

Lets first differentiate them.
I. Panic Attack
A Panic Attack is an abrupt surge of intense fear or intense discomfort that reaches a peak within minutes, and during which time, four or more of the following symptoms occur:
- Palpitations, pounding heart, or accelerated heart rate.
- Sweating.
- Trembling or shaking.
- Sensations of shortness of breath or smothering.
- Feelings of choking.
- Chest pain or discomfort.
- Nausea or abdominal distress.
- Feeling dizzy, unsteady, light-headed, or faint.
- Chills or heat sensations.
- Paresthesias (numbness or tingling sensations).
- Derealization (feelings of unreality) or depersonalization (being detached from oneself).
- Fear of losing control or "going crazy."
- Fear of dying.
Key Characteristics of a Panic Attack:
- Abrupt onset: Symptoms appear suddenly, not gradually.
- Peak intensity: Reach their peak within 10 minutes (though they can be shorter or longer).
- Intense fear/discomfort: The emotional experience is overwhelming.
- Multiple physical and cognitive symptoms: Not just one or two symptoms, but a cluster.
- Can be expected or unexpected:
- Expected Panic Attack: Occurs in anticipation of a feared situation (e.g., someone with social anxiety having a panic attack before a public speaking event).
- Unexpected Panic Attack: Occurs "out of the blue" without an obvious trigger. These are particularly central to Panic Disorder.
Panic Disorder
Panic Disorder is a type of anxiety disorder characterized by recurrent, unexpected panic attacks. The diagnosis is made when an individual experiences:
- Recurrent, unexpected panic attacks.
- At least one of the attacks has been followed by 1 month (or more) of one or both of the following:
- Persistent concern or worry about additional panic attacks or their consequences (e.g., losing control, having a heart attack, "going crazy"). This is often referred to as anticipatory anxiety.
- A significant maladaptive change in behavior related to the attacks (e.g., behaviors designed to avoid having panic attacks, such as avoidance of exercise or unfamiliar situations, or avoidance of places where previous panic attacks occurred). This often leads to the development of agoraphobia.
Key Characteristics of Panic Disorder:
- Core Feature: The unexpected nature of the panic attacks. It's not just about having panic attacks, but having them without an obvious trigger, leading to a fear of having more panic attacks.
- Anticipatory Anxiety: A constant state of worry about when and where the next attack will strike, leading to hypervigilance for bodily sensations.
- Behavioral Change/Avoidance: People start to avoid situations, places, or even physical sensations (like increased heart rate from exercise) that they associate with previous panic attacks or fear might trigger one. This avoidance can become very pervasive.
Differentiation from Other Anxiety Disorders
It's crucial to distinguish Panic Disorder from other anxiety disorders, as treatment approaches can vary.
- Generalized Anxiety Disorder (GAD):
- Panic Disorder: Characterized by acute, intense, episodic panic attacks, often unexpected, followed by worry about future attacks. The anxiety is typically episodic and focused on the panic attacks themselves.
- GAD: Characterized by chronic, excessive, pervasive, and difficult-to-control worry about a variety of everyday life events.
- Social Anxiety Disorder (Social Phobia):
- Panic Disorder: Attacks are often unexpected, and the primary fear is of the panic attack itself.
- Social Anxiety Disorder: Panic attacks are expected and triggered by specific social or performance situations.
- Specific Phobia:
- Panic Disorder: Attacks are often unexpected.
- Specific Phobia: Panic attacks are expected and consistently triggered by exposure to a specific object or situation.
- Post-Traumatic Stress Disorder (PTSD):
- Panic Disorder: Focus on unexpected panic attacks and anticipatory anxiety.
- PTSD: Panic attacks can occur, but they are typically expected and triggered by trauma-related reminders or flashbacks.
- Obsessive-Compulsive Disorder (OCD):
- Panic Disorder: Anxiety is related to the recurrence of panic attacks.
- OCD: Anxiety is triggered by obsessions and relieved by compulsions.
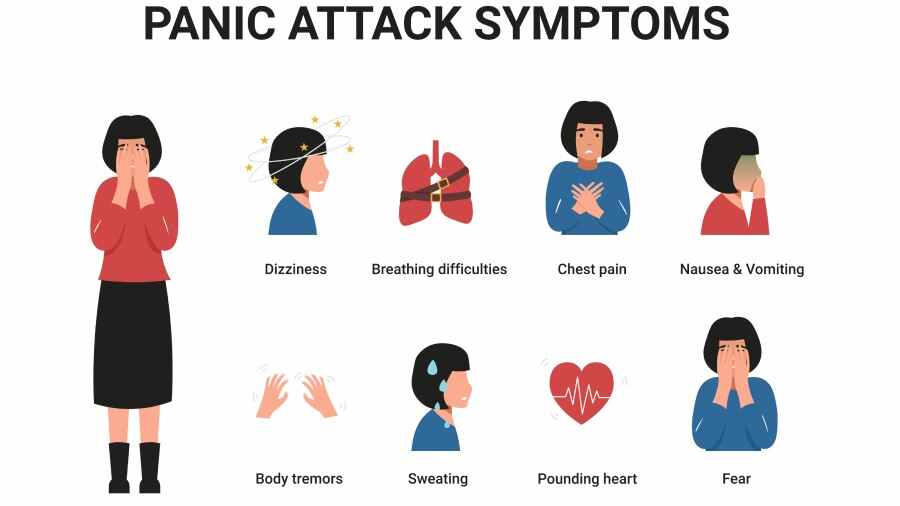
Signs and Symptoms of a Panic Attack
A panic attack is an abrupt surge of intense fear or discomfort accompanied by a cluster of specific symptoms. These can be categorized as follows:
1. Physical/Somatic Symptoms:
These are often the most prominent and distressing, leading many individuals to believe they are having a medical emergency (e.g., heart attack, stroke).
- Cardiovascular: Palpitations, pounding heart, accelerated heart rate, chest pain or discomfort.
- Respiratory: Sensations of shortness of breath, smothering, feelings of choking.
- Gastrointestinal: Nausea or abdominal distress.
- Neurological/Vestibular: Dizziness, unsteadiness, light-headedness, faintness, paresthesias, trembling or shaking.
- Thermoregulation: Chills or heat sensations, sweating.
2. Cognitive Symptoms:
These involve distorted thoughts and misinterpretations that fuel the fear.
- Fear of losing control or "going crazy."
- Fear of dying.
- Derealization: Feelings of unreality.
- Depersonalization: Being detached from oneself.
3. Emotional Symptoms:
The core emotional experience is intense fear.
- Intense fear: Overwhelming and often unprovoked terror.
- Apprehension: A sense of impending doom or danger.
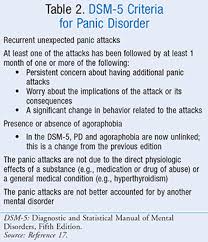
Diagnostic Criteria for Panic Disorder (based on DSM-5-TR)
For a diagnosis of Panic Disorder, the following criteria must be met:
A. Recurrent Unexpected Panic Attacks:
The individual must experience recurrent, unexpected panic attacks.
- "Unexpected" means the attack occurs without an obvious trigger or cue. This is a critical distinction from panic attacks that are always tied to a specific situation (e.g., a phobic situation).
- A Panic Attack itself is defined by the abrupt surge of intense fear or intense discomfort that reaches a peak within minutes, during which four or more of the following 13 physical and cognitive symptoms occur: 1. Palpitations. 2. Sweating. 3. Trembling. 4. Shortness of breath. 5. Feelings of choking. 6. Chest pain. 7. Nausea. 8. Feeling dizzy. 9. Derealization. 10. Fear of losing control. 11. Fear of dying. 12. Paresthesias. 13. Chills or heat sensations.
B. Subsequent Persistent Concern or Behavioral Change:
At least one of the panic attacks has been followed by 1 month or more of one or both of the following:
- Persistent concern or worry about additional panic attacks or their consequences. (Anticipatory anxiety).
- A significant maladaptive change in behavior related to the attacks. (Avoidance of exercise, unfamiliar situations, social withdrawal).
C. Exclusion of Substance/Medical Condition:
The disturbance is not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition. This emphasizes the importance of a thorough medical workup.
D. Exclusion of Other Mental Disorder:
The disturbance is not better explained by another mental disorder. For example, the panic attacks are not exclusively due to Social Anxiety Disorder, Specific Phobia, OCD, PTSD, or Separation Anxiety Disorder.
Development of Agoraphobia (often co-occurs with Panic Disorder):
- While Agoraphobia can be diagnosed independently, it frequently develops as a direct consequence of Panic Disorder.
- The fear of having a panic attack in situations where escape is difficult leads to avoidance of these situations (e.g., public transportation, open spaces).
- In severe cases, individuals with agoraphobia may become housebound.
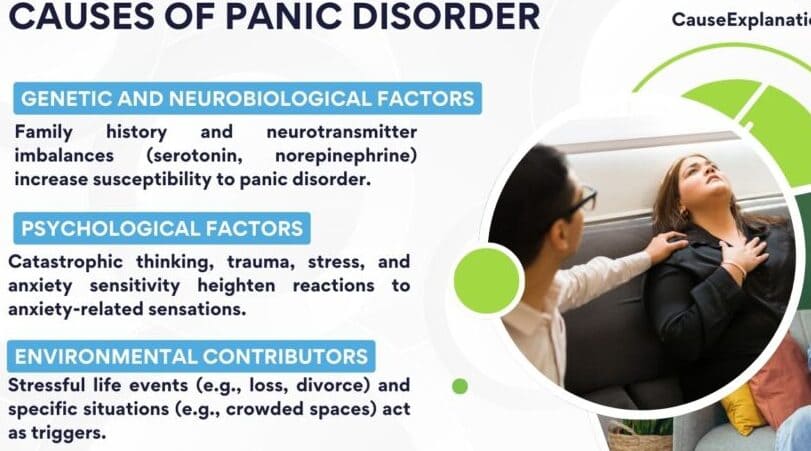
Cause of panic attacks
The cause of panic attack is unknown (idiopathic) but the following are thought to trigger panic attacks;
I. Biological Factors
- Genetic Predisposition:
- Panic Disorder often runs in families. First-degree biological relatives of individuals with Panic Disorder are at a higher risk (up to 4-8 times higher) of developing the disorder themselves.
- Neurochemical Imbalances:
- Several neurotransmitter systems are implicated in anxiety and panic:
- Norepinephrine: Overactivity in the locus coeruleus is thought to contribute to the physiological arousal.
- Serotonin: Dysregulation in serotonergic systems is well-established in many anxiety disorders.
- GABA (Gamma-aminobutyric acid): Reduced GABAergic activity can lead to increased neuronal excitability.
- Several neurotransmitter systems are implicated in anxiety and panic:
- Interoceptive Sensitivity and False Suffocation Alarm Theory:
- Interoception: Individuals with Panic Disorder often have heightened sensitivity to normal bodily sensations.
- False Suffocation Alarm Theory: Suggests that a subset of individuals have a hypersensitive "suffocation alarm" system in the brainstem.
II. Psychological Factors
- Cognitive Misinterpretation of Bodily Sensations:
- Individuals with Panic Disorder tend to catastrophically misinterpret normal bodily sensations as signs of impending catastrophe.
- Anxiety Sensitivity:
- Defined as the fear of anxiety-related sensations due to beliefs that these sensations have harmful consequences.
- Conditioning and Learning Theories:
- Classical Conditioning: A neutral stimulus can become associated with the intense fear of a panic attack.
- Operant Conditioning (Negative Reinforcement): Avoiding situations that might trigger panic provides immediate relief, making avoidance more likely in the future.
III. Environmental/Social Factors
- Stressful Life Events:
- Panic attacks often first occur during periods of significant stress, such as job loss or major life transitions.
- Childhood trauma: A history of abuse or trauma is a significant risk factor.
- Substance Use and Withdrawal:
- Stimulants: Caffeine, nicotine, and illicit stimulants can induce anxiety.
- Alcohol/Sedative-Hypnotic Withdrawal: Withdrawal from substances can lead to severe anxiety and panic attacks.
- Parenting Styles/Attachment:
- Certain parenting styles or insecure attachment styles may contribute to a child's vulnerability to anxiety disorders.
Nursing Concerns/Impact and Complications
I. Impairment in Daily Functioning
The constant threat of unexpected panic attacks and the associated anticipatory anxiety and avoidance behaviors can severely disrupt nearly every aspect of an individual's life:
- Occupational/Academic: Difficulty concentrating, avoidance of work/school, reduced productivity.
- Social Life: Withdrawal from social activities, fear of embarrassment, significant reduction in social support.
- Relationships: Strain on family and romantic relationships, dependence on others.
- Leisure and Hobbies: Inability to participate in previously enjoyed activities.
- Independence: In severe cases, individuals may become housebound.
II. Comorbidity with Other Mental Health Disorders
Panic Disorder rarely occurs in isolation. High rates of comorbidity are a significant challenge.
- Major Depressive Disorder: 50-65% of individuals with Panic Disorder will experience a major depressive episode.
- Other Anxiety Disorders: GAD, Social Anxiety Disorder, Specific Phobias, and PTSD can co-occur.
- Substance Use Disorders: Increased risk of developing alcohol or substance use disorders as a form of "self-medication."
- Personality Disorders: Certain personality disorders can co-occur, making treatment complex.
III. Physical Health Consequences
- Cardiovascular Risk: Chronic activation of the sympathetic nervous system may contribute to an increased risk of cardiovascular disease.
- Gastrointestinal Issues: Chronic anxiety can exacerbate conditions like IBS.
- Sleep Disturbances: Difficulty falling or staying asleep.
- Increased Healthcare Utilization: Frequent visits to emergency rooms leading to numerous diagnostic tests.
- Headaches and Chronic Pain: Increased muscle tension can lead to headaches.
IV. Impact on Quality of Life
- Reduced overall life satisfaction.
- Feelings of helplessness, hopelessness, and demoralization.
- Increased disability and unemployment rates.
- Higher risk of suicidal ideation and attempts.
Thanks
These notes have really saved my time
They well organized
Thank you
We appreciate your efforts
Greatly understood 😊😊😊
thank you so much for this topic
I really need to know more about this topic
thank you for ur service