

Human Immunodeficiency Virus (HIV) infection in children is primarily a consequence of mother-to-child transmission (MTCT), also known as vertical transmission. This means the virus is passed from an HIV-infected mother to her child during pregnancy, childbirth, or breastfeeding. While less common in developed nations due to effective prevention programs, pediatric HIV remains a significant public health challenge in many parts of the world, particularly in sub-Saharan Africa.
- HIV (Human Immunodeficiency Virus): A retrovirus that primarily targets and destroys CD4+ T-lymphocytes (helper T-cells), which are crucial components of the immune system. The progressive loss of these cells leads to immunosuppression.
- AIDS (Acquired Immunodeficiency Syndrome): The final, most severe stage of HIV infection, characterized by profound immunosuppression and the appearance of opportunistic infections, certain cancers, and other severe clinical manifestations. In children, the definition of AIDS has specific criteria related to age, CD4 counts, and the presence of certain severe clinical conditions.
- Initially recognized in the early 1980s, pediatric HIV was devastating, often leading to rapid progression to AIDS and early death.
- The development of antiretroviral therapy (ART) in the mid-1990s revolutionized the prognosis for both adults and children with HIV. ART has transformed HIV from a rapidly fatal disease into a manageable chronic condition.
- A major focus globally has been on Prevention of Mother-to-Child Transmission (PMTCT) programs, which have dramatically reduced the rates of new pediatric HIV infections.
The epidemiology of HIV and AIDS in children has seen dramatic shifts over the past few decades, primarily due to the widespread implementation of Prevention of Mother-to-Child Transmission (PMTCT) programs and the availability of Antiretroviral Therapy (ART). However, significant disparities still exist globally.
- Declining New Infections: There has been a remarkable global decline in new HIV infections among children (0-14 years old). From a peak of over 500,000 new infections annually in 2000, this number has fallen dramatically.
- UNAIDS Data (e.g., 2022 estimates): Approximately 89,000 new HIV infections among children (0-14 years) were reported globally in 2022. This represents an 82% decline since 2010. While significant progress, it still means thousands of children are being infected each year.
- Number of Children Living with HIV: Despite the decline in new infections, a substantial number of children continue to live with HIV.
- UNAIDS Data (e.g., 2022 estimates): Around 1.5 million children (0-14 years) were estimated to be living with HIV globally in 2022.
- AIDS-Related Deaths: AIDS-related deaths among children have also fallen considerably due to increased access to ART.
- UNAIDS Data (e.g., 2022 estimates): Approximately 47,000 AIDS-related deaths among children (0-14 years) occurred in 2022.
Geographical Distribution: Sub-Saharan Africa continues to bear the overwhelming majority of the global burden of pediatric HIV. Over 85% of children living with HIV worldwide reside in this region. High prevalence of HIV among women of reproductive age, limited access to comprehensive PMTCT services in some areas, and challenges in diagnosis and treatment for infected children.
This is the primary route by which children become infected with HIV, accounting for over 90% of all pediatric HIV cases globally. MTCT can occur at three distinct phases:
- During Pregnancy (In Utero / Antenatal Transmission): HIV can cross the placenta from the mother's blood into the fetal circulation. This can happen early in pregnancy, but the risk tends to increase as pregnancy progresses, especially in the third trimester.
- Factors: The risk is higher with high maternal viral load, advanced maternal disease, placental inflammation, or coinfections that compromise placental integrity.
- Proportion: Accounts for approximately 5-10% of transmissions without intervention.
- During Labor and Delivery (Intrapartum / Perinatal Transmission): This is the most common period for MTCT without effective interventions. The infant is exposed to the mother's blood and vaginal secretions during passage through the birth canal.
- Factors: High maternal viral load (especially at delivery), prolonged rupture of membranes, invasive delivery procedures (e.g., episiotomy, vacuum extraction, forceps delivery), chorioamnionitis, and bleeding during delivery increase the risk.
- Proportion: Accounts for the majority of MTCT, approximately 10-20% of transmissions without intervention. Elective Cesarean section can significantly reduce this risk if performed before labor and rupture of membranes.
- During Breastfeeding (Postpartum Transmission): HIV can be transmitted from the mother to the infant through breast milk. The virus particles are present in the breast milk.
- Factors: High maternal viral load, mastitis (breast inflammation), breast abscesses, nipple lesions, and mixed feeding (introducing other foods/liquids in addition to breast milk) can increase the risk. The risk is cumulative with the duration of breastfeeding.
- Proportion: Can account for an additional 5-20% of transmissions, depending on the duration of breastfeeding and lack of maternal ART.
These routes are exceedingly rare in the pediatric population in most settings due to stringent public health measures.
- Transfusion of Contaminated Blood or Blood Products: Direct introduction of HIV-infected blood into the recipient's bloodstream.
- Current Status: Extremely rare in most developed countries and increasingly rare globally due to routine screening of all donated blood for HIV and other blood-borne pathogens. In emergency situations or regions with less developed infrastructure, the risk, though small, still exists.
- Contaminated Needles or Syringes: Sharing of needles, accidental needle stick injuries, or reuse of unsterilized needles can transmit HIV.
- Current Status: Very rare in children, primarily seen in specific contexts:
- Accidental exposure: Extremely rare in healthcare settings with proper universal precautions.
- Injection drug use: Almost exclusively seen in adolescents/adults, not typically in young children.
- Unsterile medical practices: Historically, reuse of unsterilized needles/syringes in some medical settings contributed to transmission, but this is largely rectified with single-use equipment.
- Current Status: Very rare in children, primarily seen in specific contexts:
- Sexual Abuse: Unprotected sexual contact between an HIV-positive individual and a child.
- Current Status: A tragic and rare mode of transmission. In cases of child sexual abuse, assessment for HIV (and other sexually transmitted infections) is a crucial part of medical evaluation.
The risk of Mother-to-Child Transmission (MTCT) of HIV is not uniform across all HIV-positive pregnancies. Several factors, both maternal and obstetric, can influence the likelihood of transmission.
- High Maternal Plasma Viral Load: This is the single most important determinant of MTCT risk.
- Mechanism: A higher viral load means more virus particles are circulating in the mother's blood, increasing the chance of viral transfer across the placenta, to the infant during labor and delivery, and into breast milk.
- Intervention: Effective Antiretroviral Therapy (ART) during pregnancy, labor, and breastfeeding is designed to suppress maternal viral load to undetectable levels, thereby dramatically reducing the risk of transmission.
- Lack of ART or Poor Adherence:
- Mechanism: If a mother is not on ART, or is not adherent, her viral load remains high, significantly elevating MTCT risk.
- Intervention: Early diagnosis of maternal HIV, prompt initiation of ART, and sustained adherence are critical.
- Low Maternal CD4+ Count (Advanced Maternal Disease):
- Mechanism: A low CD4+ count indicates a weakened immune system, which is often associated with a higher viral load and a greater likelihood of opportunistic infections that can increase placental inflammation.
- Impact: While viral load is more directly correlated, a low CD4+ count is an indicator of more advanced disease and often correlates with higher viral load, thus increasing MTCT risk.
- Prolonged Rupture of Membranes (PROM):
- Mechanism: If the amniotic sac ruptures for an extended period (e.g., >4 hours) before delivery, the infant has prolonged exposure to HIV-infected maternal blood and cervical secretions.
- Intervention: Timely delivery (often by Cesarean section) if PROM occurs and the mother has a detectable viral load.
- Invasive Delivery Procedures:
- Mechanism: Procedures such as artificial rupture of membranes, fetal scalp electrodes, fetal blood sampling, or instrumental delivery (forceps or vacuum extraction) can create micro-traumas or open wounds, increasing the infant's exposure to maternal blood.
- Vaginal Delivery with High Viral Load:
- Mechanism: During vaginal birth, the infant is exposed to maternal blood, amniotic fluid, and cervicovaginal secretions. If the maternal viral load is high, this exposure is more likely to result in transmission.
- Intervention: Elective Cesarean section is recommended for mothers with detectable viral loads near term to minimize intrapartum exposure.
- Preterm Delivery: Premature infants may have more immature immune systems, less developed skin and mucous membrane barriers, and are more vulnerable to infection.
- Chorioamnionitis (Infection/Inflammation of Placenta and Membranes): Inflammation of the placental membranes can compromise the placental barrier, allowing easier passage of the virus to the fetus. It can also be associated with early rupture of membranes and preterm labor.
- Maternal Genital Tract Infections (e.g., STIs, Bacterial Vaginosis): These infections can cause inflammation and ulceration of the maternal genital tract, increasing shedding of HIV virus and enhancing the risk of exposure for the infant during delivery.
- Breastfeeding:
- Mechanism: HIV can be transmitted through breast milk. The risk is cumulative with the duration of breastfeeding.
- Factors Increasing Risk: High maternal viral load during breastfeeding (if not on ART), mixed feeding (introducing other foods/liquids while breastfeeding, which can damage the infant's gut lining), mastitis (breast inflammation), breast abscesses, and nipple lesions in the mother.
- Intervention: In settings where replacement feeding is safe, feasible, affordable, sustainable, and culturally acceptable (AFASS criteria), avoidance of breastfeeding is recommended. In settings where AFASS is not met, exclusive breastfeeding while the mother is on ART with an undetectable viral load is the recommended approach to minimize transmission risk while providing the benefits of breastfeeding.
- Coinfections: Maternal infections (e.g., malaria, tuberculosis, other STIs) can lead to a transient increase in HIV viral load and/or inflammation, potentially increasing MTCT risk.
- Nutritional Status: Severe maternal malnutrition can compromise immune function and overall health, potentially impacting viral load control and increasing susceptibility to complications.
- Illicit Drug Use: Associated with a higher risk of other infections, poor adherence to ART, and compromised health.
The pathogenesis of HIV infection, particularly in children, hinges on its ability to systematically dismantle the immune system by targeting immune cells, primarily the CD4+ T-lymphocytes.
The human body is made out of millions of different cells. Each body cell often makes new cell parts in order to stay alive and to reproduce. Viruses hide their own material inside the cells of the body, and then, when the body cells try to make new parts, they accidentally make new viruses as well.
HIV mostly enters cells of the immune system. Although HIV infects a variety of cells, its main target is the T4-lymphocyte (CD4): a kind of white blood cell that is responsible for warning the immune system that there are invaders (diseases) in the body. Once HIV binds to a cell structure, it hides its material inside the cell. This turns the cell into a sort of HIV factory.
The process by which HIV enters a host cell and then hijacks its machinery to replicate is a complex, multi-step process. CD4 receptors and co-receptors (chemokine receptors like CCR5 or CXCR4) are essential for HIV entry.
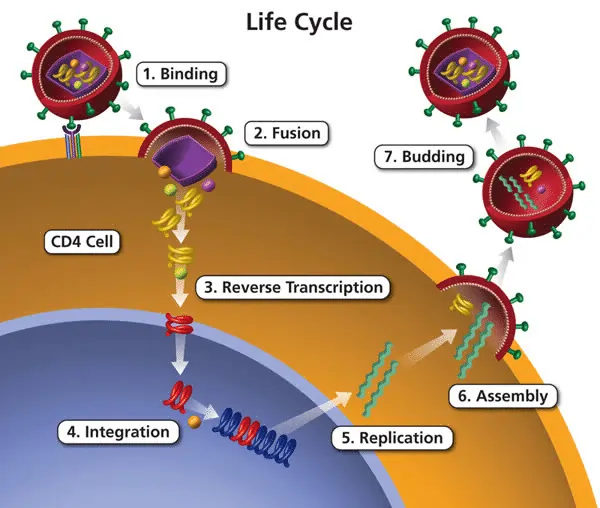
Here are the key phases:
- Viral Entry: Binding and Fusion
- The process begins when the HIV GP120 glycoprotein on the surface of the virus specifically binds to the CD4 receptor on the host cell (primarily CD4+ T-cells, but also macrophages, dendritic cells).
- This binding induces a conformational change in GP120, allowing it to then bind to a chemokine co-receptor (either CCR5 or CXCR4).
- The binding to the co-receptor triggers further changes, exposing the GP41 glycoprotein, which mediates the fusion of the viral envelope with the host cell membrane.
- Once fusion occurs, the viral capsid (containing the viral RNA, enzymes, and other proteins) is released into the cell cytoplasm. Strands of viral RNA are released into the cell cytoplasm.
- Reverse Transcription:
- Inside the cytoplasm, the enzyme reverse transcriptase (carried by the virus) converts the single-stranded viral RNA into a double-stranded DNA copy. This is a unique step for retroviruses, as in nature, DNA typically produces RNA, not the other way around. Now, HIV enters the center of the cell. To do this, it needs to make some important changes in the way it looks so that it will not be ‘recognized’ by the cell. HIV has a special substance to make these changes in its structure.
- Integration:
- The newly synthesized viral DNA, now referred to as a provirus, is transported into the host cell's nucleus.
- The viral enzyme integrase (also carried by the virus) then inserts this proviral DNA into the host cell's chromosomal DNA. HIV is present in the center of the cell, but in a different shape. Once integrated, the viral DNA can remain dormant for periods or become actively expressed.
- Transcription:
- When the infected CD4 cell becomes activated, its cellular machinery is tricked into transcribing the integrated proviral DNA back into multiple copies of viral RNA. These RNA copies serve two main purposes:
- They act as messenger RNA (mRNA) for the production of viral proteins.
- They serve as the genomic RNA for new viral particles.
- HIV RNA has 9 genes which code for the production of structural proteins like the viral envelope and core, in addition to essential enzymes like reverse transcriptase, integrase, and protease. The center of the cell starts to make new parts of HIV instead of making new parts for the body’s defense.
- When the infected CD4 cell becomes activated, its cellular machinery is tricked into transcribing the integrated proviral DNA back into multiple copies of viral RNA. These RNA copies serve two main purposes:
- Translation:
- The viral mRNA is then transported out of the nucleus to the cell's ribosomes, where it is translated into long chains of viral proteins (polypeptide chains).
- Cleavage and Assembly:
- The long polypeptide chains are not functional until they are cut into individual, functional proteins. This crucial step is performed by the viral enzyme protease. Viral protease cleaves the polypeptide chain into enzyme components like integrase and reverse transcriptase, as well as structural proteins. Before leaving the cell, the new parts of HIV need to be put together, just like parts of a car need to be put together in the factory before they can leave the factory to be sold. HIV has a special substance that helps to put the different parts together to form a new HIV before it leaves the cell.
- These newly synthesized viral proteins and genomic RNA molecules then assemble near the inner surface of the host cell membrane.
- Budding and Maturation:
- New viral particles (virions) are formed as the assembled components bud off from the host cell's membrane, acquiring a new lipid envelope in the process. This is the final step in the formation of new infectious HIV particles.
- HIV attacks many CD4 cells. The infected CD4 cells will first produce many new copies of the virus, and then die. The new copies of HIV will then attack other CD4 cells, which will also produce new copies of HIV and then die. This goes on and on: more and more CD4 cells are destroyed, more and more new copies of HIV are made, and new CD4 cells get infected.
HIV's primary mode of attack is the progressive destruction and dysfunction of the immune system, particularly the CD4+ T-lymphocytes (helper T-cells). These cells are central orchestrators of the immune response, coordinating the activities of other immune cells (like B-cells and cytotoxic T-cells) to fight off infections and diseases.
- Direct Infection and Destruction of CD4+ T-cells:
- As we've discussed, HIV preferentially binds to and infects CD4+ T-cells.
- Once inside, the virus replicates, producing thousands of new virions. This process often leads to the lysis (bursting) and death of the infected CD4+ T-cell.
- The newly released virions then go on to infect other healthy CD4+ T-cells, perpetuating a cycle of infection and destruction.
- Indirect Killing of CD4+ T-cells:
- Apoptosis (Programmed Cell Death): Uninfected CD4+ T-cells can also be driven to commit suicide (apoptosis) due to chronic immune activation, bystander effects from infected cells, or exposure to viral proteins.
- Cytotoxic T-Lymphocyte (CTL) Activity: The body's own CTLs, designed to kill infected cells, will destroy HIV-infected CD4+ T-cells. While initially beneficial, this contributes to the overall decline in CD4+ cell count over time.
- Depletion of CD4+ T-cells:
- The continuous cycle of infection, replication, and cell death leads to a progressive decline in the total number of circulating CD4+ T-cells.
- A healthy adult typically has a CD4+ count ranging from 500 to 1,500 cells/mm³. As HIV infection progresses, this count steadily drops.
- Impairment of CD4+ T-cell Function:
- Even before significant CD4+ cell depletion occurs, the function of these cells can be impaired. Infected CD4+ cells may not be able to effectively signal to other immune cells, produce cytokines, or mount a robust immune response.
- This functional impairment, coupled with numerical decline, renders the immune system increasingly ineffective.
- Immune Activation and Exhaustion:
- HIV infection causes chronic immune activation. The body constantly tries to fight the virus, leading to a state of persistent inflammation and immune cell proliferation.
- Over time, this chronic activation can lead to immune exhaustion, where immune cells (including uninfected CD4+ cells) become less responsive and less effective at fighting off pathogens.
- Destruction of Lymphoid Tissues:
- HIV also infects and destroys cells in lymphoid tissues, such as lymph nodes, spleen, and gut-associated lymphoid tissue (GALT). These tissues are crucial sites for immune cell maturation, interaction, and pathogen clearance. Their destruction further compromises immune function.
- Impact on Other Immune Cells:
- While CD4+ T-cells are the primary target, HIV can also infect other immune cells to a lesser extent, such as macrophages, dendritic cells, and microglia (in the brain).
- Infection of these cells can lead to viral reservoirs, facilitate viral dissemination, and contribute to specific HIV-associated complications (e.g., neurocognitive disorders).
- Development of Immunodeficiency (AIDS):
- The cumulative effect of CD4+ T-cell depletion, functional impairment, and immune exhaustion is the development of profound immunodeficiency.
- When the CD4+ count drops below a critical threshold (e.g., 200 cells/mm³ in adults, age-specific thresholds in children), or when certain opportunistic infections or cancers occur, the individual is diagnosed with AIDS (Acquired Immunodeficiency Syndrome).
- At this stage, the body can no longer effectively fight off common infections that a healthy immune system would easily handle.
The breakdown of the immune system leads to a range of clinical consequences, which are severe and rapid in children without treatment:
- Opportunistic Infections: Infections caused by pathogens that typically do not cause disease in individuals with healthy immune systems (e.g., Pneumocystis jirovecii pneumonia, candidiasis, cryptosporidiosis, toxoplasmosis, cytomegalovirus).
- Recurrent Bacterial Infections: Children with HIV often suffer from frequent and severe bacterial infections (e.g., pneumonia, sepsis, otitis media).
- HIV-Associated Malignancies: Certain cancers are more common in individuals with HIV (e.g., Kaposi's sarcoma, non-Hodgkin's lymphoma).
- Wasting Syndrome/Failure to Thrive: Significant unintended weight loss, chronic fever, and diarrhea.
- HIV Encephalopathy (Neurocognitive Disorders): The virus can directly infect brain cells, leading to developmental delays, cognitive impairment, and neurological symptoms, especially in children.
- Other Organ System Damage: HIV can directly or indirectly affect almost every organ system, leading to cardiomyopathy, nephropathy, dermatological conditions, etc.
Good but description of HIV treatment regimen
Dz wondering, well summarized notes
this you for this material,it’s very helpful