
HYPERTENSION
Introduction
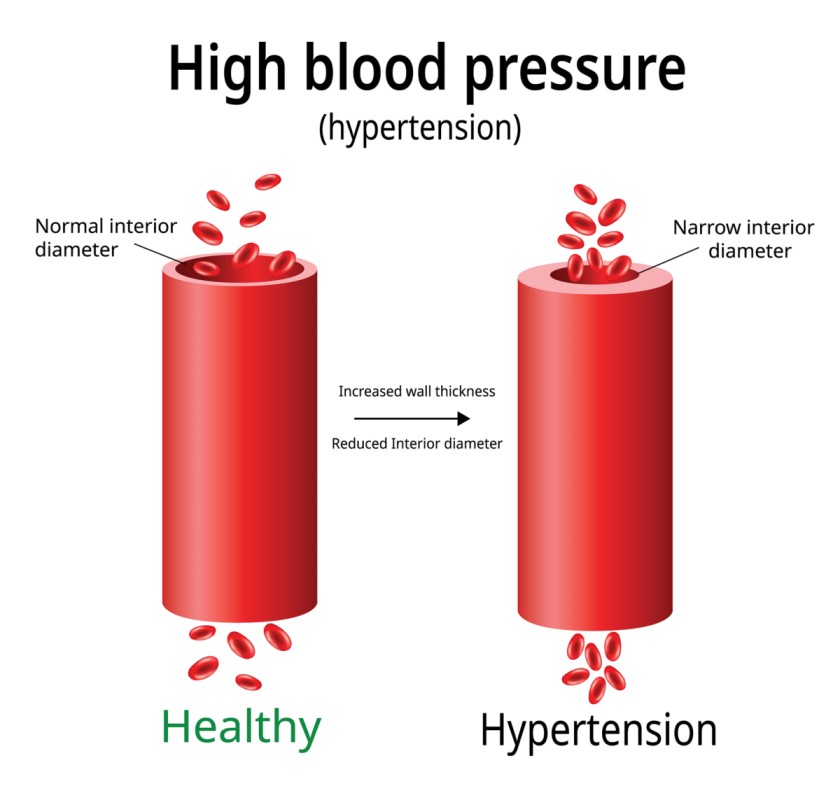
Definition: Hypertension, or high blood pressure (BP), is defined as a persistent systolic blood pressure (SBP) greater than or equal to 140 mm Hg, diastolic blood pressure (DBP) greater than or equal to 90 mm Hg. High blood pressure means that the heart is working harder than normal thus putting the heart and the blood vessels on a high pressure.
This is based on the average of two or more accurate blood pressure measurements during two or more consultations with the healthcare provider. The definition is taken from the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.
- Blood pressure: This is the pressure exerted when blood flows into the arteries. It is measured in mmHg using a sphygmomanometer (blood pressure machine).
- Diastolic pressure: This is the pressure exerted on the arteries when the heart relaxes.
- Systolic pressure: This the pressure exerted on the arteries when the heart contracts.
Types of Hypertension
- Primary (essential or idiopathic) hypertension: elevated BP without an identified cause; accounts for 90% to 95% of all cases of hypertension.
- Secondary hypertension: elevated BP with a specific cause; accounts for 5% to 10% of hypertension in adults.
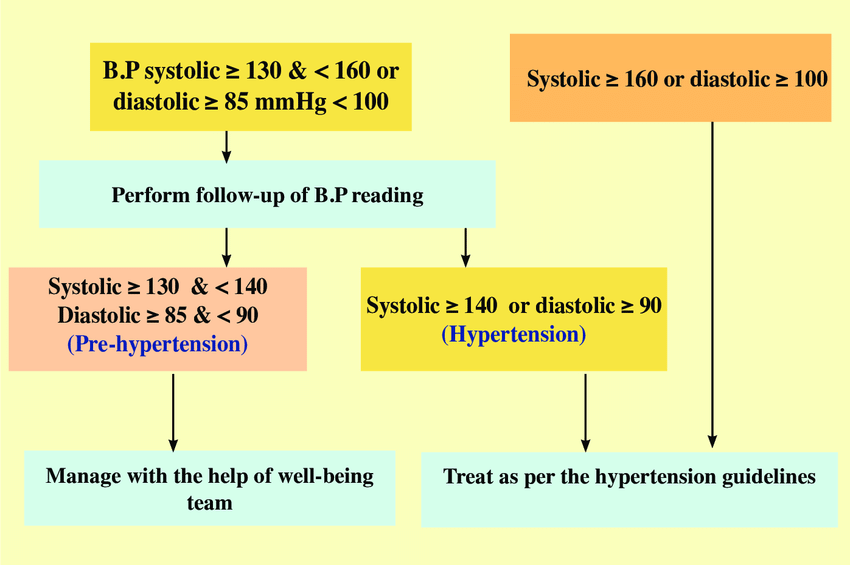
Stages of Hypertension
Blood pressure is classified to guide treatment and assess risk.
| Category | Systolic BP (mmHg) | Diastolic BP (mmHg) |
|---|---|---|
| Normal | less than 120 | and less than 80 |
| Elevated | 120 – 129 | and less than 80 |
| Stage 1 hypertension | 130 – 139 | or 80 – 89 |
| Stage 2 hypertension | 140 or higher | or 90 or higher |
| Hypertensive crisis | higher than 180 | and/or higher than 120 |
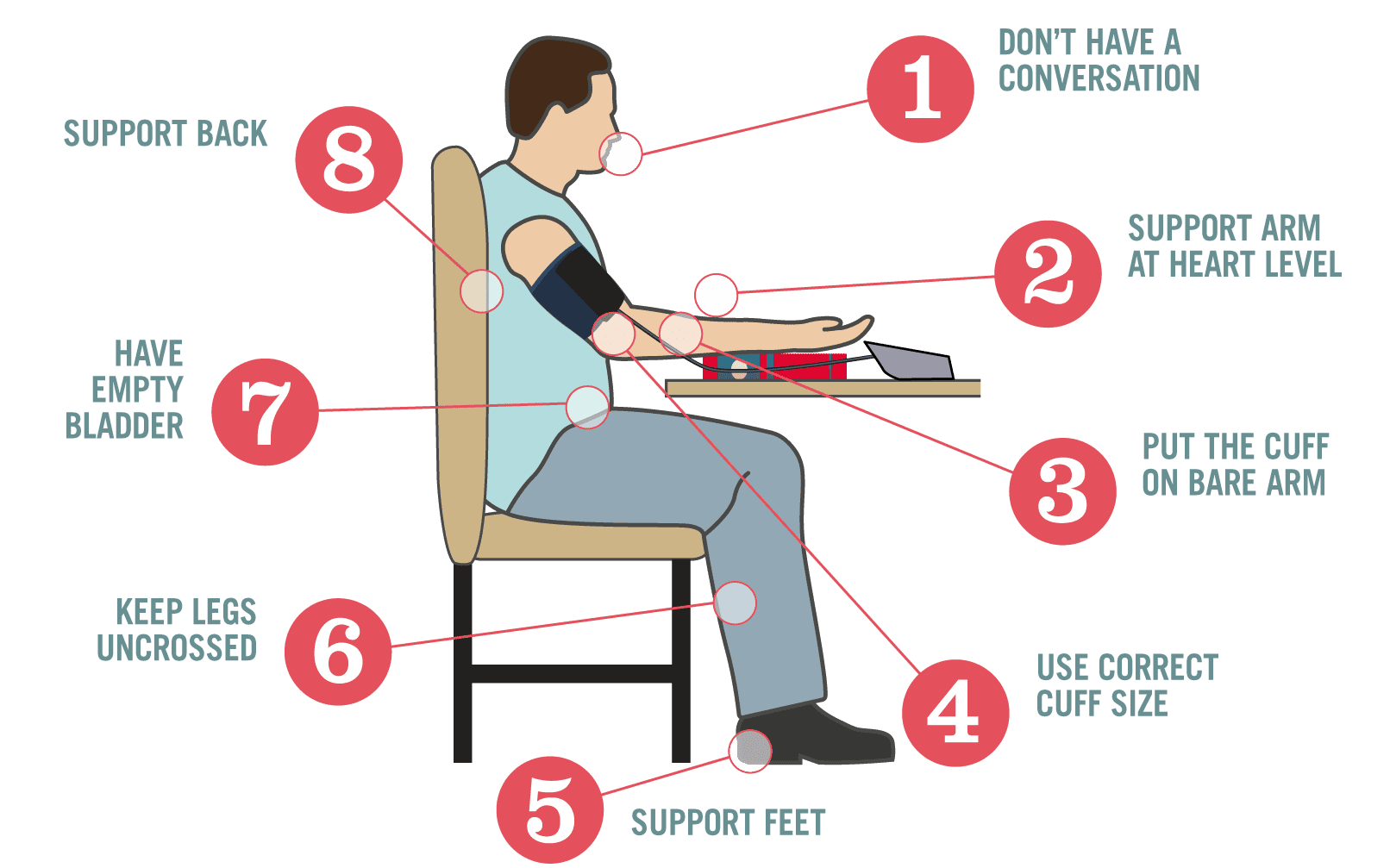
Proper Measurement of Blood Pressure
In order to obtain appropriate results, the following must be followed:
- Right Blood Pressure Machine: The cuff should not be too small or too large for the patient.
- Rest Period: Allow the patient to rest for at least 5 to 10 minutes before measuring the blood pressure, as exercise increases blood pressure.
- Avoid Talking: The patient should not be talking while the blood pressure is being measured, as wrong results (higher) may be obtained when the patient talks.
- Arm Position: The arm of the patient should be positioned at the level of the heart.
- Multiple Measurements: At least 2-3 measurements should be made at different visits for those with pre-hypertension and stage 1 hypertension before the patient is confirmed to be having hypertension.
- Inform Patient: Inform the patient of his or her blood pressure results and what they mean.
- Record and Provide Copy: Record the patient’s blood pressure on the medical form, and a copy of results should be given to the patient.
Pathophysiology
There are various mechanisms described for the development of hypertension which includes increased salt absorption resulting in volume expansion, an impaired response of the renin-angiotensin-aldosterone system (RAAS), increased activation of the sympathetic nervous system. These changes lead to the development of increased total peripheral resistance and increased afterload which in turn leads to the development of hypertension.
Causes of Hypertension
Hypertension has a lot of causes just like how fever has many causes. The factors that are implicated as causes of hypertension are:
- Increased sympathetic nervous system activity: Sympathetic nervous system activity increases because there is dysfunction in the autonomic nervous system.
- Increase renal reabsorption: There is an increase reabsorption of sodium, chloride, and water which is related to a genetic variation in the pathways by which the kidneys handle sodium.
- Increased RAAS activity: The renin-angiotensin-aldosterone system increases its activity leading to the expansion of extracellular fluid volume and increased systemic vascular resistance.
- Decreased vasodilation of the arterioles: The vascular endothelium is damaged because of the decrease in the vasodilation of the arterioles.
Risk factors of Hypertension
- Age: Increasing age increases the risk of development of hypertension
- Family History of the disease increases the risk
- Lack of exercise
- Obesity
- Stress and depression
- Vitamin D deficiency
- Smoking
- Drug abuse and alcoholism
- Cushing syndrome
- Diabetes
- Sedentary lifestyle
- Intake of extra salt
- Insufficient calcium, magnesium, and potassium intake
- Chronic kidney disease
- Adrenal and thyroid problems
- Adrenal gland tumors
- Thyroid problems
- Certain medications such as birth control pills, cough, and cold remedies and over-the-counter pain relievers( NSAIDs)
- Obstructive sleep apnea
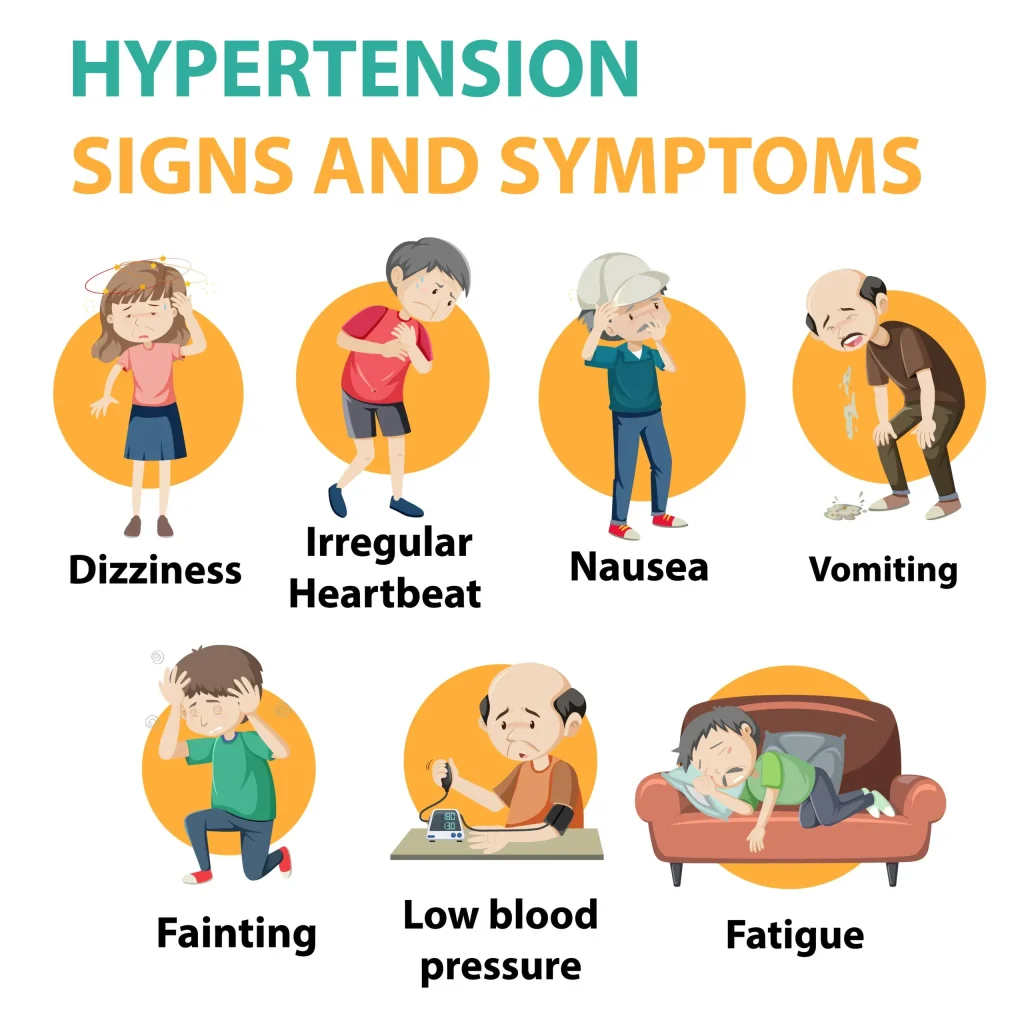
Clinical manifestations
Often called the “silent killer” because it is frequently asymptomatic until it becomes severe and target organ disease occurs.
- Headache: The red blood cells carrying oxygen is having a hard time reaching the brain because of constricted vessels, causing headache.
- Dizziness occurs due to the low concentration of oxygen that reaches the brain.
- Chest pain: Chest pain occurs also due to decreased oxygen levels.
- Blurred vision: Blurred vision may occur later on because of too much constriction in the blood vessels of the eye that red blood cells carrying oxygen cannot pass through.
- Fatigue or confusion,
- Lightheadedness,
- Vertigo,
- Tinnitus,
- Fainting,
- Irregular heartbeat,
- Blood in the urine.
Test and Diagnosis for Hypertension
- History exam
- Physical exam: Manual checking of blood pressure by a sphygmomanometer.
- Urinalysis is performed to check the concentration of sodium in the urine though the specific gravity.
- Blood chemistry (e.g. analysis of sodium, potassium, creatinine, fasting glucose, and total and high density lipoprotein cholesterol levels). These tests are done to determine the level of sodium and fat in the body.
- Renin level. Renin level should be assessed to determine how RAAS is coping.
- Urinalysis: May show blood, protein, or white blood cells; or glucose suggests renal dysfunction and/or presence of diabetes.
- Renin: Elevated in renovascular and malignant hypertension, salt-wasting disorders.
- Urine steroids: Elevation may indicate hyperadrenalism, pheochromocytoma, pituitary dysfunction, Cushing’s syndrome.
- Intravenous pyelogram (IVP): May identify cause of secondary hypertension, e.g., renal parenchymal disease, renal/ureteral -calculi.
- Kidney and renography nuclear scan: Evaluates renal status (TOD).
- Excretory urography: May reveal renal atrophy, indicating chronic renal disease.
Management
Medical Management
The medications used for treating hypertension decrease peripheral resistance, blood volume, or the strength and rate of myocardial contraction.
- For uncomplicated hypertension, the initial medications recommended are diuretics and beta blockers.
- Only low doses are given, but if blood pressure still exceeds 140/90 mmHg, the dose is increased gradually.
- Thiazide diuretics decrease blood volume, renal blood flow, and cardiac output.
- ARBs (Angiotensin II Receptor Blockers) are competitive inhibitors of aldosterone binding.
- Beta blockers block the sympathetic nervous system to produce a slower heart rate and a lower blood pressure.
- ACE inhibitors inhibit the conversion of angiotensin I to angiotensin II and lowers peripheral resistance.
Drug therapy
- ACE Inhibitors (Captopril, Enalapril, Perindopril, Quinapril). an ACE inhibitor is particularly. Useful if heart failure and diabetes present.
- Beta-blockers (Acebutolol, Atenolol, Bisoprolol, Propranolol, Timolol). Slowing the heart rate and reducing the force of the heart.
- Calcium channel blockers (Amlodipine, DIltiazem, Felodipine, Nifedipine, Verapamil). Relaxing blood vessels and control blood pressure.
- Diuretics (Bendroflumethiazide, Chlortalidone, Cyclopenthiazide and Indapamide).
Lifestyle modification
Lifestyle modifications are indicated for all patients with prehypertension and hypertension and include the following:
- Weight reduction: A weight loss of 10 kg (22 lb) may decrease SBP by approximately 5 to 20 mm Hg.
- Dietary Approaches to Stop Hypertension (DASH) eating plan. Involves eating several servings of fish each week, eating plenty of fruits and vegetables, increasing fiber intake, and drinking a lot of water. The DASH diet significantly lowers BP.
- Restriction of dietary sodium to less than 6 g of salt (NaCl) or less than 2.4 g of sodium per day. This involves avoiding foods known to be high in sodium (e.g., canned soups) and not adding salt in the preparation of foods or at meals.
- Restriction of alcohol
- Regular aerobic physical activity (e.g., brisk walking) at least 30 minutes a day most days of the week. Moderately intense activity such as brisk walking, jogging, and swimming can lower BP, promote relaxation, and decrease or control body weight.
- It is strongly recommended that tobacco use be avoided.
- Stress management. Stress can raise BP on a short-term basis and has been implicated in the development of hypertension. Relaxation therapy, guided imagery, and biofeedback may be useful in helping patients manage stress, thus decreasing BP.
Nursing management
1. Assessment of the patient
- a. Carrying out history of the presenting signs and symptoms e.g. fever, headaches among others.
- b. Taking vital observation e.g. TPR/BP and general examination to exclude other diseases
- c. Alerting the doctor who will order for investigations and admission, there the nurse will assist the patient throughout the process
2. To prevent the heart failure as a result of BP > 140 systolic
- a. Monitor bp. Measure in both arms/thighs three times, 3–5 min apart while patient is at rest, then sitting, then standing for initial evaluation. Use correct cuff size and accurate technique.
- b. Note presence, quality of central and peripheral pulses because pulses in the legs/feet may be diminished, reflecting effects of vasoconstriction increased systemic vascular resistance and venous congestion.
- c. Auscultate heart tones and breath sounds to detect pulmonary congestion secondary to developing or chronic heart failure.
- d. Observe skin color, moisture, temperature, and capillary refill time to detect or exclude peripheral vasoconstriction.
3. To relieve pain (head ache among others)
- a. Determine specifics of pain, e.g., location, characteristics, intensity (0–10 scale), onset/duration and note nonverbal cues to identify the pain
- b. Encourage/maintain bed rest during acute phase to minimizes stimulation/promotes relaxation.
- c. Provide/recommend non-pharmacological measures for relief of headache, e.g., cool cloth to forehead; back and neck rubs; quiet, dimly lit room; relaxation techniques (guided imagery, distraction); and diversional activities to reduce cerebral vascular pressure.
4. Diet
- a. Establish a realistic weight reduction plan with the patient, e.g., 1 lb weight loss/wk.
- b. Instruct and assist in appropriate food selections, such as a (DASH diet) diet rich in fruits, vegetables, and low-fat dairy foods referred to as the dash dietary approaches to stop hypertension) diet and avoiding foods high in saturated fat (butter, cheese, eggs, ice cream, meat) and cholesterol (fatty meat, egg yolks, whole dairy products, shrimp, organ meats).
5. To promote patient’s knowledge:
- a. Instruct patient and family about the cause, management of symptoms, signs, and symptoms, and the need for follow-up.
- b. Instruct patient about the factors that may have contributed to the development of the disease.
6. Discharge and Home Care Guidelines
- a. The nurse can help the patient achieve blood pressure control through education about managing blood pressure.
- b. Assist the patient in setting goal blood pressures.
- c. Encourage the involvement of family members in the education program to support the patient’s efforts to control hypertension.
- d. Encourage and teach patients to measure their blood pressures at home.
- e. Emphasize strict compliance of follow-up checkup.
Complications of Hypertension
- Heart attack or stroke,
- Aneurysm,
- Weakened and narrowed blood vessels of the kidney,
- Heart failure,
- Thickened narrowed or torn blood vessels of eyes (Blindness),
- Metabolic syndrome.

Drug Therapy for Hypertension
Drug treatment is recommended for those patients who have not responded to non-drug measures and for those who report when the blood pressure is already very high. One drug (monotherapy) is recommended initially for patients with mild hypertension.
In case of poor response, another drug may be added or substituted.
Patients who present when already in stage 2 hypertension may be started on two drugs at once in lower doses, then adjusted depending on the response.
Choice of Antihypertensive
When choosing a drug for treating hypertension, consider the following in order to safely use the drugs and effectively control blood pressure:
- Co-existing Diseases/Conditions: Patients with other existing diseases or conditions such as pregnancy, asthma, diabetes, heart failure, and angina pectoris. This is because some antihypertensives are not recommended to be used in some of the above conditions.
- Affordability and Accessibility: Ensure affordability and accessibility of the medicine by the patients.
- Allergies: Establish whether the patient is allergic to the drug or not.
- Target Organ Damage: Establish the presence of target organ damage.
Choice of Antihypertensive in Different Conditions
| Condition | 1st Choice | 2nd Choice |
|---|---|---|
| Pregnancy | Methyldopa (Aldomet) | Atenolol, Nifedipine |
| Diabetes Mellitus | Captopril, Lisinopril | Nifedipine, Amlodipine |
| Asthma | Amlodipine, Nifedipine | |
| Preeclampsia or Eclampsia of Pregnancy | Hydralazine (Apresoline) | Labetalol |
| Angina Pectoris | Nifedipine, Amlodipine | Atenolol, Propranolol |
| Heart Failure | Frusemide, Lisinopril, Captopril | Carvedilol |
Resistant Hypertension
This is the persistent elevation of blood pressure above 140/90mmHg despite the use of 3 or more appropriate drug combinations including a diuretic at full doses.
Causes:
- Patients above 60 years
- Poor drug compliance (taking the drugs wrongly)
- Continuous presence of risk factors such as smoking, excessive alcohol intake, and obesity
- Concurrent use of drugs that elevate blood pressure, for example, flu (common cold) preparations (decongestants), painkillers like diclofenac
- Presence of secondary causes of hypertension, for example, kidney failure
Malignant Hypertension, Hypertensive Emergency, Hypertensive Urgency
Malignant Hypertension
Malignant hypertension is a condition characterized by a sudden severe rise in blood pressure resulting in small vessel damages.
Clinical Presentation:
- Confusion
- Headache
- Visual loss
- Coma
It is a medical emergency that requires hospital admission and rapid control of blood pressure over 12 to 24 hours to a normal level.
Hypertensive Emergency
This is a severe elevation of blood pressure (more than 180/120mmHg) with signs of damage to target organs such as the brain and kidney.
The patient must be admitted to the hospital, if possible in an intensive care unit, and pressure must be lowered immediately to prevent damage to the kidney, heart, and brain.
Blood pressure should be gradually lowered since cerebral hypoperfusion can occur if the blood pressure is lowered by more than 40% in the initial 24 hours.
Drugs used to treat hypertensive emergencies in Uganda include intravenous hydralazine or Labetalol.
Hypertensive Urgency
This is a situation in which blood pressure is very elevated but there is no potential organ damage.
The blood pressure must be reduced within 1-2 days, and oral medications are recommended, for example, Nifedipine (Sublingual), Captopril, Labetalol tablet, etc.
Drugs Used in the Treatment of Hypertension
Drugs used in the treatment of hypertension in Uganda include:
- Beta blockers
- Calcium channel blockers
- Diuretics
- Angiotensin converting enzyme inhibitor (ACE inhibitors)
- Angiotensin II antagonist
- Centrally acting antihypertensive
- Direct acting vasodilators
1. Beta Blockers
Beta blockers are the most commonly used drugs in the treatment of hypertension in Uganda because they are affordable and available in most places countrywide.
Examples:
- Propranolol (Inderal)
- Atenolol (Totamol)
- Carvedilol
- Labetalol
Mechanism of Action:
Beta blockers block beta 1 receptors in the heart, which results in slowing of the heart rate and reduction in the force of heart contraction. This action results in lowering of blood pressure.
Indications:
- Hypertension
- Angina pectoris
- Migraine headache
- Congestive heart failure (Carvedilol)
- Post myocardial infarction
Side Effects:
- Impotence
- Wheezing
- Cold extremities
- Bradycardia
- Reduced exercise tolerance
- Tiredness
- Heart failure
Contraindications:
- Patients with asthma
- Patients with acute heart failure
- Heart block
- Chronic obstructive airway disease
- Patients with diabetes mellitus (since they mask signs of hypoglycemia)
- Depression
- Pregnancy and breast feeding
Generally, common beta blockers are recommended for use in pregnant mothers, though prolonged use may lead to growth retardation in fetuses. Beta blockers may be used in breast feeding mothers.
2. Calcium Channel Blockers
Calcium channel blockers are among the first-line drugs used in the treatment of hypertension. They can be used alone or in combination with other antihypertensives such as beta blockers, Angiotensin converting enzyme inhibitors, or diuretics. These drugs can be used safely in patients who also have other co-existing conditions such as asthma, hyperlipidemia, diabetes mellitus, and renal dysfunction.
Examples:
- Nifedipine
- Amlodipine
- Felodipine
Mechanism of Action:
Calcium channel blockers decrease the entry of calcium ions into the smooth muscles, causing vasodilation and lowering of the blood pressure.
Indications:
- Hypertension
- Angina pectoris
Side Effects:
- Flushing
- Oedema
- Headache
- Postural hypotension
- Dizziness
- Weakness
- Heart burn
- Tachycardia
Contraindications:
- 2nd or 3rd degree heart block
- Known hypersensitivity to any of the members
- Severe heart failure
- Severe hypotension
- Pregnancy and breast feeding
Calcium channel blockers, especially Nifedipine, are used in the treatment of hypertension in pregnant mothers.
3. Diuretics
Diuretics are among the first-line drugs used in the treatment of hypertension. Diuretics, for example Bendrofluazide, are safe, cheap, and effective in the treatment of hypertension. These drugs may be used alone or in combination with ACE inhibitors, beta blockers, etc., in the treatment of hypertension.
Classification of Diuretics:
| Class | Example |
|---|---|
| Thiazide Diuretics | Bendrofluazide (Aprinox), Metolazone |
| Loop Diuretics | Frusemide (Lasix) |
| Potassium Sparing Diuretics | Spironolactone |
Mechanism of Action:
Diuretics work by promoting the excretion of large amounts of water in the form of urine, thereby reducing the blood volume and lowering of blood pressure.
Indications:
- Hypertension
- Heart failure
Note: Thiazide diuretics are mainly used in the treatment of hypertension but may be used in mild cases of heart failure. Loop diuretics are commonly used in the treatment of heart failure and rarely in the treatment of hypertension unless associated with fluid overload (oedema).
Side Effects:
| Class | Common Side Effects |
|---|---|
| Thiazide Diuretics | Hypokalaemia, Hyperuricaemia (elevated level of uric acid), Glucose intolerance, Sexual dysfunction (impotence), Weakness, Dehydration |
| Loop Diuretics | Dehydration, Dry mouth, Muscle aches, Hypokalaemia, Elevation of blood sugar, Postural hypotension |
Contraindications:
Thiazide diuretics are not recommended in patients with:
- Gout
- Diabetes
- Hypokalaemia
- Hyperlipidemia
- Known hypersensitivity
Pregnancy and Breastfeeding:
Generally, diuretics should be used with caution during pregnancy and breastfeeding.
4. Angiotensin Converting Enzyme Inhibitors (ACE Inhibitors)
ACE inhibitors are drugs of first choice in the treatment of hypertension and also hypertension in diabetic patients. They may be used alone or in combination with diuretics or beta blockers.
Examples:
- Captopril
- Ramipril
- Lisinopril
- Enalapril
Mechanism of Action:
These drugs interfere with the conversion of Angiotensin I (vasodilator) to Angiotensin II (vasoconstrictor) by inhibiting the Angiotensin converting enzyme. This leads to a reduction of peripheral resistance and lowering of blood pressure.
Indications:
- Hypertension
- Heart failure
- Diabetic nephropathy
Side Effects:
The common side effects associated with the use of ACE inhibitors include:
- Dry irritating cough
- Skin rash
- Taste disturbance
- Angioedema
Contraindications:
- Pregnant mothers
- Patients with renal impairment
- Previous history of angioedema
- Known hypersensitivity to any of the drugs in this group
- Breastfeeding
5. Centrally Acting Antihypertensives
These drugs were among the first to be used in the treatment of hypertension in Uganda. They are no longer used so much in the general management of hypertension because of associated side effects and presence of effective drugs with less side effects.
Examples:
- Methyldopa
- Clonidine
Methyldopa, the only member currently registered in Uganda, is used as a drug of 1st choice in the treatment of hypertension in pregnant mothers because of its safety in this category of patients.
Mechanism of Action:
These drugs inhibit sympathetic outflow from the brain, thereby decreasing total peripheral resistance and lowering of blood pressure.
Indications:
- Hypertension during pregnancy
- Severe hypertension as a 3rd line drug
Side Effects:
- Tiredness
- Headache
- Impotence
- Dizziness
- Mental depression
- Sedation
- Rebound hypertension on withdrawal
Contraindications:
- Severe liver disease
- Known hypersensitivity to methyldopa
6. Angiotensin II Antagonists
These drugs are among the new ones used in the treatment of hypertension. They are as effective as ACE inhibitors but are usually recommended in patients who cannot tolerate ACE inhibitors because of side effects such as cough.
Examples:
- Losartan
- Telmisartan
- Valsartan
- Candesartan
Mechanism of Action:
Angiotensin II antagonists bind tightly at Angiotensin II receptors, preventing the action of Angiotensin II. This action reduces peripheral resistance, resulting in vasodilation and lowering of blood pressure.
Indications:
- Hypertension
- Heart failure
Side Effects:
The most common side effects associated with the use of these drugs include:
- Hypotension
- Dizziness
- Hyperkalaemia
Contraindications:
These drugs should be avoided during pregnancy, especially during the 2nd and 3rd trimester, since they are associated with fetal malformation.
- Breastfeeding mothers
7. Direct Acting Vasodilators
Drugs that belong to this group include:
- Hydralazine
- Minoxidil
Hydralazine is the only member registered in Uganda and is only recommended in the treatment of hypertension that has not responded to other antihypertensives.
The use of hydralazine in the long-term treatment of hypertension is associated with fluid retention and reflex tachycardia, which can be offset by combining it with beta blockers (to prevent reflex tachycardia) or diuretics (to reduce fluid retention).
Mechanism of Action:
Direct acting vasodilators work directly on the blood vessels causing relaxation (widening of the blood vessel) leading to a reduction in the blood pressure.
Indications:
- Severe hypertension
- Hypertensive emergencies
- Hypertension in pregnancy associated with pre-eclampsia and eclampsia
Side Effects:
The following side effects are commonly seen when hydralazine is used:
- Headache
- Tachycardia
- Flushing
- Dyspnoea
- Oedema
- Postural hypotension
Contraindications:
- Angina pectoris
- Patients with heart failure
- Known hypersensitivity
The complications ,nursing management,and prevention are not included
thank you for clarity on hypertension