

Abdominal examination
Abdominal examination is done when the patient is lying supine with a pillow for headrest.
The arms should be by the sides and the bladder must be emptied. The only exception to the procedure is the presence of a history suggestive of stress incontinence. If history suggests chronic retention of urine, catheterization should be done, taking aseptic precautions, using a sterile simple rubber catheter.
The physician usually prefers to stand on the right side.
Actual steps of abdominal examination
INSPECTION:
Abdominal examination assesses for:
Shape of the abdomen
Abdominal distension or masses
Movement with respiration
Presence of scars due to surgery or trauma
Distended veins and presence or absence of striae
Distribution of the pubic hair
Swelling or bulging inguinal orifices (with or without cough impulse)
PALPATION
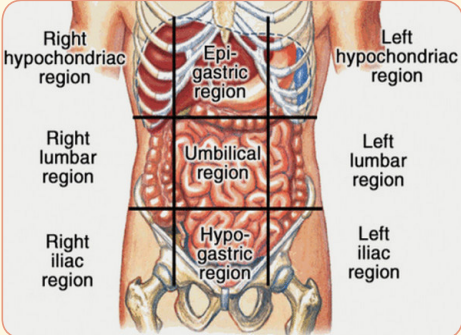
Palpation for tenderness, spleen, liver, kidneys, and for masses. Palpate the abdomen in all the nine regions; right hypochondria (RH), epigastrium (E), Left Hypochondria (LH), Right Lumbar (RL), Umbilical (U), Left Lumbar (LL), Right Iliac (RI), Pubic/Hypogastric (P) and Left Iliac.
Palpation should be done with the flat of the hand gently rather than the tips of the fingers.
If a mass is felt in the lower abdomen, its location, size above the symphysis pubis, consistency, feel, surface, mobility from side to side and from above to down, and margins are to be noted.
PERCUSSION
Percussion is done to assess for presence or absence of gas or fluid in the abdomen. Fluids could be blood or ascites.

AUSCULTATION
Listen for bowel sounds or for fetal heart sounds and rate in case of pregnancy using a stethoscope or fetal stethoscope (fetoscope) respectively.

PELVIC EXAMINATION
- The pelvic examination should be done on an examination couch with patient supine, knees and hips flexed, hips abducted and feet together.
- The examiner stands on the patient’s (right or left) side.
- A good and adjustable light source is needed for inspection of the vulva and for the speculum examination.
- Sterile gloves, sterile lubricant (preferably colourless without any antiseptics), speculum, sponge holding forceps and swabs are required.
- Pelvic examination is usually required when a patient presents with lower abdominal pain, menstrual disorders, abnormal vaginal discharge or to obtain a pap smear.
- Pelvic examination should never be missed unless the patient is a virgin.
- To examine a minor or unmarried, a consent from the parent or guardian is required
- Lower bowel (rectum and pelvic colon) should preferably be empty.
Pelvic examination includes:
1. Inspection of the external genitalia
2. Vaginal examination
- Inspection of the cervix and vaginal walls
- Palpation of the vagina and vaginal cervix by digital examination
- Bimanual examination of the pelvic organs
3. Rectal examination
4. Recto-vaginal examination.
Positions during pelvic examination:

Lithotomy position (patient lying supine with her legs on stirrups) is ideal for examination.
Inspection of the vulva:
- To note any anatomical abnormality starting from the pubic hair, clitoris, labia, and perineum.
- To note any palpable pathology over the areas.
- To note the character of the visible vaginal discharge, if any
- To separate the labia using fingers of the left hand to note external urethral meatus, visible openings of the Bartholin’s ducts (normally not visible unless inflamed), and character of the hymen.
- To ask the patient to strain in order to find out Stress incontinence—urine comes out through the urethral meatus or Genital prolapse and the structures involved— anterior vaginal wall, uterus alone or posterior vaginal wall or all the three.
- Lastly, to look for haemorrhoids, anal fissure, anal fistula, or perineal tear.
Vaginal examination:
We shall look at the following variations of performing vaginal examination:
- Inspection of the cervix and vaginal walls
- Palpation of the vagina and vaginal cervix by digital examination
- Bimanual examination of the pelvic organs
Inspection of the vagina and cervix:
Inspection of the vagina and cervix is done by speculum examination. Two types of speculum are commonly used—Sims’ or Cusco’s bivalve. While in the dorsal position, Cusco is widely used, but in the lateral position, Sims’ variety has advantages.
Introduction of Cusco’s speculum:
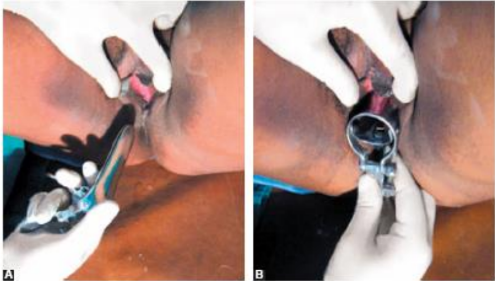
(A) The transverse diameter of the closed blades is placed in the anteroposterior position and inserted slightly obliquely to minimize pressure on the urethra;
(B) Blades are inserted in a downward motion and then rotated. Rotate to 90° and then open up the blades. Inspection is then made using good light. The cervix is best visualized with Cusco’s variety. But while the vaginal fornices are only visualized by Cusco, the anterior vaginal wall is to be visualized by Sims’ variety. Sims’ speculum is advantageous in cases of genital prolapse. Speculum examination should preferably be done prior to bimanual examination.
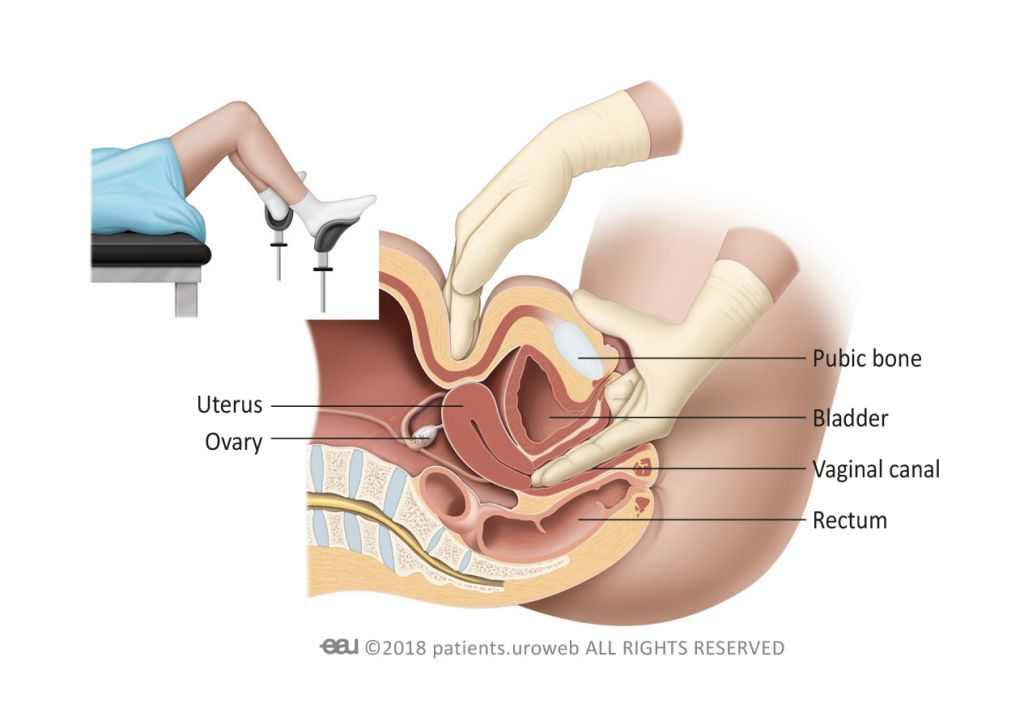
Bimanual Digital examination:
- Explain every step to the patient and reassure her. Inform her that an internal examination is to be performed.
- The labia are gently parted with the gloved index finger and thumb of the non-dominant hand.
- Initially the lubricated index finger of the examiner’s dominant hand is inserted through the introitus into the vaginal canal.
- If the patient is comfortable with this, the lubricated middle finger of the same hand is also inserted.
- If not, due to pain, a limited bimanual examination with one finger can be performed.
- The full length of the finger is introduced, assessing the vaginal walls in transit until the cervix is located.

Factorized completely
It was so helpful