
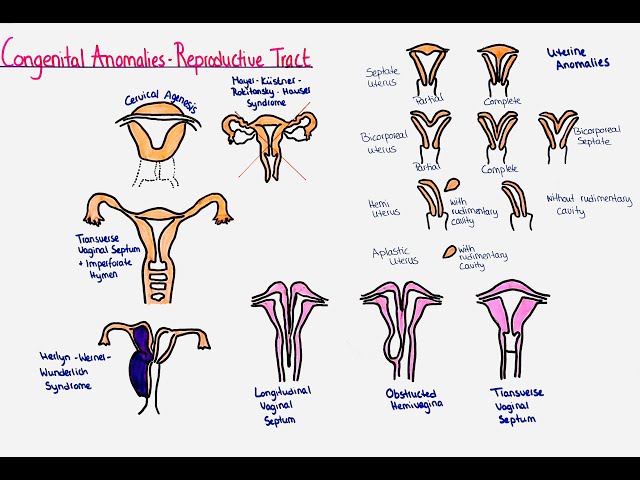
CONGENITAL ANOMALIES OF THE FEMALE GENITAL ORGANS
These are developmental abnormalities of the reproductive female organs that occur intrauterine.
Congenital abnormalities of the female reproductive tract are developmental abnormalities in the reproductive organs that form in the embryo.
Congenital anomalies of the female genital tract result from genetic, environmental, or unknown factors. They can affect various parts of the reproductive system, including the uterus, vagina, cervix, ovaries, and external genitalia.
They result from issues in the embryological development of the Müllerian ducts, which are the precursors to the female reproductive organs.
The Müllerian ducts are two tubes present in the developing embryo. In females, these ducts develop into the fallopian tubes, uterus, cervix, and the upper part of the vagina. Normally, these ducts fuse to form a single uterine cavity and then undergo canalization (hollowing out) to form the fallopian tubes, uterus, and upper vagina.
They can also be referred to as;
- Uterine/vaginal anomalies
- Mullerian anomalies
- Mullerian duct anomalies
- Aplasia (agenesis)
Aetiology/Causes
The cause of these disruptions in embryonic development is usually not known.
- Genetic Factors: Inherited genetic mutations or chromosomal abnormalities. Turner syndrome (affects ovarian development), Androgen Insensitivity Syndrome (affects external genitalia development).
- Environmental Factors: Exposure to harmful substances during pregnancy. Medications like diethylstilbestrol(DES), infections (like rubella), and toxins.
- Unknown Factors: Sometimes, the exact cause is not known.
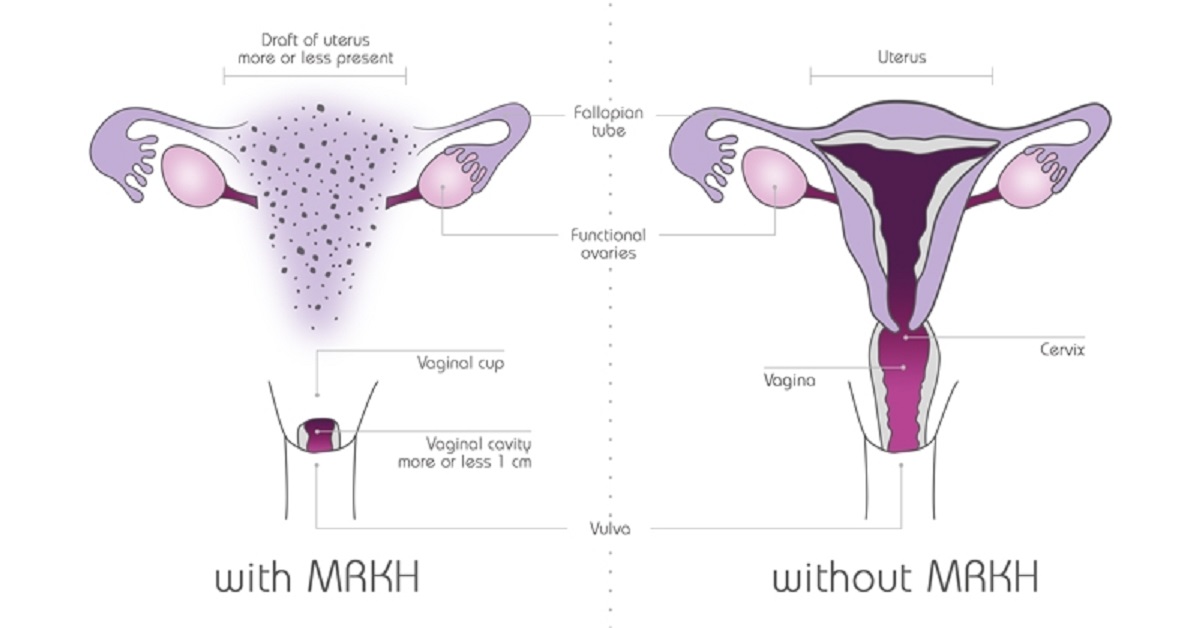
Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome
Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome is a disorder that occurs in females and mainly affects the reproductive system.
This condition causes the vagina and uterus to be underdeveloped or absent, although external genitalia are normal. It is also known as Rokitansky-Küster-Hauser syndrome
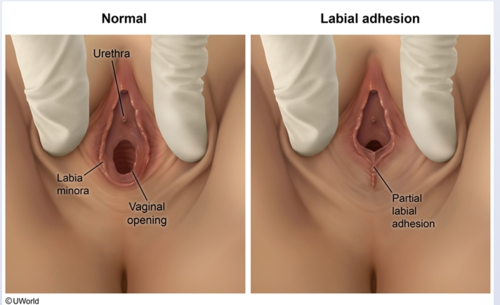
Anomalies of the Vagina
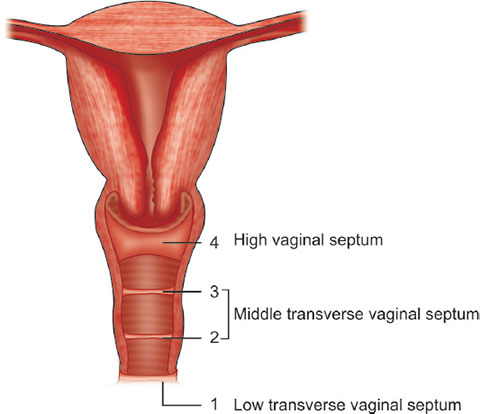
Transverse Vaginal Septum: Horizontal band of tissue partially or completely obstructing the vaginal canal.
- Symptoms: Primary amenorrhea, cyclic abdominal pain, and dyspareunia.
- Management: Surgical excision to restore vaginal patency.
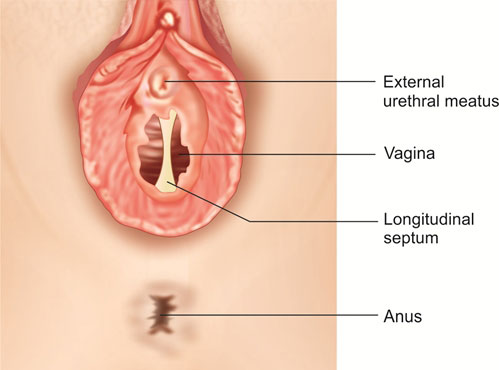
Vertical or Complete Vaginal Septum: A vertical partition dividing the vaginal canal into two separate channels.
- Potential Effects: Dyspareunia, difficulty with tampon use, or complications in childbirth.
- Management: Surgical correction to remove the septum.

Vaginal Agenesis (Mayer-Rokitansky-Küster-Hauser (MRKH) Syndrome): Absence of a vaginal canal, with a functioning uterus or absence thereof.
- Management: Surgical creation of a neovagina using techniques such as tissue grafting, balloon dilation, or bowel vaginoplasty.
- Use of vaginal dilators to create or maintain vaginal width.
Vaginal Atresia: Narrowing or closure of the vagina.
Anomalies of the Cervix
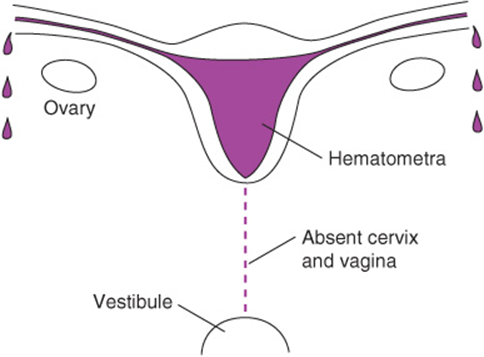
Cervical Agenesis: Absence of the cervix, leading to obstruction of menstrual flow and infertility.
- Clinical Features: Amenorrhea (absence of menstruation); infertility; Hematometra.
- Management: Management depends on the specific situation and may involve surgical reconstruction or assisted reproductive technologies (ART).
Cervical Hypoplasia: Underdevelopment of the cervix.
- Symptoms: Menstrual irregularities, or recurrent pregnancy losses, early onset of cervical incompetence (inability to support pregnancy), and potential fertility problems.
- Management: Depends on severity; fertility treatments or surgical correction may be considered. Cerclage (stitching the cervix) might be used in pregnancy.
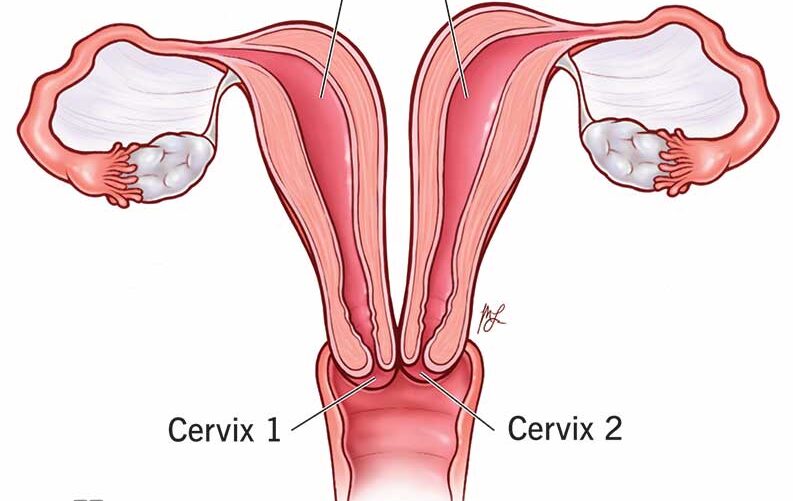
Cervical Duplication: Presence of two cervical canals, often associated with uterine duplication.
- Potential Effects: Obstetric complications, such as difficulty during labor.
- Management: Surgical correction or monitoring during pregnancy.
Anomalies of the Uterus
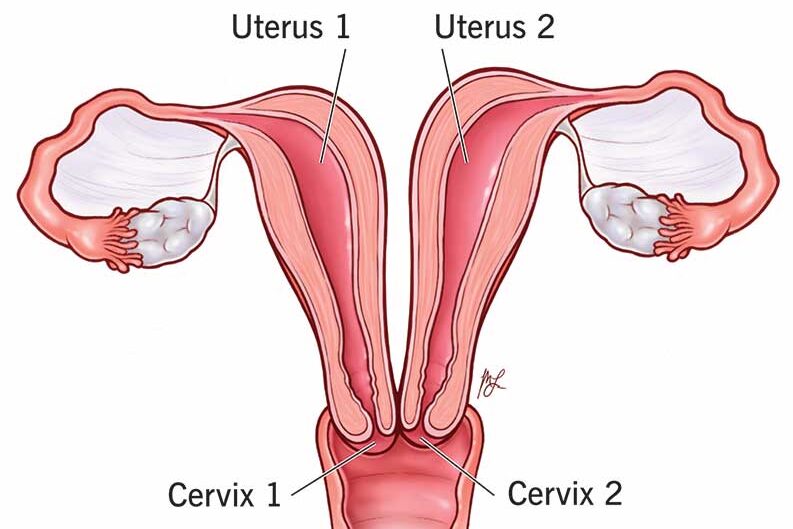
Uterine Duplication: Two separate uterine cavities, each with its own cervix and, in rare cases, separate vaginas.
- Potential Effects: Menstrual irregularities, infertility, or recurrent miscarriages.
- Management: Surgical unification if symptomatic.
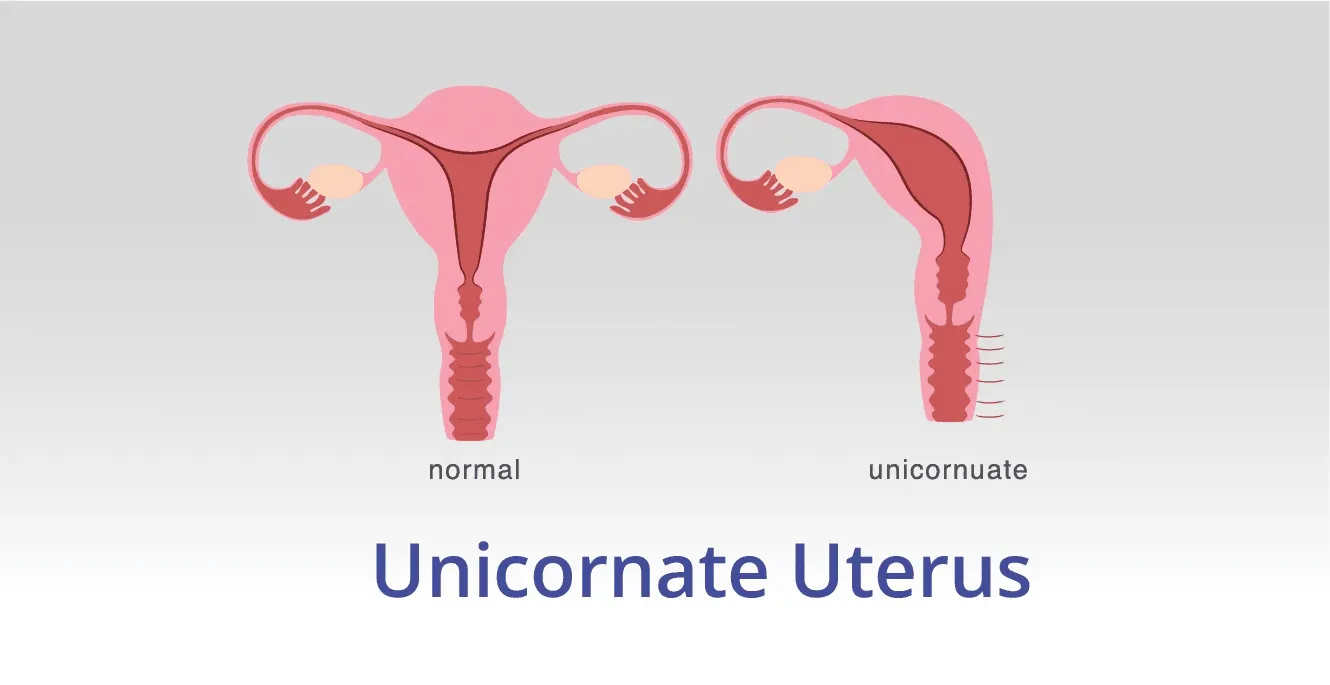
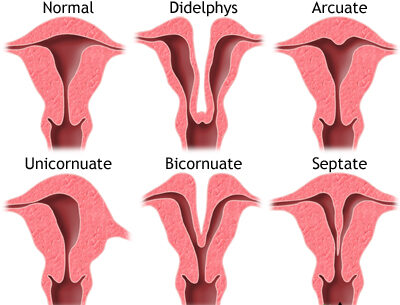
Unicornuate Uterus: Uterus formed from one Müllerian duct, resulting in a single uterine horn.
- Potential Effects: Increased risk of miscarriage, preterm labor, or infertility.
- Management: Monitoring during pregnancy or surgical interventions.
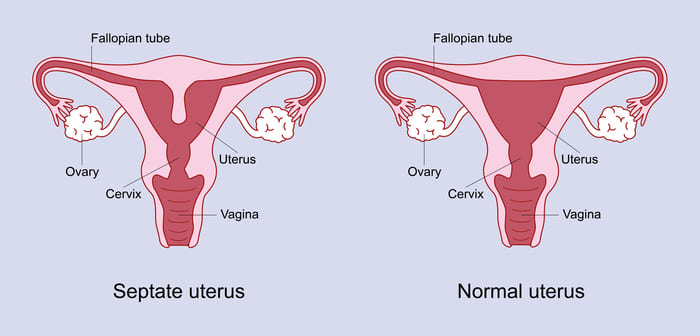
Septate Uterus: A fibrous or muscular septum dividing the uterine cavity.
- Symptoms: Infertility, recurrent pregnancy loss.
- Management: Hysteroscopic metroplasty to remove the septum.
Uterine Agenesis: Complete absence of the uterus, often part of MRKH syndrome.
Management:
- Neovaginal creation for sexual function.
- Gestational surrogacy for childbearing.
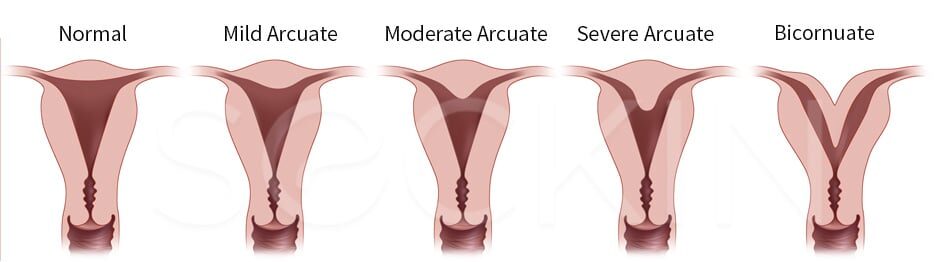
Arcuate Uterus: This is a variation rather than a true anomaly. The uterine cavity has a slightly indented fundus (top portion), giving it a heart-shaped appearance. The indentation is generally shallow. It’s often considered a normal variant and doesn’t usually cause problems with fertility or pregnancy.
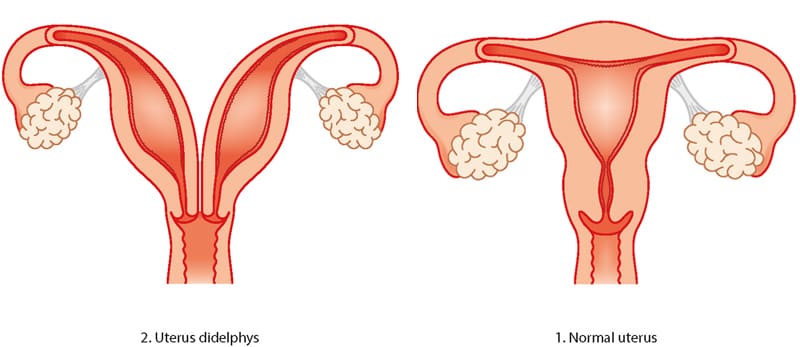
Didelphys Uterus (Uterus Didelphys): This is a complete duplication of the uterus, with two separate uterine horns, each having its own cervix and often its own vagina. Pregnancy complications, such as preterm birth and ectopic pregnancy, are more likely.
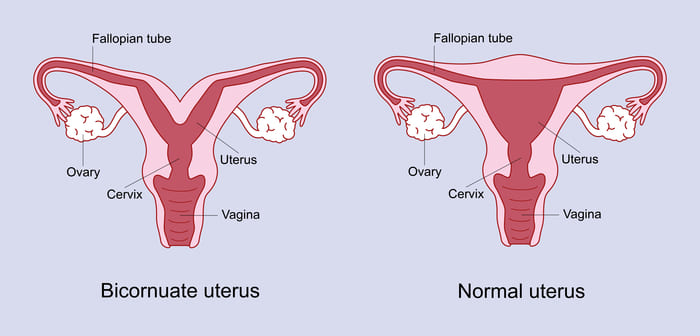
Bicornuate Uterus: This is characterized by a uterus with two horns that are partially fused. There’s a single cervix, but the uterine cavity is partially or completely divided. Similar to a didelphys uterus, there’s a higher chance of pregnancy complications, including miscarriage, preterm labor, and ectopic pregnancy.
Anomalies of the Fallopian Tubes
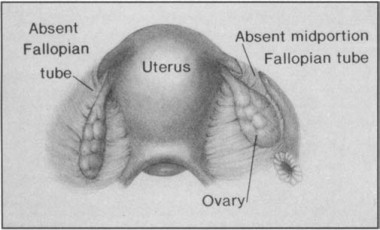
Fallopian Tube Agenesis: Absence of one or both fallopian tubes.
- Potential Effects: Infertility, depending on whether one tube is functional.
- Management: Assisted reproductive technologies like in vitro fertilization (IVF).
Accessory Fallopian Tubes: Presence of extra fallopian tubes, in addition to the normal pair.
- Potential Effects: Increased risk of ectopic pregnancy.
- Management: Surgical removal of accessory tubes.
Tubal Duplication: Presence of duplicated segments in fallopian tubes.
- Potential Effects: Infertility or ectopic pregnancies.
- Management: Corrective surgery.
Tubal Atresia: Underdevelopment or closure of one or more segments of the fallopian tubes.
- Potential Effects: Impaired egg transportation, leading to infertility.
- Management: Surgery or IVF.
good notes
fairly summarized