

Before we define SUD, lets first understand key terms. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), provides the standardized criteria used by clinicians.
I. Key Terms and Definitions
- Substance: Any natural or synthesized chemical that, when taken into the body, alters its functioning. This includes psychoactive substances like alcohol, illicit drugs, prescription medications used non-medically, and even substances like caffeine and nicotine.
- Substance Use: The consumption of a substance. This is a broad term that can range from experimental or recreational use (e.g., having a glass of wine with dinner) to problematic use. Not all substance use is problematic or constitutes a disorder.
- Substance Intoxication: A reversible syndrome of symptoms resulting from the recent ingestion of a substance. These symptoms are specific to the substance and manifest as clinically significant problematic behavioral or psychological changes (e.g., belligerence, mood lability, impaired cognition) that developed during or shortly after substance ingestion.
- Example: Acute alcohol intoxication leading to slurred speech, unsteady gait, and impaired judgment.
- Substance Withdrawal: A syndrome that develops shortly after the cessation of (or reduction in) prolonged, heavy substance use. The symptoms are specific to the substance and cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- Example: Alcohol withdrawal characterized by tremors, sweating, anxiety, and potentially seizures or delirium tremens.
- Tolerance: A need for markedly increased amounts of the substance to achieve intoxication or desired effect, OR a markedly diminished effect with continued use of the same amount of the substance. This is a physiological adaptation.
- Craving: An intense desire or urge for the substance. This is a psychological component, often a powerful driver of continued use and relapse.
- Substance dependence: Refers to a compulsive use and continuous relying on a specific substance for both physical and psychological relief with an inability to stop its usage even after significant problems in everyday functioning have developed.
- Tolerance: Refers to a need for increased amounts of a substance to attain the desired effect.
Substance Use Disorder (SUD) - According to DSM-5
The DSM-5 no longer separates "substance abuse" and "substance dependence" into distinct diagnoses. Instead, it combines them into a single diagnostic category: Substance Use Disorder (SUD), which is measured on a continuum from mild to severe.
A Substance Use Disorder is characterized by a problematic pattern of substance use leading to clinically significant impairment or distress.
It is diagnosed by the presence of at least two of the following 11 criteria occurring within a 12-month period:
Impaired Control (Criteria 1-4):
- Taken in larger amounts or over a longer period than was intended: The individual uses more of the substance or for a longer duration than they initially planned.
- Persistent desire or unsuccessful efforts to cut down or control use: The individual wants to reduce or stop use but struggles to do so.
- A great deal of time is spent in activities necessary to obtain the substance, use the substance, or recover from its effects: The individual's life revolves around the substance.
- Craving, or a strong desire or urge to use the substance: The individual experiences intense urges.
Social Impairment (Criteria 5-7):
- Recurrent substance use resulting in a failure to fulfill major role obligations at work, school, or home: Use interferes with responsibilities (e.g., missing work, neglecting children).
- Continued substance use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of the substance: Use continues even when it's damaging relationships.
- Important social, occupational, or recreational activities are given up or reduced because of substance use: Activities once enjoyed are replaced by substance-seeking/using.
Risky Use (Criteria 8-9):
- Recurrent substance use in situations in which it is physically hazardous: Using in dangerous situations (e.g., driving under the influence, using needles unsafely).
- Continued substance use despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the substance: The individual knows the substance is harming their health but continues to use.
Pharmacological Criteria (Criteria 10-11):
- Tolerance: (As defined above) Need for increased amounts to achieve effect, or diminished effect with continued use of the same amount. Note: This criterion is not met for some substances if used medically under appropriate supervision.
- Withdrawal: (As defined above) Characteristic withdrawal syndrome when substance use is reduced or stopped, or the substance is taken to relieve or avoid withdrawal symptoms. Note: This criterion is not met for some substances if used medically under appropriate supervision.
III. Severity Specifiers
Based on the number of criteria met, SUDs are specified by severity:
- Mild SUD: 2-3 criteria met
- Moderate SUD: 4-5 criteria met
- Severe SUD: 6 or more criteria met
IV. Differentiating from Past Terminology
- "Substance Abuse" (DSM-IV): Implied a pattern of use leading to negative consequences but without physiological dependence. This term is largely replaced by the broader SUD diagnosis.
- "Substance Dependence" (DSM-IV): Implied a compulsive pattern of use with physiological symptoms like tolerance and withdrawal. This is now encompassed within the severe end of the SUD spectrum.
Epidemiology and Prevalence of SUDs
SUDs are a major public health concern globally. They affect millions of people of all ages, socioeconomic statuses, and background. In a typical year, millions of Americans (aged 12 or older) report having an SUD in the past year. This includes significant numbers for alcohol use disorder, illicit drug use disorder, and prescription drug misuse.
- Alcohol Use Disorder (AUD): Often the most prevalent SUD.
- Illicit Drug Use Disorder: Includes cannabis, cocaine, heroin, hallucinogens, inhalants, methamphetamine, and misuse of prescription medications (pain relievers, tranquilizers, stimulants, sedatives). Opioid use disorder (including heroin and prescription pain relievers) remains a significant crisis.
- Co-occurrence with Mental Illness: There is a very high rate of co-occurrence between SUDs and other mental health disorders (often referred to as "dual diagnosis" or "co-occurring disorders"). More than half of individuals with an SUD also have a mental illness, and vice-versa. This complicates treatment and often leads to poorer outcomes if not addressed integratively.
Etiology and Risk Factors for SUDs
Addiction is not a moral failing but a disease with identifiable risk factors that increase an individual's vulnerability. These factors can be broadly categorized:
1. Genetic/Biological Factors:
- Family History: Genetics account for 40-60% of an individual's vulnerability to SUDs. Having a first-degree relative with an SUD significantly increases risk.
- Genetic Predisposition: Specific genes may influence how a person responds to substances (e.g., how they metabolize alcohol, the sensitivity of their reward pathways).
- Neurobiological Vulnerability: Differences in brain structure and function, particularly in areas related to impulse control, stress response, and reward processing, can increase risk.
2. Psychological Factors:
- Mental Health Disorders: Pre-existing mental illnesses (e.g., depression, anxiety disorders, PTSD, ADHD, bipolar disorder, schizophrenia) significantly increase the risk of developing an SUD. Individuals may use substances to self-medicate distressing symptoms.
- Trauma: A history of trauma (e.g., childhood abuse, neglect, combat exposure, sexual assault) is a major risk factor. Trauma can alter brain chemistry and increase vulnerability to both mental health disorders and SUDs.
- Personality Traits: Traits such as impulsivity, sensation-seeking, poor self-regulation, low self-esteem, and difficulty coping with stress can contribute to increased risk.
- Coping Deficits: Lack of healthy coping mechanisms to manage stress, emotions, or life challenges can lead individuals to turn to substances.
3. Social/Environmental Factors:
- Early Exposure: Early initiation of substance use (especially during adolescence when the brain is still developing) is a strong predictor of later SUD.
- Peer Pressure/Social Networks: Association with peers who use substances significantly increases the likelihood of an individual using and developing an SUD.
- Family Environment: Parental substance use, lack of parental supervision, family conflict, weak family bonds, and inconsistent discipline are risk factors.
- Socioeconomic Status: Poverty, unemployment, homelessness, and lack of educational opportunities are associated with higher rates of SUDs.
- Culture and Community Norms: Cultural attitudes toward substance use, availability of substances, and community-level stressors (e.g., discrimination, violence) play a role.
- Stress: Chronic stress from various sources (work, relationships, financial) can increase vulnerability.
Theories Behind the Development of Addiction
Addiction is generally understood through a biopsychosocial model, integrating various theoretical perspectives:
1. Neurobiological Theories (Disease Model):
- Reward Pathway Dysregulation: Substances flood the brain's reward system (mesolimbic dopamine pathway) with dopamine, producing intense pleasure. With repeated use, the brain adapts, reducing its natural dopamine production and making natural rewards less pleasurable. This leads to a need for more of the substance to achieve the same effect (tolerance) and a powerful drive to seek the substance.
- Brain Changes: Chronic substance use causes long-lasting changes in brain structure and function in areas controlling executive function (prefrontal cortex), judgment, decision-making, memory, learning, and behavioral control. These changes contribute to compulsive drug-seeking behavior and impaired impulse control despite negative consequences.
- Genetics: Genetic predispositions influence the brain's vulnerability to these changes.
2. Psychological Theories:
- Learning Theory (Conditioning): Substance use becomes a learned behavior. Positive reinforcement (euphoria, reduced anxiety) drives initial use. Negative reinforcement (relief from withdrawal or distress) maintains use. Cues associated with substance use (people, places, objects) become conditioned stimuli that trigger craving and relapse.
- Cognitive Theory: Focuses on thoughts and beliefs. Individuals may develop cognitive distortions (e.g., "I can only relax with alcohol," "I need drugs to be creative"). Expectations about substance effects and self-efficacy (belief in one's ability to cope) also play a role.
- Psychodynamic Theory: Views substance use as a defense mechanism or a way to cope with underlying psychological conflicts, unresolved trauma, or emotional pain.
3. Sociocultural Theories:
- Social Learning: Individuals learn substance use behaviors and attitudes from observing others (family, peers, media).
- Cultural Influences: Societal norms, cultural traditions, and legal/policy environments shape access and attitudes toward substance use.
- Social Disintegration: Factors like poverty, lack of social support, and community disorganization can contribute to higher rates of SUDs.
Common Substances of Abuse
This objective requires a comprehensive understanding of the physiological and psychological impact of various psychoactive substances.
I. Alcohol (Ethanol)
- Mechanism of Action: Primarily a Central Nervous System (CNS) depressant. Enhances the effects of GABA (inhibitory) and inhibits the effects of glutamate (excitatory). Also affects dopamine and serotonin.
- Acute Effects (Low Dose): Relaxation, disinhibition, mild euphoria, impaired judgment, reduced coordination, slurred speech.
- Intoxication Syndrome:
- Symptoms: Increasing CNS depression (ataxia, slurred speech, nystagmus, impaired memory/cognition), mood lability, aggressive behavior.
- Severe Intoxication/Overdose: Respiratory depression, aspiration risk, stupor/coma, hypotension, hypothermia, ultimately death if untreated. Blood Alcohol Content (BAC) levels correlate with severity.
- Withdrawal Symptoms (Onset 6-24 hours after last drink, peaks 24-72 hours, can last days to weeks):
- Early/Minor: Tremors, anxiety, nausea, vomiting, diaphoresis, headache, insomnia, hypertension, tachycardia.
- Intermediate: Alcoholic hallucinosis (visual, auditory, tactile hallucinations with intact orientation).
- Severe: Withdrawal Seizures (generalized tonic-clonic), Delirium Tremens (DTs): a medical emergency characterized by severe disorientation, agitation, marked tremors, hallucinations, severe autonomic instability (tachycardia, hypertension, fever, diaphoresis). Can be fatal if untreated.
II. Opioids (Heroin, Fentanyl, Oxycodone, Morphine, Hydrocodone, etc.)
- Mechanism of Action: Bind to opioid receptors (mu, kappa, delta) in the brain, spinal cord, and GI tract, mimicking endogenous opioids (endorphins). This inhibits pain signals, produces euphoria, and depresses CNS function.
- Acute Effects (Low Dose): Analgesia, euphoria, sedation, constipation, pupil constriction (miosis), respiratory depression.
- Intoxication Syndrome:
- Symptoms: Pinpoint pupils, respiratory depression (slow, shallow breathing), altered mental status (drowsiness, lethargy), bradycardia, hypotension.
- Overdose: Profound respiratory depression (can lead to respiratory arrest), coma, hypoxia, cyanosis, aspiration, death. Naloxone (Narcan) is an opioid antagonist used to reverse overdose.
- Withdrawal Symptoms (Onset varies by half-life, e.g., short-acting: 6-12 hrs; long-acting: 24-72 hrs. Can last 5-10 days for acute, protracted withdrawal for months):
- Symptoms: Highly unpleasant but rarely life-threatening. Intense craving, dysphoria, anxiety, irritability, muscle aches, lacrimation (tearing), rhinorrhea (runny nose), pupillary dilation (mydriasis), piloerection ("goosebumps"), nausea, vomiting, diarrhea, abdominal cramping, yawning, fever, insomnia.
III. Stimulants (Cocaine, Amphetamines, Methamphetamine, Methylphenidate, MDMA/Ecstasy)
- Mechanism of Action: Primarily increase the release of and/or block the reuptake of dopamine, norepinephrine, and serotonin in the CNS.
- Acute Effects (Low Dose): Increased energy and alertness, euphoria, decreased appetite, increased heart rate and blood pressure, talkativeness, enhanced self-esteem.
- Intoxication Syndrome:
- Symptoms: Hyperactivity, agitation, paranoia, psychosis (hallucinations, delusions), dilated pupils, tachycardia, hypertension, chest pain, arrhythmias, hyperthermia, seizures.
- Overdose: Severe cardiovascular events (myocardial infarction, stroke), hyperthermic crisis, severe psychosis, seizures, rhabdomyolysis, renal failure, death.
- Withdrawal Symptoms (Onset hours to days, lasts days to weeks, often called "Crash"):
- Symptoms: Profound dysphoria, fatigue, hypersomnia, increased appetite, vivid unpleasant dreams, psychomotor retardation or agitation, severe depression (often with suicidal ideation), intense craving. Not typically life-threatening physically, but severe psychological distress.
IV. Cannabis (Marijuana, Hashish)
- Mechanism of Action: Primary active compound, Delta-9-tetrahydrocannabinol (THC), acts on cannabinoid receptors (CB1 and CB2) in the brain and peripheral nervous system, affecting pleasure, memory, thinking, concentration, movement, coordination, and sensory/time perception.
- Acute Effects (Low Dose): Euphoria, relaxation, altered perception of time, intensified sensory experiences, increased appetite ("munchies"), impaired motor coordination, dry mouth, red eyes, increased heart rate.
- Intoxication Syndrome:
- Symptoms: Impaired motor coordination, anxiety, paranoia, panic attacks, impaired judgment, memory impairment, perceptual disturbances (depersonalization, derealization).
- High Dose/Overdose (rarely fatal): Can induce acute psychosis (especially in vulnerable individuals), severe anxiety/panic, severe nausea/vomiting (Cannabinoid Hyperemesis Syndrome with chronic use).
- Withdrawal Symptoms (Onset 24-72 hours, peaks within a week, can last weeks):
- Symptoms: Irritability, anger, anxiety, depression, sleep disturbances (insomnia, vivid dreams), decreased appetite, restlessness, abdominal pain, tremors, sweating, headache, fever.
V. Sedatives, Hypnotics, or Anxiolytics (Benzodiazepines: Lorazepam, Diazepam, Alprazolam; Barbiturates: Phenobarbital)
- Mechanism of Action: Enhance the effects of GABA, leading to CNS depression. Similar to alcohol in their effects.
- Acute Effects (Low Dose): Reduced anxiety, sedation, muscle relaxation, impaired coordination, disinhibition.
- Intoxication Syndrome:
- Symptoms: Slurred speech, ataxia, nystagmus, impaired attention or memory, stupor, coma.
- Overdose: Profound CNS depression, respiratory depression, hypotension, hypothermia, death. Especially dangerous when combined with alcohol or other CNS depressants. Flumazenil can reverse benzodiazepine overdose but carries seizure risk in chronic users.
- Withdrawal Symptoms (Onset varies by half-life, e.g., short-acting: 12-24 hrs; long-acting: several days. Can last weeks to months):
- Symptoms: Often severe and potentially life-threatening. Anxiety, agitation, irritability, insomnia, tremors, autonomic hyperactivity (tachycardia, diaphoresis, hypertension), nausea, vomiting, muscle aches, seizures, delirium. Benzodiazepine withdrawal is medically dangerous and requires medical supervision and often a slow taper.
VI. Hallucinogens (LSD, Psilocybin/Mushrooms, PCP, Ketamine, MDMA/Ecstasy - also a stimulant)
- Mechanism of Action: Highly variable depending on the substance.
- Classic Hallucinogens (LSD, Psilocybin): Primarily act on serotonin receptors (5-HT2A).
- Dissociatives (PCP, Ketamine): Act on NMDA glutamate receptors.
- Acute Effects:
- LSD/Psilocybin: Perceptual distortions (visual, auditory), hallucinations, altered sense of self/time, synesthesia, intense emotions (euphoria to anxiety/panic), spiritual experiences, dilated pupils.
- PCP/Ketamine: Dissociation (feeling detached from body/environment), numbness, impaired coordination, distorted perceptions, belligerence, agitation, psychosis, nystagmus, hypertension, tachycardia.
- Intoxication Syndrome:
- Symptoms: "Bad trip" (severe panic, paranoia, intense fear), acute psychosis (delusions, hallucinations), aggressive behavior (PCP), hyperthermia, seizures (PCP).
- Overdose (PCP/Ketamine): Respiratory depression, coma, seizures, severe hypertension/cardiovascular events.
- Withdrawal Symptoms:
- Classic Hallucinogens: No significant physical withdrawal syndrome. Some users may experience persistent perceptual problems or Hallucinogen Persisting Perception Disorder (HPPD).
- PCP/Ketamine: Can cause dysphoria, depression, anxiety, craving, cognitive difficulties, and sometimes a protracted withdrawal-like syndrome.
Assessment of SUDs
It aims to gather a holistic picture of the individual's substance use patterns, associated problems, strengths, and readiness for change, guiding appropriate intervention and treatment planning.
1. History Taking :
- Substance Use History:
- Specific Substances: Which substances (alcohol, illicit drugs, prescription medications, nicotine, caffeine) have been used?
- Age of Onset: When did use begin for each substance?
- Pattern of Use: Frequency, quantity, route of administration (e.g., oral, inhaled, injected), duration of use.
- Periods of Abstinence: Any attempts to quit or reduce use? Duration? Reasons for relapse?
- Consequences of Use: Problems related to health, finances, legal issues, relationships, employment/education.
- Previous Treatment: Any prior detoxification, rehabilitation, or counseling? What was helpful/unhelpful?
- Family History of SUDs: Crucial genetic risk factor.
- Withdrawal History: History of withdrawal symptoms? Seizures? Delirium Tremens?
- Overdose History: Any past overdoses? How were they managed?
- Medical History:
- Current and past medical conditions (especially cardiac, hepatic, renal, neurological, infectious diseases like HIV/HCV).
- Medications (prescription, over-the-counter, herbal supplements).
- Allergies.
- Psychiatric History:
- Past and current mental health diagnoses (e.g., depression, anxiety, PTSD, bipolar, schizophrenia).
- Psychiatric hospitalizations, suicide attempts, self-harm.
- Medications for mental health conditions.
- Trauma history (important to specifically inquire about this).
- Social History:
- Living situation, support system (family, friends), marital/relationship status.
- Employment/educational status.
- Legal history.
- Financial stability.
- Spiritual/cultural considerations.
- Exposure to violence or trauma.
- Developmental History: Significant events, childhood experiences.
- Readiness to Change: Assess the patient's motivation for change, using techniques like Motivational Interviewing. What are their goals? What are perceived barriers?
2. Physical Examination Findings (Identify current effects and long-term complications):
- General Appearance: Signs of neglect, malnourishment, hygiene.
- Vital Signs: Tachycardia, hypertension, hypotension, hypothermia, hyperthermia (can indicate intoxication, withdrawal, or associated medical issues).
- Skin: Track marks (injection drug use), abscesses, cellulitis, jaundice, pallor, spider angiomas (liver disease), poor turgor (dehydration).
- Eyes: Pupillary changes (miosis for opioids, mydriasis for stimulants/withdrawal), nystagmus (alcohol, sedatives), scleral icterus.
- Nose: Septal perforation (cocaine sniffing).
- Mouth: Poor dentition, gingivitis, oral candidiasis (methamphetamine).
- Cardiovascular: Murmurs (endocarditis), peripheral edema.
- Respiratory: Diminished breath sounds, signs of aspiration.
- Abdomen: Hepatomegaly, ascites (liver disease).
- Neurological: Tremors, ataxia, gait disturbances, altered mental status, seizures, focal neurological deficits.
- Psychiatric: Agitation, anxiety, paranoia, hallucinations, delusions, anhedonia, depression.
3. Screening Tools (Brief, standardized instruments to identify potential SUDs):
- Universal Screening: Recommended for all adults and adolescents in healthcare settings.
- Common Tools:
- AUDIT (Alcohol Use Disorders Identification Test): 10-item self-report questionnaire for hazardous, harmful, and dependent alcohol consumption. Score of 8 or more often indicates problematic use.
- DAST (Drug Abuse Screening Test): 10 or 20-item self-report questionnaire for drug abuse. Similar to AUDIT but for drug use.
- CAGE-AID (Cut down, Annoyed, Guilty, Eye-opener; Adapted to Include Drugs): 4-item questionnaire, quick to administer. Two or more "yes" answers are significant.
- ASSIST (Alcohol, Smoking and Substance Involvement Screening Test): Developed by WHO, screens for a wide range of substances and provides a risk score.
- SBIRT (Screening, Brief Intervention, and Referral to Treatment): A comprehensive public health approach to early intervention for individuals with substance use disorders and those at risk. Involves screening, brief motivational intervention, and referral to treatment if needed.
4. Toxicology Screening (Objective laboratory tests):
- Urine Drug Screens (UDS): Most common. Detects presence of substances or their metabolites.
- Limitations:
- Detection Window: Varies widely by substance (e.g., cocaine 2-4 days, cannabis up to 30+ days for chronic users).
- False Positives/Negatives: Certain medications or foods can cause false positives (e.g., poppy seeds for opioids, ibuprofen for cannabis). Adulteration by patients is possible.
- Does not quantify: A positive result indicates presence, not amount or recency of use.
- Limitations:
- Blood Tests: More accurate for acute intoxication, can quantify levels. Used in emergency settings or for forensic purposes.
- Hair Follicle Testing: Can detect substance use over a longer period (up to 90 days). More expensive and less commonly used.
- Saliva Tests: Shorter detection window than urine, often used in workplace testing.
- Breathalyzer: Measures Blood Alcohol Content (BAC).
Nursing Diagnoses and Specific Nursing Interventions for SUDs
These diagnoses the guide the selection of targeted, evidence-based nursing interventions.
I. Common Nursing Diagnoses for Individuals with Substance Use Disorders
Here are some frequently encountered nursing diagnoses, categorized for clarity, along with their related factors and defining characteristics (as identified in the assessment):
- Risk for Injury
- Related Factors: CNS depressant/stimulant intoxication or withdrawal, impaired judgment, seizures, delusions/hallucinations, risk-taking behavior, altered motor coordination, suicide attempts.
- Defining Characteristics: (Observed or reported behaviors and symptoms from assessment, e.g., "patient reports history of falls during intoxication," "exhibits tremors and diaphoresis").
- Risk for Inadequate Fluid Volume / Inadequate Fluid Volume
- Related Factors: Diaphoresis, vomiting, diarrhea (withdrawal), inadequate fluid intake (intoxication), fever, gastrointestinal losses.
- Defining Characteristics: Dry mucous membranes, decreased skin turgor, decreased urine output, orthostatic hypotension, electrolyte imbalances.
- Disturbed Thought Processes / Acute Confusion
- Related Factors: Substance intoxication, alcohol withdrawal delirium (DTs), stimulant-induced psychosis, cognitive impairment from chronic use.
- Defining Characteristics: Disorientation, impaired memory, difficulty concentrating, paranoia, hallucinations, delusions, illogical thought patterns.
- Ineffective Coping
- Related Factors: Inadequate coping skills, unresolved grief/trauma, low self-esteem, maladaptive coping mechanisms (e.g., substance use), stressful life events.
- Defining Characteristics: Inability to meet basic needs, difficulty problem-solving, emotional lability, destructive behavior toward self or others, expressed inability to cope, substance use.
- Inadequate protein energy nutritional intake
- Related Factors: Anorexia (stimulants, withdrawal), nausea/vomiting, financial constraints, preoccupation with substance use, poor dietary choices, malabsorption.
- Defining Characteristics: Weight loss, muscle wasting, electrolyte imbalances, poor skin turgor, dull hair, lack of interest in food, abnormal lab values (e.g., low albumin).
- Sleep Deprivation / Disturbed Sleep Pattern
- Related Factors: Stimulant use, withdrawal from CNS depressants, anxiety, hyperarousal, nightmares, altered sleep-wake cycle.
- Defining Characteristics: Difficulty falling/staying asleep, daytime drowsiness, irritability, dark circles under eyes, frequent yawning, changes in mood/cognition.
- Compromised Family Coping / Dysfunctional Family Processes
- Related Factors: Substance use of a family member, enabling behaviors, codependency, lack of boundaries, ineffective communication patterns, financial strain.
- Defining Characteristics: Family expression of despair, anger, frustration, neglect of family roles, withdrawal from social interaction, denial, abuse (physical/emotional).
- Inadequate health Knowledge (regarding disease process, treatment, relapse prevention)
- Related Factors: Lack of exposure to information, misinterpretation of information, cognitive impairment, denial.
- Defining Characteristics: Verbalization of misinformation, inappropriate behaviors, failure to follow instructions, asking questions, lack of follow-through.
- Chronic Low Self-Esteem / Situational Low Self-Esteem
- Related Factors: Shame, guilt, repeated failures in past treatment, negative self-talk, stigma associated with SUDs, perceived lack of control.
- Defining Characteristics: Self-negating verbalizations, feelings of worthlessness, lack of eye contact, social withdrawal, self-destructive behavior.
- Risk for Infection
- Related Factors: Intravenous drug use (HIV, hepatitis, cellulitis, endocarditis), poor hygiene, malnutrition, compromised immune system, risky sexual behaviors.
- Defining Characteristics: (Not applicable as it's a risk diagnosis, but related factors and patient behaviors would indicate it).
II. Nursing Interventions
Interventions are tailored to the specific diagnosis and the patient's stage of recovery. They often involve a combination of physiological and psychosocial approaches.
A. Detoxification and Withdrawal Management
(Acute Phase - Often Requires Medical Oversight)
| Intervention | Detail/Rationale |
|---|---|
| 1. Safety and Monitoring (Priority 1) |
|
| 2. Pharmacological Management (MAT for Acute Withdrawal) |
|
| 3. Supportive Care |
|
B. Patient Education
(Ongoing Throughout All Phases)
| Area of Education | Detail/Rationale |
|---|---|
| 1. Disease Education |
|
| 2. Medication Education |
|
| 3. Relapse Prevention Strategies |
|
| 4. Harm Reduction (if appropriate) | Education on safer injection practices (if still using), safe sex, overdose prevention, naloxone use. |
C. Psychosocial Interventions
(Addressing Ineffective Coping, Low Self-Esteem, etc.)
| Intervention | Detail/Rationale |
|---|---|
| 1. Therapeutic Communication |
|
| 2. Coping Skills Training |
|
| 3. Self-Esteem Building |
|
| 4. Social Support and Community Resources |
|
| 5. Family Involvement (with patient consent) |
|
Pharmacological Treatments for SUDs
Pharmacological treatments for Substance Use Disorders (SUDs) are often referred to as Medication-Assisted Treatment (MAT). MAT combines medications with behavioral therapies and counseling to provide a "whole-person" approach to treatment. It has been shown to be more effective than either approach alone.
I. Medications for Alcohol Use Disorder (AUD)
A. Detoxification/Withdrawal Management (Acute Phase):
- Benzodiazepines (e.g., Chlordiazepoxide [Librium], Diazepam [Valium], Lorazepam [Ativan], Oxazepam [Serax]):
- Purpose: The first-line treatment for acute alcohol withdrawal. They act on GABA receptors to reduce hyperexcitability, prevent seizures, and alleviate symptoms like anxiety, tremors, and agitation.
- Nursing Considerations: Administered on a fixed schedule or symptom-triggered (e.g., using CIWA-Ar scale). Monitor for over-sedation, respiratory depression.
- Adjunctive Medications:
- Thiamine (Vitamin B1): Administered to prevent Wernicke-Korsakoff syndrome, a severe neurological disorder caused by thiamine deficiency common in chronic alcohol use. Often given before or with glucose-containing solutions.
- Folic Acid, Multivitamins: To address other nutritional deficiencies.
- Magnesium Sulfate: May be given to reduce seizure risk and correct electrolyte imbalances.
- Anticonvulsants (e.g., Carbamazepine, Valproic Acid): May be used for patients with a history of withdrawal seizures or those who cannot tolerate benzodiazepines.
- Beta-blockers (e.g., Atenolol): To manage hypertension and tachycardia, but do not prevent seizures or DTs.
B. Relapse Prevention (Post-Detoxification/Maintenance Phase):
- Naltrexone (Revia, Vivitrol):
- Mechanism: An opioid receptor antagonist. It blocks the euphoric and sedating effects of alcohol and reduces cravings.
- Forms: Oral (Revia - daily) and extended-release injectable (Vivitrol - monthly).
- Nursing Considerations: Do not initiate if patient is on opioids (will precipitate acute withdrawal). Monitor liver function, side effects (nausea, headache).
- Acamprosate (Campral):
- Mechanism: Believed to restore the balance between excitatory (glutamate) and inhibitory (GABA) neurotransmitters, reducing craving and discomfort (e.g., anxiety, dysphoria) associated with protracted withdrawal.
- Nursing Considerations: Taken three times daily. Excreted renally, so contraindicated in severe renal impairment. Side effects include diarrhea, nausea.
- Disulfiram (Antabuse):
- Mechanism: Inhibits acetaldehyde dehydrogenase, an enzyme involved in alcohol metabolism. If alcohol is consumed while taking disulfiram, it leads to a highly unpleasant reaction (flushing, throbbing headache, nausea, vomiting, chest pain, dizziness, vertigo). This creates a strong deterrent.
- Nursing Considerations: Patient must be fully informed of the severe consequences of drinking. Avoid all alcohol-containing products (mouthwash, hand sanitizer, cologne, some foods). Requires informed consent. Monitor liver function.
II. Medications for Opioid Use Disorder (OUD)
A. Detoxification/Withdrawal Management (Acute Phase):
- Buprenorphine (Subutex, often combined with naloxone as Suboxone):
- Mechanism: A partial opioid agonist. It binds to opioid receptors but produces a weaker effect than full agonists (like heroin or fentanyl). This reduces withdrawal symptoms and cravings without producing the same high.
- Nursing Considerations: Can only be started after the patient is in mild to moderate withdrawal (COWS score > 8-12) to avoid precipitating acute withdrawal (due to its partial agonist/antagonist properties). Administered sublingually.
- Clonidine:
- Mechanism: An alpha-2 adrenergic agonist. It reduces the autonomic symptoms of opioid withdrawal (e.g., hypertension, tachycardia, sweating, anxiety, muscle aches) but does not address cravings or euphoria.
- Nursing Considerations: Monitor blood pressure closely for hypotension. Does not prevent "cold turkey" withdrawal entirely.
- Methadone:
- Mechanism: A full opioid agonist. It replaces the illicit opioid, preventing withdrawal symptoms and cravings. It has a long half-life, allowing for once-daily dosing.
- Nursing Considerations: Administered in highly regulated opioid treatment programs (OTPs). Requires careful titration. Risk of respiratory depression, cardiac arrhythmias (QT prolongation).
B. Relapse Prevention (Maintenance Phase):
- Buprenorphine/Naloxone (Suboxone, Zubsolv, Bunavail; also injectable long-acting forms like Sublocade, Probuphine implant):
- Mechanism: Buprenorphine for maintenance, naloxone is added to deter IV abuse (if injected, naloxone precipitates withdrawal).
- Nursing Considerations: Prescribed by DATA 2000 waivered providers. Continued monitoring for diversion, side effects.
- Methadone:
- Mechanism: As described above, also serves as a maintenance medication to stabilize individuals in recovery.
- Nursing Considerations: Long-term treatment in OTPs.
- Naltrexone (Vivitrol injectable, Revia oral):
- Mechanism: An opioid receptor antagonist. Blocks the effects of any ingested opioids, preventing euphoria and reducing cravings.
- Nursing Considerations: Patient must be fully opioid-free for 7-14 days before initiation to avoid precipitating acute, severe withdrawal. This makes it challenging for some patients. Monitor liver function.
III. Medications for Stimulant Use Disorder (Cocaine, Methamphetamine)
- No FDA-approved medications specifically for stimulant use disorder.
- Treatment focuses on behavioral therapies.
- Off-label medications: May be used to manage co-occurring mental health disorders (e.g., antidepressants for depression) or to address specific withdrawal symptoms (e.g., benzodiazepines for severe agitation/anxiety).
- Emerging research: Exploring various medications (e.g., bupropion, naltrexone, disulfiram, topiramate) with mixed results, but none are standard of care.
IV. Medications for Cannabis Use Disorder
- No FDA-approved medications.
- Treatment primarily behavioral.
- Off-label medications: May be used to manage withdrawal symptoms (e.g., dronabinol for sleep/appetite, gabapentin for anxiety/sleep, antidepressants for mood).
V. Medications for Sedative/Hypnotic Use Disorder (Benzodiazepines, Barbiturates)
A. Detoxification/Withdrawal Management (Acute Phase):
- Gradual Tapering of the Benzodiazepine: The safest and most effective method. Slowly reduce the dose over weeks to months, depending on the dose and duration of use.
- Cross-Tapering to a Long-Acting Benzodiazepine (e.g., Diazepam, Clonazepam): Allows for smoother dose reductions and fewer interdose withdrawals.
- Nursing Considerations: Abrupt cessation can be life-threatening (seizures, delirium). Close monitoring for withdrawal symptoms, seizure precautions.
VI. Medications for Co-occurring Mental Health Disorders
- Antidepressants (SSRIs, SNRIs, etc.): For depression, anxiety disorders.
- Mood Stabilizers (Lithium, Valproic Acid): For bipolar disorder.
- Antipsychotics: For psychotic disorders (e.g., schizophrenia) or stimulant-induced psychosis.
- Medications for PTSD (SSRIs, Prazosin): To manage trauma-related symptoms.
- Nursing Considerations: These medications should be initiated and carefully monitored by a psychiatrist. Important to consider potential interactions with substances of abuse and the risk of misuse.
ALCOHOLISM
Alcoholism is a chronic condition characterized by excessive and prolonged alcohol consumption, leading to severe physical, social, and mental adverse effects, and an increased physical and social dependency on alcohol.
Key Terms and Definitions:
- Drug (Substance): Any chemical agent that, once ingested, can cause physiological and psychological changes.
- Alcoholic: An individual who excessively consumes alcohol, leading to mental, social, physical, and psychological problems.
- Substance Intoxication: A reversible, substance-specific syndrome that develops due to recent ingestion or exposure to a drug.
- Alcohol Intoxication: A temporary mental disturbance following heavy drinking, where blood alcohol levels are high enough to affect activity, mood, and consciousness.
- Tolerance: The need for increasing amounts of a drug to achieve the same effect previously obtained with a lower dose.
- Dependency: A compulsion to continuously take a drug to experience its effects and avoid the discomfort of its absence. This can be physical (bodily response) or psychological.
- Addiction: A psychological and physical inability to stop consuming a drug despite it causing psychological and physical harm, characterized by continued use despite negative consequences.
- Misuse: Incorrect, excessive, or non-therapeutic use of mind-altering substances.
Causes of Alcohol Abuse:
- Availability: Easy access to alcohol and societal acceptance of drinking (e.g., at social gatherings).
- Genetic Factors: A family history of excessive drinking suggests a genetic predisposition.
- Poor Coping Strategies: Individuals struggling with stress may resort to alcohol as a coping mechanism.
- Psychiatric Disorders: Co-occurring conditions like depressive, anxiety, or phobic disorders can lead to alcohol abuse.
- Social Disorders: Factors such as isolation, unemployment, loss, bereavement, or injustice.
- High-Risk Groups: Includes those with chronic physical illnesses, business executives, traveling salespersons, industrial workers, hostel students, and military personnel.
- Age: Most common between late adolescence and early adulthood.
Process of Alcoholism:
The development of alcoholism often follows a progression:
- Experimental Stage: Initial consumption due to peer pressure, influences, or curiosity.
- Recreational Stage: Enjoyment of alcohol during weekends or holidays. In small amounts, it may relieve tension, relax the mind, or promote well-being.
- Compulsive Stage: Regular, heavy drinking to achieve pleasure or avoid withdrawal discomfort.
Stages of Alcoholism:
The text outlines distinct stages:
- Early Stage:
- Increased Tolerance: Needing more alcohol for the desired effect.
- Blackouts: Inability to recall events while intoxicated.
- Preoccupation: Constant thoughts about drinking.
- Middle Stage:
- Loss of Control: Inability to limit amount or frequency of drinking.
- Cycles of Abstinence: Brief periods without alcohol, followed by obsessive drinking.
- Chronic Stage:
- Low Tolerance: Getting drunk on small amounts.
- Prioritizing Alcohol: Alcohol takes precedence over family or job; willingness to lie, beg, borrow, or steal for supply.
Types of Drinkers:
- Mild Drinkers: Rarely and occasionally consume small amounts, or large amounts infrequently, with minimal problems.
- Moderate Drinkers: Consume in moderation, without excess, generally avoiding significant health issues.
- Problem Drinkers: Consume large amounts daily, often with high concentrations, leading to impaired health, mental distress, family disruption, loss of reputation, and poor performance.
Effects and Complications of Alcohol:
A. Physical or Medical Effects:
- Hepatitis and Liver Cirrhosis
- Pancreatitis
- Peptic Ulcers and Gastritis
- Cardiomyopathies and Heart Failure
- Epileptic-like Fits (RUM Fits - alcohol withdrawal seizures)
- Tuberculosis
- Weight Loss
- Alcoholic Dementia
- Anemia
- Malnutrition
- Lowered Immunity
B. Psychiatric Effects:
- Depression
- Pathological Intoxication: Maladaptive behavioral effects (e.g., fighting, impaired judgment, slurred speech, mood changes, irritability, impaired attention).
- Delirium Tremens (DTs): Severe withdrawal syndrome with confusion, hallucinations, and autonomic instability.
- Alcoholic Hallucinosis: Vivid hallucinations shortly after reducing or stopping alcohol.
- Alcoholic Psychosis: Psychotic disorder resembling paranoid schizophrenia (delusions, hallucinations, primary mental function impairment) after prolonged, heavy drinking.
- Alcohol Amnestic Disorder: Impairment in short and long-term memory, disorientation, and confabulation.
- Alcoholic Dementia: Chronic organic mental disorder resulting in irreversible memory and orientation impairment.
- Suicide
- Anxiety
- Paranoia: Persecutory ideation and self-hate.
- Morbid or Pathological Jealousy: Irrational jealousy, often directed at a partner.
- Hallucinations
- Wernicke’s Encephalopathy: Acute deficiency of Vitamin B1 (Thiamine) in alcoholics, causing neurological symptoms.
- Korsakoff Syndrome: Gradual depletion of thiamine, leading to severe memory problems and confabulation.
C. Social Problems:
- Decreased work performance and productivity (due to chronic absenteeism).
- Family problems (e.g., divorce).
- Increased accidents (e.g., drunk driving).
- Legal effects (e.g., rape, theft).
- Violence and aggression.
Diagnosis of Alcoholism:
- History Taking: Comprehensive assessment of upbringing, family background, duration of abuse, etc.
- Clinical Presentation: Observable signs like curly hair, swollen cheeks, red lips, poor hygiene, etc.
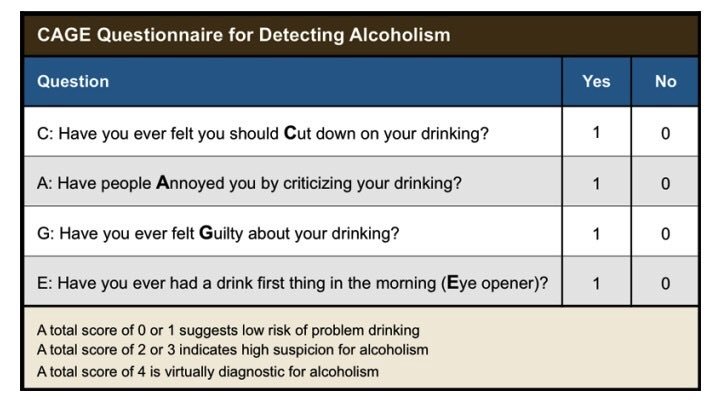
- CAGE Questionnaire: A screening tool:
- C - Have you ever felt you should Cut down on your drinking?
- A - Have people Annoyed you by criticizing your drinking?
- G - Have you ever felt Guilty about your drinking?
- E - Have you ever had an Eye-opener first thing in the morning to get rid of a hangover or calm your nerves?
- Interpretation: Two or more "yes" answers are highly suggestive of alcoholism.
Concentration of Alcohol in Blood and Effects:
- 80-150 mg/100ml: Intoxication
- 150-300 mg/100ml: Fatal (high risk of death)
- 300-500 mg/100ml: Very Fatal (extremely high risk of death)
- 500 mg/100ml and above: Leads to death
- Note: These effects can vary based on individual tolerance.
Management of Alcoholism:
A. Aims of Management:
- Detoxify the patient (in acute stages).
- Improve social relationships and support.
- Develop confidence and ability to change.
- Identify reasons for change.
- Develop alternative activities.
- Learn to prevent relapse.
B. Admission:
- Hospitalization is crucial to prevent alcohol access; often 6-8 weeks initially.
- Admit to a psychiatric hospital in a well-lit, quiet, open room to reduce fear and illusions.
- Establish a good nurse-patient relationship.
- Remove potentially harmful objects to prevent self-harm.
- Keep the bed dry, clean, and warm due to possible incontinence.
- Monitor vital signs every 15 minutes initially, including physical and mental behavior.
- Investigations: Urine for sugar, blood for hemoglobin level and sugars, blood alcohol level.
C. Medication:
- Minor Tranquilizers (Anxiolytics): Librium (chlordiazepoxide) and Diazepam (Valium) parenterally for anxiety, insomnia, agitation, and tremors (these are benzodiazepines, crucial for withdrawal management).
- Anticonvulsants: For withdrawal seizures ("rum fits").
- Vitamins: Plenty of B vitamins (especially Thiamine B1, B6, B12 – 100-300mg BID for 7 days), B complex, and Vitamin C.
- Antacids: To relieve gastritis.
- Fluid & Electrolyte Correction: Intravenous infusions, fluid balance chart.
- Disulfiram (Antabuse): Administered under close supervision. It causes severe adverse reactions (nausea, vomiting, headache, palpitations, blurred vision, hypotension, dyspnea) if alcohol is consumed. Initial dose 1g, tapering down to 0.1g for maintenance (up to a year).
- Aversion Therapy (Apomorphine): Injectable emetic; causes vomiting when alcohol is smelled. The text notes this is discouraged.
- Yeast Tablets: Twice daily to induce appetite.
- Stemetil (Prochlorperazine) / Avomine (Promethazine): 5-10mg to control vomiting.
- Sedation: May be required.
- Avoid Barbiturates: Alcoholics can easily become addicted to them.
D. General Nursing Care:
- Treat Associated Conditions: Address malnutrition, vitamin deficiencies, hallucinations, delirium, gastritis, or liver diseases.
- Nutrition: Small, frequent, nutritious, and appetizing meals.
- Hygiene: Oral care, general body, and bed hygiene.
- Nurse-Patient Relationship: Acceptance by the nurse is essential to encourage socialization and participation, reducing inferiority and low self-esteem.
- Psychiatric Social Workers: Involvement in addressing social problems.
- Religious Commitment: Encouraged.
- Familial Therapy: Encouraged to help the patient stay sober.
- Social Circle Change: Encourage changing friends and associates to remove triggers.
- Alcoholics Anonymous (AA): Prepare the patient for AA, a self-help group where ex-addicts provide mutual support and guidance for sobriety.
- Discharge Planning: Plan for the patient's discharge and resettlement into the community.
Therapeutic Modalities for SUDs
Therapeutic modalities form the backbone of behavioral treatment for Substance Use Disorders (SUDs). They address the psychological, social, and behavioral aspects of addiction, helping individuals develop coping strategies, improve interpersonal relationships, and maintain abstinence.
I. Individual Therapies
Individual therapy provides a private and confidential setting for patients to explore their substance use, underlying issues, and recovery goals with a trained therapist.
- A. Cognitive Behavioral Therapy (CBT):
- Core Principle: Based on the idea that thoughts, feelings, and behaviors are interconnected. CBT helps patients identify and change problematic thinking patterns and behaviors that contribute to substance use.
- Techniques:
- Identifying Triggers: Recognizing situations, thoughts, or feelings that lead to craving and substance use.
- Coping Skills Training: Developing healthy ways to manage stress, cravings, and high-risk situations (e.g., relaxation techniques, distraction, problem-solving).
- Relapse Prevention: Learning to anticipate and cope with potential setbacks, developing a plan for managing a "slip."
- Cognitive Restructuring: Challenging and changing irrational or unhelpful thoughts (e.g., "I can't cope without alcohol").
- Role in SUDs: Highly effective for many SUDs, helping patients develop self-control and build skills for long-term recovery.
- B. Dialectical Behavior Therapy (DBT):
- Core Principle: Developed for individuals with severe emotion dysregulation (originally for Borderline Personality Disorder), but highly effective for SUDs, especially when co-occurring with trauma or personality disorders. Emphasizes balancing acceptance and change.
- Skills Modules:
- Mindfulness: Learning to be present and aware without judgment.
- Distress Tolerance: Developing strategies to cope with intense emotions and crises without resorting to substance use or other maladaptive behaviors.
- Emotion Regulation: Learning to identify, understand, and manage intense emotions.
- Interpersonal Effectiveness: Improving communication skills and building healthier relationships.
- Role in SUDs: Helps patients manage intense cravings, cope with emotional triggers, and develop healthier interpersonal boundaries.
- C. Motivational Interviewing (MI):
- Core Principle: A person-centered, directive method for enhancing intrinsic motivation to change by exploring and resolving ambivalence.
- Key Elements (OARS):
- Open-ended questions: Encourage detailed responses.
- Affirmations: Recognize patient strengths and efforts.
- Reflective listening: Show understanding and empathy.
- Summaries: Consolidate understanding and highlight key points.
- Role in SUDs: Often used as an initial intervention to help patients move from precontemplation/contemplation to preparation/action stages of change, increasing readiness for treatment. Nurses frequently use MI techniques.
- D. Psychodynamic Therapy:
- Core Principle: Explores unconscious conflicts, past experiences (especially childhood trauma), and relationship patterns that may contribute to substance use.
- Role in SUDs: May be useful for individuals whose substance use is deeply rooted in unresolved psychological issues, often as a long-term approach.
II. Group Therapies
Group therapy provides a supportive environment where individuals can share experiences, receive feedback, and learn from peers in recovery.
- A. Psychoeducational Groups:
- Focus: Provide information about SUDs, relapse prevention, coping skills, and healthy lifestyle choices.
- Role in SUDs: Informative and foundational for understanding the disease and recovery process.
- B. Process-Oriented Groups:
- Focus: Explore interpersonal dynamics, emotions, and behaviors within the group setting. Members provide support and challenge each other.
- Role in SUDs: Helps individuals develop social skills, address isolation, and practice new behaviors in a safe environment.
- C. Relapse Prevention Groups:
- Focus: Utilize CBT principles to identify high-risk situations, develop coping strategies, and review relapse warning signs.
- Role in SUDs: Critical for maintaining long-term abstinence by equipping patients with proactive strategies.
III. 12-Step Programs
(e.g., Alcoholics Anonymous (AA), Narcotics Anonymous (NA))
- Core Principle: A mutual-help, peer-led program based on spiritual principles (though not necessarily religious). Emphasizes abstinence, working through the 12 steps, making amends, and service to others.
STEPS OF ALCOHOLICS ANONYMOUS:
- We admitted we were powerless over alcohol – that our lives had become unmanageable. AA firmly believes that individuals cannot overcome alcoholism on their own. They are unable to exercise willpower or personal strength that could prevent them from drinking
- Came to believe that a Power greater than ourselves could restore us to sanity. Alcoholics Anonymous is based on the belief in a higher power. For some, this higher power may be God; for others, it may be a belief in the universe itself. The point is that recovery begins, in part, by looking to an entity greater than yourself.
- Made a decision to turn our will and our lives over to the care of God as we understood Him.
- Made a searching and fearless moral inventory of ourselves. During this step, many participants make a list of poor decisions or character flaws. They outline hurt they caused to others, as well as feelings, like fear and guilt, that motivated some of their past actions. Once the individual has acknowledged these issues, the issues are less likely to serve as triggers to future alcohol abuse.
- Admitted to God, to ourselves and to another human being the exact nature of our wrongs. As AA members work this step, they sit down with someone – often their sponsor – and confess everything they identified in Step 4. This step requires the recovering individual to put aside their ego and pride to acknowledge shameful past behavior. The step is also empowering, as the alcoholic no longer has to hide behind guilt and lies.
- Were entirely ready to have God remove all these defects of character. In this step, the recovering alcoholic acknowledges that he or she is ready to have a higher power – again, whatever that may be – take away the moral shortcomings identified in
- Humbly asked Him to remove our shortcomings. This step requires the person to focus on the positive aspects of his or her character – humility, kindness, compassion and a desire for change – as well as step away from the negative defects that have been identified.
- Made a list of all persons we had harmed, and became willing to make amends to them all. During this step, recovering alcoholics write down a list of all the people they have hurt. Often, this list includes people they hurt during their active alcoholism; however, it may go back further to include anyone they have hurt throughout their entire lives
- Made direct amends to such people wherever possible, except when to do so would injure them or others. Paired with Step 8, Step 9 gives recovering alcoholics the opportunity to make things right with those they have hurt. One’s sponsor can be a big source of help during this process, helping the recovering alcoholic to determine the best way to go about making amends.
- Continued to take personal inventory and when we were wrong promptly admitted it. Linked to Step 4, this step involves a commitment to continue to keep an eye out for any defects of character. It also involves a commitment to readily admit when one is wrong, reinforcing humility and honesty.
- Sought through prayer and meditation to improve our conscious contact with God as we understood Him, praying only for knowledge of His will for us and the power to carry that out. Step 11 commits the recovering alcoholic to continued spiritual progress. For some, this may mean reading scripture every morning. For others, it may mean a daily meditation practice. Alcoholics Anonymous doesn’t have stringent rules on what form spiritual growth takes. It simply involves a commitment to take time to reassess one’s spiritual and mental state.
- Having had a spiritual awakening as the result of these steps, we tried to carry this message to alcoholics and to practice these principles in all our affairs practice these principles in all our affairs. The final step involves helping others and serves as motivation for many to become sponsors themselves. By going through the 12 steps, individuals have a major internal shift and part of that shift is a desire to help others.
IV. Family Therapy
- Core Principle: Recognizes that SUDs affect the entire family system. Focuses on improving family communication, establishing healthy boundaries, and addressing enabling or dysfunctional patterns.
- Approaches:
- Family Behavioral Therapy (FBT): Focuses on teaching family members communication skills, problem-solving, and contingency management to support the patient's recovery.
- Multisystemic Therapy (MST): Intensive, family- and community-based treatment for adolescents with serious substance use and other behavioral problems.
- Role in SUDs: Essential for healing family dynamics, creating a supportive home environment, and preventing relapse. It also provides support and education for family members, who often suffer secondary effects of the SUD.
V. Other Emerging Therapies
- Mindfulness-Based Relapse Prevention (MBRP): Integrates mindfulness practices with CBT for relapse prevention.
- Contingency Management (CM): Uses positive reinforcement (e.g., vouchers, prizes) to reward abstinence and treatment adherence. Highly effective, especially for stimulant use, but can be resource-intensive.
VI. Nursing Role in Therapeutic Modalities
- Referral: Identify appropriate therapeutic modalities based on patient needs and preferences, and facilitate referrals.
- Support: Encourage participation in therapy and support groups.
- Integration: Reinforce therapeutic concepts (e.g., coping skills, trigger identification) in daily interactions with patients.
- Psychoeducation: Provide basic information about different therapy types and what to expect.
- Advocacy: Advocate for access to these vital services.
I need these notes because they’re very good for teaching diploma students .
Actually The whole outline for pharmacologyIII
You can always find them here waiting
I need a detailed specific nursing intervention for a patient with narcotic abuse
Am greatiful for this
Welcome, anything you wish we can improve?
Very easy to understand,,, great thanks,,,,
thanks for the good work here may God bless you
am requesting these notes ,thank you .
Great work indeed
I like u man thank you
Please some past paper questions
a vital job for student nurses and midwives