

Lets first differentiate them.
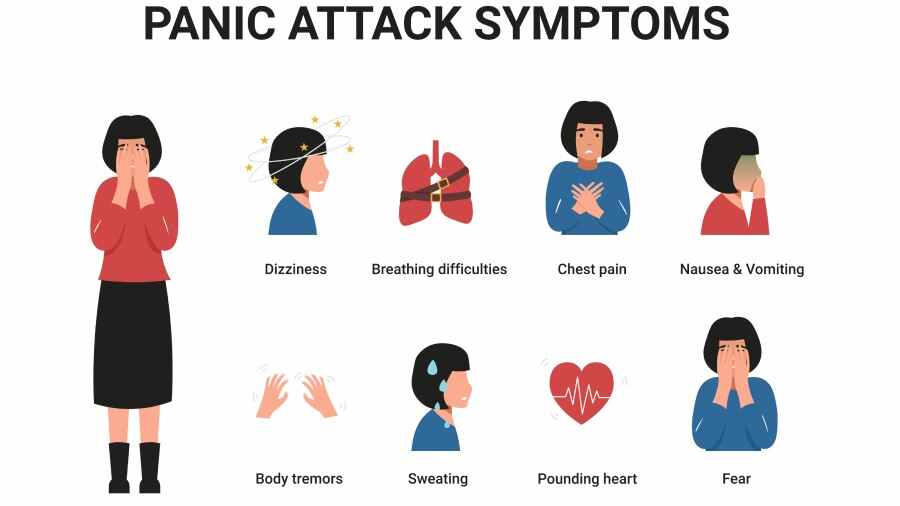
A Panic Attack is an abrupt surge of intense fear or intense discomfort that reaches a peak within minutes, and during which time, four or more of the following symptoms occur:
- Palpitations, pounding heart, or accelerated heart rate.
- Sweating.
- Trembling or shaking.
- Sensations of shortness of breath or smothering.
- Feelings of choking.
- Chest pain or discomfort.
- Nausea or abdominal distress.
- Feeling dizzy, unsteady, light-headed, or faint.
- Chills or heat sensations.
- Paresthesias (numbness or tingling sensations).
- Derealization (feelings of unreality) or depersonalization (being detached from oneself).
- Fear of losing control or "going crazy."
- Fear of dying.
- Expected Panic Attack: Occurs in anticipation of a feared situation (e.g., someone with social anxiety having a panic attack before a public speaking event).
- Unexpected Panic Attack: Occurs "out of the blue" without an obvious trigger. These are particularly central to Panic Disorder.
Panic Disorder is a type of anxiety disorder characterized by recurrent, unexpected panic attacks. The diagnosis is made when an individual experiences:
- Recurrent, unexpected panic attacks.
- At least one of the attacks has been followed by 1 month (or more) of one or both of the following:
- Persistent concern or worry about additional panic attacks or their consequences (e.g., losing control, having a heart attack, "going crazy"). This is often referred to as anticipatory anxiety.
- A significant maladaptive change in behavior related to the attacks (e.g., behaviors designed to avoid having panic attacks, such as avoidance of exercise or unfamiliar situations, or avoidance of places where previous panic attacks occurred). This often leads to the development of agoraphobia.
- Core Feature: The unexpected nature of the panic attacks. It's not just about having panic attacks, but having them without an obvious trigger, leading to a fear of having more panic attacks.
- Anticipatory Anxiety: A constant state of worry about when and where the next attack will strike, leading to hypervigilance for bodily sensations.
- Behavioral Change/Avoidance: People start to avoid situations, places, or even physical sensations (like increased heart rate from exercise) that they associate with previous panic attacks or fear might trigger one. This avoidance can become very pervasive.
It's crucial to distinguish Panic Disorder from other anxiety disorders, as treatment approaches can vary.
- Generalized Anxiety Disorder (GAD):
- Panic Disorder: Characterized by acute, intense, episodic panic attacks, often unexpected, followed by worry about future attacks. The anxiety is typically episodic and focused on the panic attacks themselves.
- GAD: Characterized by chronic, excessive, pervasive, and difficult-to-control worry about a variety of everyday life events (e.g., work, finances, family health). The anxiety is more diffuse and persistent, though individuals with GAD can also experience panic attacks, they are not the central focus of the disorder.
- Social Anxiety Disorder (Social Phobia):
- Panic Disorder: Attacks are often unexpected, and the primary fear is of the panic attack itself or its consequences.
- Social Anxiety Disorder: Panic attacks, if they occur, are expected and always triggered by specific social or performance situations where the individual fears scrutiny or embarrassment (e.g., public speaking, eating in public). The core fear is negative evaluation by others, not the panic attack itself.
- Specific Phobia:
- Panic Disorder: Attacks are often unexpected, and the primary fear is of the panic attack itself.
- Specific Phobia: Panic attacks, if they occur, are expected and consistently triggered by exposure to a specific object or situation (e.g., heights, spiders, flying). The core fear is of the specific object/situation.
- Post-Traumatic Stress Disorder (PTSD):
- Panic Disorder: Focus on unexpected panic attacks and anticipatory anxiety.
- PTSD: Panic attacks can occur, but they are typically expected and triggered by trauma-related reminders or flashbacks. The core features are re-experiencing the trauma, avoidance, negative alterations in cognitions and mood, and alterations in arousal and reactivity.
- Obsessive-Compulsive Disorder (OCD):
- Panic Disorder: Anxiety is related to the recurrence of panic attacks.
- OCD: Anxiety is triggered by obsessions (intrusive thoughts) and relieved by compulsions (repetitive behaviors). While panic can occur due to extreme anxiety from obsessions, it's not the central feature.
A panic attack is an abrupt surge of intense fear or discomfort accompanied by a cluster of specific symptoms. These can be categorized as follows:
These are often the most prominent and distressing, leading many individuals to believe they are having a medical emergency (e.g., heart attack, stroke).
- Cardiovascular: Palpitations, pounding heart, accelerated heart rate, chest pain or discomfort.
- Respiratory: Sensations of shortness of breath, smothering, feelings of choking.
- Gastrointestinal: Nausea or abdominal distress.
- Neurological/Vestibular: Dizziness, unsteadiness, light-headedness, faintness, paresthesias (numbness or tingling), trembling or shaking.
- Thermoregulation: Chills or heat sensations, sweating.
These involve distorted thoughts and misinterpretations that fuel the fear.
- Fear of losing control or "going crazy."
- Fear of dying.
- Derealization: Feelings of unreality (e.g., feeling detached from one's surroundings, world seems dreamlike).
- Depersonalization: Being detached from oneself (e.g., feeling like an observer of one's body, feeling unreal).
The core emotional experience is intense fear.
- Intense fear: Overwhelming and often unprovoked terror.
- Apprehension: A sense of impending doom or danger.
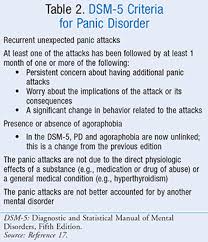
For a diagnosis of Panic Disorder, the following criteria must be met:
The individual must experience recurrent, unexpected panic attacks.
- "Unexpected" means the attack occurs without an obvious trigger or cue. This is a critical distinction from panic attacks that are always tied to a specific situation (e.g., a phobic situation).
- A Panic Attack itself is defined by the abrupt surge of intense fear or intense discomfort that reaches a peak within minutes, during which four or more of the following 13 physical and cognitive symptoms occur: 1. Palpitations, pounding heart, or accelerated heart rate. 2. Sweating. 3. Trembling or shaking. 4. Sensations of shortness of breath or smothering. 5. Feelings of choking. 6. Chest pain or discomfort. 7. Nausea or abdominal distress. 8. Feeling dizzy, unsteady, light-headed, or faint. 9. Derealization (feelings of unreality) or depersonalization (being detached from oneself). 10. Fear of losing control or "going crazy." 11. Fear of dying. 12. Paresthesias (numbness or tingling sensations). 13. Chills or heat sensations.
At least one of the panic attacks has been followed by 1 month or more of one or both of the following:
- Persistent concern or worry about additional panic attacks or their consequences. This includes worries about potential implications like losing control, having a heart attack, or "going crazy." (This is often called anticipatory anxiety).
- A significant maladaptive change in behavior related to the attacks. This involves behaviors adopted to avoid having future panic attacks (e.g., avoidance of exercise, avoidance of unfamiliar situations, social withdrawal, not leaving home).
The disturbance is not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition (e.g., hyperthyroidism, cardiopulmonary disorders). This emphasizes the importance of a thorough medical workup.
The disturbance is not better explained by another mental disorder. For example, the panic attacks are not exclusively due to:
- Social Anxiety Disorder (e.g., panic in response to social situations only).
- Specific Phobia (e.g., panic in response to specific phobic objects/situations only).
- Obsessive-Compulsive Disorder (e.g., panic in response to obsessions only).
- Posttraumatic Stress Disorder (e.g., panic in response to trauma reminders only).
- Separation Anxiety Disorder (e.g., panic in response to separation from attachment figures only).
- While Agoraphobia can be diagnosed independently, it frequently develops as a direct consequence of Panic Disorder.
- The fear of having a panic attack in situations where escape is difficult or help is unavailable leads to avoidance of these situations (e.g., public transportation, open spaces, enclosed places, standing in line, being outside the home alone).
- In severe cases, individuals with agoraphobia may become housebound.
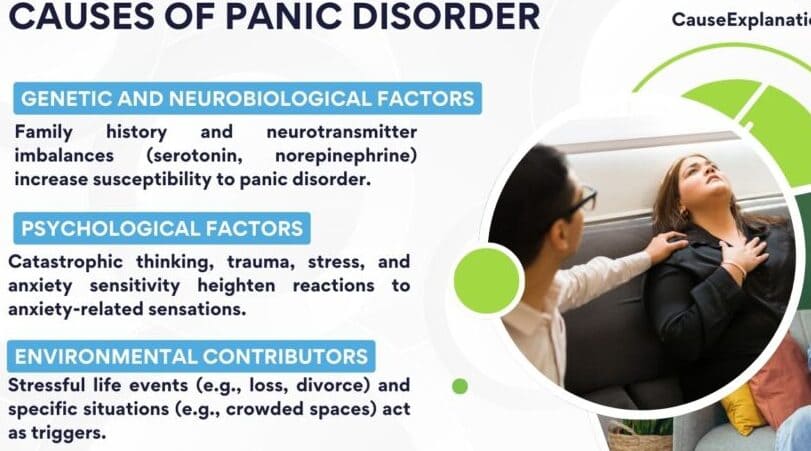
The cause of panic attack is unknown (idiopathic) but the following are thought to trigger panic attacks;
- Genetic Predisposition:
- Panic Disorder often runs in families. First-degree biological relatives of individuals with Panic Disorder are at a higher risk (up to 4-8 times higher) of developing the disorder themselves.
- Twin studies also support a genetic component, with higher concordance rates in monozygotic (identical) twins compared to dizygotic (fraternal) twins. However, genetics alone do not fully explain the disorder, indicating other factors are at play.
- Neurochemical Imbalances:
- Several neurotransmitter systems are implicated in anxiety and panic:
- Norepinephrine: Overactivity in the locus coeruleus (a brain region rich in norepinephrine neurons) is thought to contribute to the physiological arousal and "fight-or-flight" response seen in panic attacks.
- Serotonin: Dysregulation in serotonergic systems is well-established in many anxiety disorders, including panic. Selective Serotonin Reuptake Inhibitors (SSRIs) are a primary treatment, suggesting serotonin's role.
- GABA (Gamma-aminobutyric acid): GABA is an inhibitory neurotransmitter. Reduced GABAergic activity or fewer GABA receptors can lead to increased neuronal excitability and anxiety. Benzodiazepines, which enhance GABA's effects, are effective in acute panic.
- Brain Structures: Abnormalities in brain circuits involving the amygdala (involved in fear processing), hippocampus (memory of fearful events), and prefrontal cortex (emotional regulation) are also being investigated.
- Several neurotransmitter systems are implicated in anxiety and panic:
- Interoceptive Sensitivity and False Suffocation Alarm Theory:
- Interoception: Refers to the perception of internal bodily sensations (e.g., heart rate, respiration, stomach discomfort). Individuals with Panic Disorder often have heightened sensitivity to these normal bodily sensations.
- False Suffocation Alarm Theory: Proposed by Donald Klein, this theory suggests that a subset of individuals with Panic Disorder have a hypersensitive "suffocation alarm" system in the brainstem. This system is normally triggered by changes in CO2 levels (indicating a need for more oxygen), but in these individuals, it may be overly sensitive and fire even when there's no actual threat, leading to feelings of breathlessness and triggering a panic attack.
- Cognitive Misinterpretation of Bodily Sensations:
- This is a cornerstone of the Cognitive-Behavioral Model of Panic. Individuals with Panic Disorder tend to catastrophically misinterpret normal or slightly elevated bodily sensations as signs of impending catastrophe.
- Example: A slight increase in heart rate (e.g., from climbing stairs or drinking coffee) might be interpreted as "I'm having a heart attack," leading to increased anxiety, which further exacerbates physical symptoms, creating a vicious cycle of fear.
- This misinterpretation amplifies benign physiological changes into full-blown panic.
- Anxiety Sensitivity:
- Defined as the fear of anxiety-related sensations due to beliefs that these sensations have harmful consequences (e.g., "When I feel dizzy, I think I might faint and be embarrassed").
- Individuals with high anxiety sensitivity are more likely to develop Panic Disorder. They are not just anxious, but they are afraid of being anxious.
- Conditioning and Learning Theories:
- Classical Conditioning: A neutral stimulus (e.g., a specific location like a crowded mall) can become associated with the intense fear of a panic attack. Subsequently, just being in that location can trigger anxiety or even a panic attack.
- Operant Conditioning (Negative Reinforcement): Avoiding situations that might trigger panic (e.g., agoraphobia) provides immediate relief from anxiety. This relief negatively reinforces the avoidance behavior, making it more likely that the person will continue to avoid those situations, thus maintaining the disorder.
- Stressful Life Events:
- Panic attacks often first occur during periods of significant stress, such as job loss, relationship breakups, deaths of loved ones, or major life transitions. Stress can tax an individual's coping resources and increase physiological arousal, making them more vulnerable.
- Childhood trauma: A history of childhood physical or sexual abuse, or other forms of trauma, is a significant risk factor for developing Panic Disorder.
- Substance Use and Withdrawal:
- Stimulants: Caffeine, nicotine, and illicit stimulants (e.g., cocaine, amphetamines) can induce anxiety and panic-like symptoms due to their impact on the sympathetic nervous system.
- Alcohol/Sedative-Hypnotic Withdrawal: Withdrawal from substances like alcohol or benzodiazepines can lead to severe anxiety, tremors, and even panic attacks, as the nervous system becomes overactive.
- Parenting Styles/Attachment:
- Some research suggests that certain parenting styles (e.g., overprotective, critical) or insecure attachment styles may contribute to a child's vulnerability to anxiety disorders, including panic, by affecting emotional regulation and perceived self-efficacy.
The constant threat of unexpected panic attacks and the associated anticipatory anxiety and avoidance behaviors can severely disrupt nearly every aspect of an individual's life:
- Occupational/Academic:
- Difficulty concentrating due to persistent worry about attacks.
- Avoidance of work/school due to fear of having an attack in public or in demanding situations.
- Absence from work/school, leading to job loss, academic failure, or underemployment.
- Reduced productivity and performance.
- Social Life:
- Withdrawal from social activities and friends, especially if those activities involve feared situations (e.g., crowded places, driving, public transport).
- Fear of embarrassment if a panic attack occurs in public.
- Significant reduction in social support networks, leading to isolation.
- Relationships:
- Strain on family and romantic relationships as partners or family members may struggle to understand or cope with the individual's avoidance and anxiety.
- Dependence on others (e.g., relying on a partner to drive everywhere), which can create resentment or strain.
- Communication difficulties surrounding the illness.
- Leisure and Hobbies:
- Inability to participate in previously enjoyed activities, particularly those requiring travel or public interaction.
- Overall reduction in pleasurable activities due to fear and avoidance.
- Independence:
- In severe cases, particularly with co-occurring agoraphobia, individuals may become housebound, losing all independence and relying entirely on others.
Panic Disorder rarely occurs in isolation. High rates of comorbidity are a significant challenge, complicating diagnosis and treatment, and often leading to worse outcomes.
- Major Depressive Disorder:
- As noted previously, 50-65% of individuals with Panic Disorder will experience a major depressive episode in their lifetime. The chronic stress, impairment, and isolation often contribute to the development of depression.
- The combination of Panic Disorder and depression typically leads to more severe symptoms, greater functional impairment, and a poorer prognosis.
- Other Anxiety Disorders:
- Generalized Anxiety Disorder (GAD): Chronic, excessive worry can co-exist with episodic panic.
- Social Anxiety Disorder: Fear of social situations and potential panic within them.
- Specific Phobias: Co-occurring fears of specific objects or situations.
- Post-Traumatic Stress Disorder (PTSD): Panic attacks can be a symptom of PTSD, or Panic Disorder can develop after a traumatic event.
- Substance Use Disorders:
- Individuals with Panic Disorder have a significantly increased risk of developing alcohol or other substance use disorders (e.g., benzodiazepine abuse, cannabis).
- Substances are often used as a form of "self-medication" to cope with anxiety and panic, though this ultimately exacerbates the problem and leads to dependence.
- Personality Disorders:
- Certain personality disorders, particularly Cluster C (anxious/fearful cluster, e.g., dependent or avoidant personality disorder), can co-occur, making treatment more complex.
The chronic stress and physiological arousal associated with Panic Disorder can have long-term physical health implications, and the constant worry often leads to increased healthcare utilization.
- Cardiovascular Risk:
- Chronic activation of the sympathetic nervous system, elevated heart rate, and blood pressure during panic attacks may contribute to an increased risk of cardiovascular disease over time.
- However, it's more accurate to say that chronic stress and lifestyle factors associated with anxiety disorders (e.g., reduced exercise, poor diet, smoking) contribute to cardiovascular risk.
- Gastrointestinal Issues:
- Chronic anxiety and stress can exacerbate or contribute to conditions like Irritable Bowel Syndrome (IBS) or functional dyspepsia.
- Sleep Disturbances:
- Difficulty falling asleep or staying asleep due to worry, nightmares, or nocturnal panic attacks.
- Increased Healthcare Utilization:
- Individuals with Panic Disorder frequently visit emergency rooms and general practitioners due to physical symptoms, fearing they have a serious medical condition. This leads to numerous diagnostic tests, often with negative results, incurring significant healthcare costs and reinforcing health anxiety if not properly managed.
- Headaches and Chronic Pain:
- Increased muscle tension from chronic anxiety can lead to tension headaches and exacerbate other chronic pain conditions.
Ultimately, the cumulative effect of functional impairment, comorbidity, and physical health issues leads to a significantly reduced quality of life for individuals with Panic Disorder.
- Reduced overall life satisfaction.
- Feelings of helplessness, hopelessness, and demoralization.
- Increased disability and unemployment rates.
- Higher risk of suicidal ideation and attempts (especially when co-occurring with depression).
This is a psychiatric emergency. Managing Panic Disorder (PD) is a process that requires a holistic approach, often involving a multidisciplinary team.
The primary objectives of Panic Disorder management are:
- Decrease Frequency of Attacks: Reduce the number of panic attacks experienced.
- Decrease Intensity of Attacks: Lessen the severity of symptoms during an attack.
- Decrease Anticipatory Anxiety: Alleviate the constant worry about future attacks.
- Decrease Phobic Avoidance: Reduce and eventually eliminate avoidance behaviors, including agoraphobia.
- Treat Co-occurring Psychiatric Disorders: Address common comorbidities such as depression, other anxiety disorders, or substance use disorders.
- Achieve Full Symptomatic Remission: Restore full functioning and quality of life.
A panic attack, especially the first one, can be terrifying and often presents as a medical emergency due to the intensity of physical symptoms.
- Prioritize Medical Rule-Out:
- Urgent Assessment: Any patient presenting with acute chest pain, dyspnea, palpitations, or near syncope requires immediate medical evaluation to rule out life-threatening physical conditions (e.g., myocardial infarction, pulmonary embolism, severe arrhythmias).
- Medical Interventions: Place the patient on oxygen, position them appropriately (supine or Fowler's), and monitor vital signs, pulse oximetry, and perform electrocardiography (ECG). Address any abnormal findings (e.g., ventricular dysrhythmias) immediately.
- Referral: If initial medical workup reveals cardiac or other significant medical abnormalities, the patient must be referred to the appropriate specialist (e.g., cardiologist).
- Ensure Patient Safety:
- Suicide Risk Assessment: Always assess for potential suicide risk at all appointments, especially during acute anxiety crises, or if the patient reports suicidal or homicidal ideation. Inpatient care is warranted if there is evidence of dangerous behavior, severe suicidal ideation with a plan, or significant withdrawal symptoms from substances.
- Calm Environment & Reassurance (Nursing Care): Approach the patient in a calm and quiet manner. For tensed, trembling, or sweating patients, a calm presence helps de-escalate their distress. Provide frequent reassurance and explanation, emphasizing that their symptoms are neither from a serious medical condition nor a psychotic disorder, but rather from a treatable chemical imbalance related to the fight-or-flight response. This psychoeducation is crucial.
- Acute Symptom Relief (Pharmacological - Short-Term):
- In the acute crisis, a few doses of a fast-acting benzodiazepine (e.g., Lorazepam 1-2 mg orally or IM, Diazepam 10-20 mg IV, Clonazepam 0.5-2mg once daily) can be used to quickly alleviate severe anxiety and panic symptoms.
- Caution: Emphasize that benzodiazepines are for short-term, as-needed use, and not for long-term monotherapy, due to the high risk of dependence, withdrawal, and the potential to mask symptoms or interfere with full engagement in psychotherapy. Avoid in patients with a history of substance misuse.
All patients with PD should be monitored by a psychiatrist, psychologist, or other mental health professional. Psychiatric care is highly effective and cost-efficient due to the potential for reducing emergency department visits and overall healthcare costs.
- Patient and Family Education:
- Explain the nature of Panic Disorder, clarifying that symptoms are not indicative of a serious physical illness or psychosis, but a treatable psychological condition.
- Reassure the patient that many people experience similar problems and that the condition is treatable and often short-lived with proper intervention.
- Educate on the "fight-or-flight" response and how it relates to panic symptoms.
- Monitoring:
- Patients should self-monitor their symptoms by keeping a daily diary of panic symptoms and anxiety levels. Rating scales can also be used during sessions.
- Social Services Intervention:
- Provide supportive discussions and explore resources for outpatient care and assistance.
Cognitive Behavioral Therapy (CBT) is considered the most effective and low-cost approach for Panic Disorder, often leading to higher efficacy and lower relapse rates than medication alone, particularly when implemented early.
- Key Components of CBT:
- Psychoeducation: As mentioned, understanding the benign nature of their physical sensations is crucial.
- Cognitive Restructuring: Help patients identify and challenge automatic, catastrophic thoughts and false beliefs/distortions that lead to exaggerated emotional responses during a panic attack. Teach them to recognize that an increased heart rate, for example, is a normal physiological response, not a sign of impending doom.
- Behavioral Therapy / Exposure Therapy:
- Interoceptive Exposure: Gradually expose the patient to anxiety-provoking physical sensations (e.g., spinning in a chair for dizziness, hyperventilating for dyspnea, running in place for increased heart rate). The goal is to desensitize the patient to these sensations, allowing them to learn that these sensations are not dangerous and will pass.
- In Vivo Exposure: Encourage and support the patient in sequentially and gradually confronting situations they have been avoiding (e.g., crowded places, driving, public transport) due to fear of panic. This helps extinguish avoidance behaviors and rebuilds confidence.
- Relaxation Techniques: Teach patients relaxation techniques (e.g., diaphragmatic breathing) to help control hyperventilation during panic and manage overall anxiety levels.
Pharmacological therapy, particularly with SSRIs, is highly effective and often combined with psychotherapy, especially for more severe cases or when psychotherapy alone is insufficient. Patients should be informed about potential adverse reactions, realistic timelines for results, and the likely duration of treatment.
- Selective Serotonin Reuptake Inhibitors (SSRIs):
- First Choice: SSRIs are the first-choice pharmacological treatment for PD.
- Examples: Fluoxetine (10 mg starting, up to 60 mg maintenance), Paroxetine, Sertraline (50 mg starting, up to 200 mg maintenance), Fluvoxamine, Citalopram, Escitalopram.
- Mechanism: Primarily antagonize the 5-HT2 receptor and inhibit the reuptake of 5-HT, increasing serotonin levels in the brain. They have negligible affinity for cholinergic and histaminergic receptors.
- Onset: Initial follow-up care should occur within a week, as SSRIs can cause initial anxiety (jitteriness syndrome) or gastrointestinal issues. Start with the lowest dose and titrate slowly, with full therapeutic effects usually seen in 4-6 weeks.
- Long-Term Management: Educate the patient about the importance of longer-term management with SSRI medication.
- Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs):
- Examples: Venlafaxine (often extended-release), Duloxetine. Trazodone (which is primarily an antidepressant and often used for sleep, though it affects serotonin) is mentioned in your slides as used for PD with or without agoraphobia.
- Mechanism (Venlafaxine/Duloxetine): Inhibit the reuptake of both serotonin and norepinephrine.
- Mechanism (Trazodone): Primarily an antagonist at the 5-HT2 receptor and inhibits the reuptake of 5-HT.
- Use: Effective alternatives if SSRIs are not tolerated or ineffective.
- Benzodiazepines:
- Intermediate to Strong Potency: (e.g., Alprazolam, Clonazepam, Lorazepam, Diazepam).
- Mechanism: Potentiate GABA by binding to specific GABA receptors, leading to rapid anxiolytic effects.
- Role: Primarily for acute symptom control or for short-term use (e.g., to bridge the gap while SSRIs take effect). They should not be used as monotherapy for long-term management of PD due to risks of dependence and abuse.
- Prescription Caution: Dispensing should be limited to ensure patients understand it's a temporary or emergency option. Avoid in patients with a known history of substance misuse or alcoholism. Clonazepam is often preferred for its longer half-life compared to Alprazolam, which has a higher abuse potential.
- Tricyclic Antidepressants (TCAs):
- Examples: Imipramine (25 mg nocte), Amitriptyline (25-50 mg once daily), Desipramine, Clomipramine.
- Mechanism: Serotonin and Noradrenaline reuptake inhibitors.
- Use: Effective, but often discontinued in 35% of cases due to a higher side-effect burden (e.g., blurred vision, dry mouth, dizziness, weight gain, GI disturbances, agitation, headache, insomnia, decreased libido) compared to SSRIs/SNRIs. Start at low doses and titrate gradually to manage side effects.
- Monoamine Oxidase Inhibitors (MAOIs):
- Examples: Phenelzine, Tranylcypromine.
- Mechanism: Nonselective monoamine oxidase inhibitors, increasing endogenous concentrations of dopamine, serotonin, epinephrine, and norepinephrine.
- Use: Highly effective for PD and associated phobias, but typically reserved for refractory cases due to dietary restrictions (tyramine-free diet) and significant drug-drug interaction risks.
- Avoidance of Stimulants: Advise patients to reduce or eliminate caffeine, nicotine (cigarettes), and sympathomimetics (e.g., nasal decongestants), as these can be anxiety-producing agents and interfere with pharmacological therapy.
- Alcohol Reduction: Advise patients to reduce or eliminate alcohol intake, as it can exacerbate anxiety and interfere with treatment.
- Exercise: Encourage regular physical activity, which can reduce overall anxiety and improve mood.
- Relaxation Techniques: Reiterate the importance of techniques like controlled breathing and mindfulness to manage anxiety levels.
- Regular Follow-up: Initial follow-up for SSRI initiation should occur within a week. Continuous monitoring is essential, particularly for the emergence or worsening of depression, which can increase suicide risk.
- Referrals: Refer to chemical dependence treatment specialists if substance use issues are identified.
- Relapse Management:
- Triggers: Patients may experience relapses after successful treatment, especially following significant stressful life events (e.g., loss of a loved one, discovery of a severe illness).
- Strategy: If a relapse occurs, adopt the prior successful treatment plan (CBT, SSRIs, or SNRIs). If the previous approach is no longer effective, consider maintaining CBT and changing the class of pharmacological agents (e.g., switching from an SSRI to a TCA or SNRI).
Nursing staff play a vital role in the management of patients with Panic Disorder.
- Patient Comfort and Safety: These are paramount, particularly during acute episodes.
- Therapeutic Relationship: Approach patients calmly and quietly. Avoid allowing the patient to become overly dependent, as this can interfere with the therapeutic relationship and the patient's progress toward independence. The goal is to empower the patient, not foster dependence.
- Psychoeducation: Educate the patient to accept the reality of their condition and the effectiveness of treatment.
- Encouragement for Exposure: Actively encourage the patient to return to or remain in places or situations that trigger anxiety as part of exposure therapy.
The long-term prognosis for Panic Disorder is generally good.
- Remission Rates: Almost 65% of patients achieve remission, typically within 6 months, with appropriate treatment.
- Effectiveness: Appropriate pharmacologic therapy (especially SSRIs/SNRIs) and cognitive-behavioral therapy, individually or in combination, are effective in more than 85% of cases.
- Cardiovascular Risk: While panic itself can induce myocardial ischemia in patients with existing coronary disease, and increase the risk of sudden death due to reduced heart rate variability and increased QT interval variability, it's also true that patients with PD have nearly double the risk of coronary artery disease. This highlights the importance of managing both the psychiatric and any co-occurring physical health conditions.
Thanks
These notes have really saved my time
They well organized
Thank you
We appreciate your efforts
Greatly understood 😊😊😊
thank you so much for this topic
I really need to know more about this topic