidural space (the area just outside the spinal cord) and squeezes the cord. |
| Paravertebral masses | 10% | Tumors or enlarged lymph nodes next to the spine press on the cord from the side. Common in lymphoma. |
SCC is frequently observed in advanced carcinoma, particularly:
| Cancer Type | Why It Causes SCC |
|---|---|
| Breast cancer | Common metastasis to spine; estrogen-sensitive tumors often spread to bone. |
| Lung cancer | Aggressive metastasis to vertebrae; often presents late. |
| Prostate cancer | Strong tendency to spread to bones, especially the spine. |
| Kidney cancer | Hypervascular tumors that metastasize to bone. |
| Lymphoma | Paravertebral lymph node masses compress the cord directly. |
| Myeloma | Cancer of plasma cells that destroys bone, including vertebrae. |
| Sarcoma | Bone and soft tissue tumors that invade the spine. |
In Uganda: Breast cancer, prostate cancer, and lymphoma are common causes. Kaposi's sarcoma and lymphoma related to HIV/AIDS can also cause SCC.
| Site | Percentage | Notes |
|---|---|---|
| Thoracic spine (middle back, T1-T12) | 70% | Most common site. Explains why patients often describe "band-like" chest pain. |
| Lumbar spine (lower back, L1-L5) | 20% | Below L2, compression affects the cauda equina (bundle of nerves), not the spinal cord itself. |
| Cervical spine (neck, C1-C7) | 10% | Can cause weakness in arms as well as legs. |
Important: In 20% of cases, compression occurs at more than one level simultaneously. Always suspect multiple sites if symptoms are widespread or confusing.
The cauda equina (Latin for "horse's tail") is the bundle of nerve roots that continues below the end of the spinal cord. Compression here causes:
- Saddle anesthesia (numbness in the area that would touch a saddle)
- Bladder and bowel dysfunction (urinary retention, incontinence, constipation)
- Leg weakness (often asymmetrical)
- Reduced reflexes
Prognostic note: Recovery is more likely after cauda equina lesions than after true spinal cord compression, because peripheral nerves regenerate better than spinal cord tissue.
SCC follows a predictable pattern if untreated:
BACK PAIN ➔ WEAKNESS ➔ SENSORY LOSS ➔ BLADDER/BOWEL DYSFUNCTION ➔ PARALYSIS
The earlier the intervention, the better the outcome. Once paralysis and loss of sphincter control occur, recovery is unlikely.
Back pain occurs in more than 90% of cases. It is typically the first symptom and the one that should raise suspicion.
| Characteristic of Pain | Description | What It Means |
|---|---|---|
| Bony pain | Deep, aching pain in the spine from vertebral metastases | Tumor is in the bone itself. |
| Radicular pain | Sharp, shooting pain following the path of a nerve root | Nerve root is being compressed. |
| Diffuse band-like pain | Pain that wraps around the chest or abdomen like a tight belt | Classic for thoracic SCC. The patient may say "It feels like someone is squeezing me with a belt." |
| Pain worsened by straining, coughing, or sneezing | Sudden increase in pain with Valsalva maneuvers | Increased pressure in the spinal canal worsens compression. |
Other pain descriptions:
- Sharp shooting pains down the legs
- Electric shock-like sensations (Lhermitte's sign) — indicates nerve irritation
- Unpleasant sensation below the level of compression — numbness, tingling, or "dead" feeling
| Sign | What to Look For | Significance |
|---|---|---|
| Tenderness over spine | Gentle percussion (tapping) of the vertebrae causes pain | Indicates vertebral involvement. Percuss one or two vertebrae above and below the suspected level. However, absence of tenderness does NOT rule out SCC. |
| Motor weakness | Patient cannot lift legs, push against resistance, or stand | Indicates cord compression is progressing. |
| Heavy or uncoordinated legs | Patient describes legs as "heavy," "like lead," or "clumsy" | Early sign of weakness before obvious paralysis. |
| Reduced muscle tone | Limbs feel floppy rather than stiff | Lower motor neuron sign; indicates nerve damage. |
| Decreased reflexes | Knee and ankle reflexes are reduced or absent | Early sign. Later, reflexes may become increased (upper motor neuron sign) as compression worsens. |
| Sensory loss with a level | Numbness below a specific line on the body (e.g., "I cannot feel anything below my waist") | Classic for SCC. The "level" corresponds to the site of compression. |
| Decreased rectal tone | Reduced anal sphincter tone on digital rectal exam | Indicates sacral nerve involvement. Bad prognostic sign. |
Any patient with advanced cancer and the following should be treated as SCC until proven otherwise:
| Red Flag | Action |
|---|---|
| Escalating back pain (rapidly increasing severity) | High suspicion of SCC. Start treatment immediately. |
| Back pain + heavy legs | Sufficient to consider treating for SCC even before full paralysis develops. |
| Back pain + weakness | Urgent assessment and treatment needed. |
| Back pain + urinary retention or incontinence | Cord compression is affecting sphincters. Very poor prognosis if delayed. |
| Back pain + constipation + overflow incontinence | Cauda equina or conus medullaris compression. |
| Band-like chest or abdominal pain | Classic thoracic SCC. |
| Feature | Detail |
|---|---|
| What it shows | Vertebral metastases, collapse, or destruction of vertebrae at the appropriate level. |
| Sensitivity | Positive in approximately 80% of cases. |
| Important limitation | A normal X-ray does NOT rule out SCC. Early compression or soft tissue masses may not be visible. |
Nursing implication: Do not wait for X-ray results to start treatment if clinical suspicion is high. Begin steroids and analgesia immediately.
| Feature | Detail |
|---|---|
| Status | Investigation of choice when available |
| What it shows | Detailed images of the spinal cord, vertebrae, epidural space, and surrounding tissues. Can identify compression level(s), tumor extent, and cord edema. |
| Advantage | Non-invasive; no radiation; can image multiple levels. |
In Uganda: MRI is available only in major referral hospitals (Mulago, Mbarara, etc.) and is expensive. Many patients cannot access it. Clinical judgment must guide treatment.
| Feature | Detail |
|---|---|
| CT scan | Can show bony destruction and some soft tissue masses. Less detailed than MRI for cord itself. |
| Myelogram | Contrast dye injected into the spinal canal; X-rays show compression. Invasive; risk of infection and headache. |
Nursing implication: If advanced imaging is unavailable (as is common in rural Uganda), do not delay treatment. Start steroids and analgesia based on clinical suspicion.
| Neurological Status Before Treatment | Prognosis |
|---|---|
| Normal strength, only pain | Excellent — urgent treatment may prevent any neurological deficit. |
| Weakness but still able to walk (paraparesis) | Good — recovery of function is likely with prompt treatment. |
| Unable to walk but some leg movement remains | Fair — some recovery possible. |
| Complete paralysis (paraplegia) | Poor — recovery unlikely, especially if >24-48 hours. |
| Loss of sphincter control/function | Very bad prognostic sign — indicates severe, long-standing compression. |
| Factor | Impact on Prognosis |
|---|---|
| Duration of symptoms | The longer symptoms have been present, the poorer the prognosis. |
| Bladder and bowel involvement | Loss of sphincter function indicates advanced compression and poor recovery potential. |
| Cauda equina vs. spinal cord | Recovery is more likely after cauda equina lesions than true spinal cord lesions. |
| Tumor type | Some tumors (lymphoma, myeloma, breast, prostate) are more radiosensitive and respond better to treatment. |
| Timeframe | Interpretation |
|---|---|
| Days to 1-2 weeks | Improvement in this window suggests good recovery potential. |
| After weeks of immobility | Recovery is increasingly unlikely. |
| No improvement after 4-6 weeks | Permanent neurological deficit is likely. |
Nursing implication: Be honest with the patient and family about prognosis. Creating false hope leads to frustration, expense (paying for futile physiotherapy), and damaged trust when recovery does not occur.
SCC requires urgent, coordinated management involving steroids, analgesia, and definitive treatment (radiotherapy or surgery).
Purpose: To reduce inflammation and edema (swelling) around the tumor and spinal cord, thereby relieving pressure and potentially improving neurological function.
| Drug | Dose | Route | Notes |
|---|---|---|---|
| Dexamethasone | 16-24mg | Oral or Intravenous | Start immediately upon suspicion of SCC. Do not wait for imaging confirmation. |
Why dexamethasone?
- Potent anti-inflammatory effect reduces peri-tumoral edema.
- May improve leg weakness within hours to days.
- "Buys time" before radiotherapy or surgery can be arranged.
Nursing actions for steroid administration:
- Give with food or antacids to protect the stomach (steroids cause gastric irritation).
- Monitor for side effects: hyperglycemia (high blood sugar), mood changes, insomnia, increased appetite, oral thrush.
- In HIV/AIDS patients, consider adding fluconazole prophylaxis for fungal infections (steroids increase risk of opportunistic infections).
SCC causes severe pain that requires aggressive management.
| Action | Detail |
|---|---|
| Titrate morphine aggressively | The morphine dose will likely need a substantial increase in the early stages of SCC. |
| Start or increase morphine at the same time as steroids | Do not delay analgesia while waiting for other treatments. |
| Use NSAIDs for bone pain | Add ibuprofen or diclofenac if not contraindicated. |
| Consider adjuvants | Amitriptyline or gabapentin if neuropathic pain is present. |
Nursing tip: A patient who was comfortable on 10mg morphine every 4 hours may need 20mg, 30mg, or more as the compression worsens. Do not be afraid to increase rapidly under medical direction.
| Feature | Detail |
|---|---|
| Urgency | Should commence as soon as possible, ideally within 24 hours of symptom development. |
| Field | Usually includes 1-2 vertebrae above and 1-2 vertebrae below the compression to cover potential microscopic spread. |
| Effect | Shrinks the tumor, relieving pressure on the cord. |
| Availability in Uganda | Available at Uganda Cancer Institute (Mulago) and some regional centers. Many patients cannot access it due to distance and cost. |
Nursing role:
- Arrange urgent referral.
- Explain to family what radiotherapy involves and why it is needed urgently.
- Support the patient during transport and treatment.
| Feature | Detail |
|---|---|
| When indicated | In selected cases where: - Radiotherapy is unavailable - Spinal instability is present - Diagnosis is uncertain (need biopsy) - Rapid neurological deterioration despite steroids |
| Limitations | Requires specialized surgical team and facilities. Not widely available in Uganda. High risk in frail, advanced cancer patients. |
Before starting definitive cancer treatment, rule out infections that can mimic or complicate SCC:
| Infection | Why It Matters |
|---|---|
| Tuberculosis (TB) | TB of the spine (Pott's disease) can cause identical symptoms. Anti-TB treatment is needed, not radiotherapy. |
| Pyogenic osteomyelitis | Bacterial infection of the bone requires antibiotics. |
Nursing implication: If the patient has fever, night sweats, weight loss, or known TB exposure, mention this to the doctor. A simple TB test may change the entire treatment plan.
Once the acute emergency is addressed, meticulous nursing care prevents complications and maintains dignity.
| Problem | Management |
|---|---|
| Urinary retention | Catheterization — intermittent or indwelling catheter. Monitor for infection. |
| Urinary incontinence | Condom catheters (for men), pads, regular changing. Protect skin from moisture. |
| Monitoring | Record intake and output. Watch for signs of urinary tract infection (fever, cloudy urine, pain). |
| Problem | Management |
|---|---|
| Constipation | Very common due to immobility, opioids, and decreased gut motility. Give regular laxatives (senna, lactulose, bisacodyl). |
| Manual evacuation | Patients with complete cord compression may need regular manual removal of stool. Teach family or arrange community nurse support. |
| Enemas | May be needed if constipation is severe and manual evacuation is not possible. |
Immobility from SCC creates high risk for pressure sores (bedsores), which can become infected and cause further suffering.
| Intervention | How to Do It |
|---|---|
| Regular turning | Every 2 hours — day and night. Use a schedule. |
| Helping the patient sit up | For periods during the day if tolerated. Reduces pressure on sacrum and heels. |
| Pressure-relieving mattress or mat | Use foam mattress, water mattress, or thick soft mat. In resource-limited settings, use soft blankets or banana fiber mattresses. |
| Skin inspection | Check sacrum, heels, hips, and elbows daily for redness, blisters, or breakdown. |
| Keep skin clean and dry | Wash gently with warm water and mild soap. Pat dry. Apply barrier cream if needed. |
| Nutrition | Ensure adequate protein and calories to support skin healing. |
Teach family members to turn the patient, check the skin, and report any redness or breakdown immediately.
| Goal | Approach |
|---|---|
| Maintain function | Physiotherapy if available. Passive range-of-motion exercises to prevent contractures. |
| Prevent complications | Deep breathing exercises to prevent pneumonia. Ankle exercises to prevent clots. |
| Realistic expectations | Be honest about prognosis for recovery. If no improvement after weeks, focus on comfort and preventing complications rather than "walking again." |
SCC is devastating. A patient who was walking yesterday may never walk again.
| Issue | Nursing Response |
|---|---|
| Grief for lost function | Allow the patient to mourn. "I know this is very hard. You have lost so much." |
| Fear of burdening family | Reassure: "Your family loves you. We will teach them how to care for you." |
| Depression and hopelessness | Screen for depression. Consider antidepressants. Link with counselor. |
| Financial strain | Catheters, pads, special mattresses, transport for radiotherapy — all cost money. Link with social support and community resources. |
| Family education | Teach family about: turning, catheter care, bowel care, skin care, recognizing infection. |
| Situation | What to Say |
|---|---|
| Early treatment, some weakness but still walking | "We are treating this urgently. There is a good chance you will maintain or regain strength. But we must act quickly." |
| Significant weakness, early treatment | "The treatment should help reduce swelling and pain. We hope for improvement, but I cannot promise you will walk again. Let's see how you respond over the next days and weeks." |
| Complete paralysis after weeks | "I need to be honest with you. After this much time with no movement, recovery is very unlikely. Our focus now is on keeping you comfortable, preventing sores, and supporting you and your family." |
Why honesty matters:
- Families may spend money they don't have on futile physiotherapy.
- Patients may blame themselves for "not trying hard enough" when recovery is impossible.
- Trust is damaged if the patient realizes they were not told the truth.
| Priority | Action | Timeframe |
|---|---|---|
| Recognize emergency | Suspect SCC in any cancer patient with escalating back pain + neurological signs | Immediate |
| Start steroids | Dexamethasone 16-24mg oral or IV | Immediate — do not wait for imaging |
| Give analgesia | Titrate morphine substantially; add NSAIDs | Immediate |
| Assess neurological status | Document strength, sensation, sphincter function | Within 30 minutes |
| Arrange definitive treatment | Urgent referral for radiotherapy (within 24 hours if possible); consider surgery if appropriate | Urgent |
| Rule out infection | TB test if clinically indicated | Before/during definitive treatment |
| Prevent complications | Catheterization for retention; bowel care; pressure sore prevention; regular turning | Ongoing |
| Educate family | Teach turning, skin care, catheter care, bowel care | Before discharge |
| Provide psychosocial support | Address grief, fear, depression; be honest about prognosis | Ongoing |
| Follow up | Monitor for improvement or deterioration; adjust care plan | Daily initially, then weekly |
- Back pain (escalating, >90% of cases)
- Affected legs (heavy, weak, uncoordinated)
- Coughing/sneezing worsens pain
- Known cancer (advanced stage)
- Pain band-like (tight belt sensation)
- Area of numbness below a level
- Incontinence (urinary or bowel)
- Neurological signs (reduced reflexes, decreased tone)
"Thoracic is Top, Lumbar is Low, Cervical is Least"
- Thoracic: 70% (Top frequency)
- Lumbar: 20% (Low frequency)
- Cervical: 10% (Least frequent)
- Steroids (Dexamethasone 16-24mg immediately)
- Titrate analgesia (morphine increase)
- Educate family
- Radiotherapy (urgent referral, within 24 hours)
- Assess neurological status
- Dexa taper if response good
- Catheterize if retention
- Assess pressure areas
- Rehabilitation (realistic goals)
- Explain prognosis honestly
"WALK-WIN, SPHINCTER-LOSE"
- If patient can WALK ➔ WIN (good prognosis)
- If SPHINCTER lost ➔ LOSE (poor prognosis)
- Define spinal cord compression and explain why it is a palliative care emergency.
- List the two main causes of SCC and their percentages (85-90% vertebral metastases, 10% paravertebral masses).
- Name the cancers most commonly associated with SCC (breast, lung, prostate, kidney, lymphoma, myeloma, sarcoma).
- Describe the anatomical distribution of compression (70% thoracic, 20% lumbar, 10% cervical).
- Explain the difference between spinal cord compression and cauda equina compression (below L2).
- Describe the classic progression of symptoms in SCC (pain ➔ weakness ➔ sensory loss ➔ bladder/bowel dysfunction ➔ paralysis).
- List the characteristics of pain in SCC (bony, radicular, band-like, worsened by coughing/sneezing).
- Explain why escalating back pain + heavy legs is sufficient to treat for SCC.
- Describe the physical examination findings in SCC (tenderness, weakness, sensory level, decreased reflexes, decreased rectal tone).
- Discuss investigations — what plain X-ray shows, why normal X-ray doesn't rule out SCC, and what MRI is the gold standard.
- State the single most important prognostic indicator (neurological status before treatment).
- Explain why loss of sphincter function is a bad prognostic sign.
- Describe the immediate management — dexamethasone dose, route, and why it is given urgently.
- Explain the role of radiotherapy — timing, field, and urgency.
- Discuss nursing care — bladder care, bowel care, pressure area prevention, family education.
- Explain why honest communication about prognosis is essential and give examples of what to say in different situations.
- Address the challenges of managing SCC in Uganda — availability of radiotherapy, cost, transport, rural access.
- Clinical guidelines for the management of Spinal Cord Compression in Palliative Care.