
Suturing
Suturing is the process of closing a wound by stitching the wound edges together using a surgical needle and thread.
It is a fundamental technique in wound management and surgical procedures to facilitate healing, prevent infection, and restore tissue integrity.
Purpose of Suturing
The primary goals of suturing are:
 To approximate wound edges until healing occurs. To speed up the wound healing process by stabilizing the tissue. To minimize the risk of infection by reducing the open surface area. To improve cosmetic outcomes and minimize scarring. To provide additional support in high-tension areas or deep wounds.
To approximate wound edges until healing occurs. To speed up the wound healing process by stabilizing the tissue. To minimize the risk of infection by reducing the open surface area. To improve cosmetic outcomes and minimize scarring. To provide additional support in high-tension areas or deep wounds.
Types of Sutures
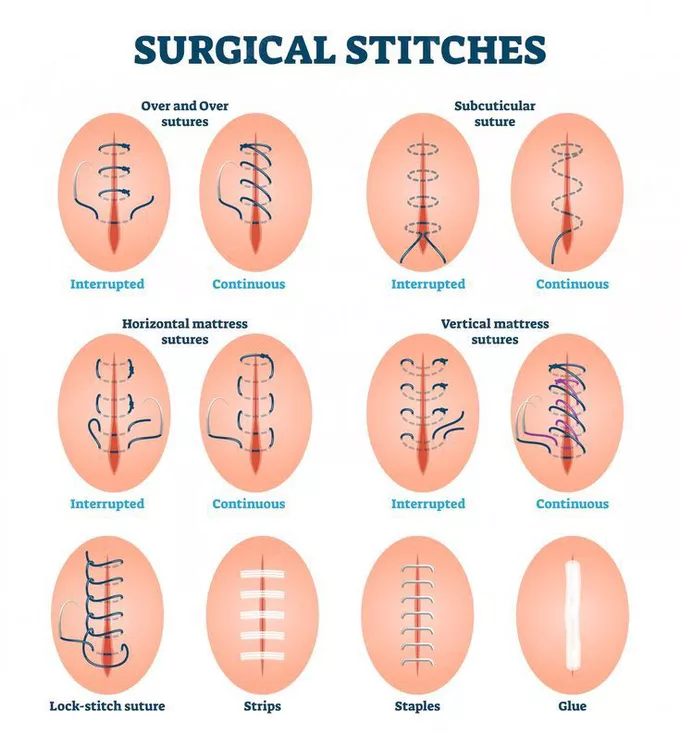
Sutures are broadly categorized into interrupted and continuous sutures.
1. Interrupted Sutures
- In interrupted suturing, each stitch is placed individually and tied separately.
- This is the most commonly used wound closure technique.
- The individual stitches are not connected, reducing the risk of wound dehiscence if one stitch fails.
Advantages:
 Easy to place.
Easy to place.
High tensile strength.
Individual stitches can be removed if infection occurs without affecting the entire closure.
 Disadvantages:
Disadvantages:
 Takes more time to place compared to continuous sutures.
Takes more time to place compared to continuous sutures.
Requires more suture material.
Each knot increases the risk of infection.
2. Continuous Sutures
- A single thread runs through the wound in a series of stitches and is tied only at the beginning and end.
- The stitches are connected, making it faster for long wounds or surgical incisions.
Advantages:
Faster than interrupted sutures.
Requires less suture material.
Distributes tension evenly along the wound.
Disadvantages:
If the suture breaks, the entire closure may fail.
Increased risk of dehiscence in high-tension areas.
Retention Sutures:
These are large interrupted sutures placed in addition to standard skin sutures.
- They support deep incisions, particularly in obese patients or high-risk wounds where dehiscence is likely.
- Often reinforced with rubber tubing to prevent the sutures from cutting into the skin.
- Retention sutures are typically removed after 14–21 days (longer than regular sutures).
Suturing Patterns
Based on the pattern of suturing, stitches can be classified as:
 Suturing Technique Tip: Each suture should be placed as deep as it is wide, and the distance between the sutures should be equal to the depth and width of the wound to ensure proper healing.
Suturing Technique Tip: Each suture should be placed as deep as it is wide, and the distance between the sutures should be equal to the depth and width of the wound to ensure proper healing.

Suture Materials
A suture material is the thread used to stitch a wound.
These materials vary in absorption, strength, and application.
Suture materials are classified into:
1. Absorbable Sutures
Absorbable sutures naturally break down and are absorbed by the body over time.
Advantages:
No need for suture removal.
Ideal for internal tissues (e.g., intestines, muscles, and subcutaneous tissues).
Available in multiple sizes (ranging from 0000000 to No. 5).
Disadvantages:
May cause an inflammatory reaction as they degrade.
Not suitable for long-term wound support.
Types of Absorbable Sutures
2. Non-Absorbable Sutures
Non-absorbable sutures do not dissolve and need to be manually removed once the wound has healed.
Advantages:
High tensile strength – they do not easily break.
Minimal tissue reaction, reducing inflammation.
Can be used for ligatures to tie off blood vessels.
Disadvantages:
Requires removal after healing.
Can cause irritation if left in place too long.
Common Non-Absorbable Suture Materials
 Ligature (Tie Sutures):
Ligature (Tie Sutures):
A ligature is a free piece of suture material used to tie off blood vessels that have been clamped with artery forceps to prevent bleeding.
Suture Removal Guidelines
The time for removing sutures varies depending on the wound location and type.
Nursing Considerations in Suturing
- Choose the appropriate suture material based on wound type, location, and required tensile strength.
- Use absorbable sutures for internal tissues to avoid the need for removal.
- Use non-absorbable sutures for skin closure, ensuring proper follow-up for suture removal.
- Place sutures evenly to distribute tension and prevent scarring.
- Monitor for infection (redness, swelling, pus formation) and remove affected sutures if needed.
- Ensure wound edges are well-approximated but not overly tight to avoid necrosis.


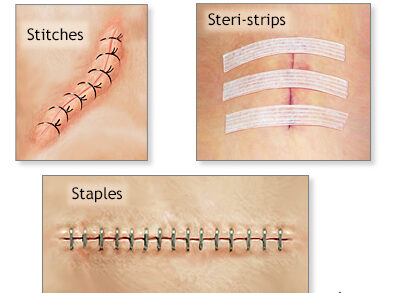
Clips (Metal Sutures) in Wound Closure
Clips, also known as metal sutures or surgical staples, are used to close the skin after a surgical procedure or deep wound.
Unlike traditional sutures, clips provide a fast, secure, and uniform wound closure, minimizing tissue trauma.
Purpose of Clips in Wound Closure
The primary objectives of using clips are similar to those of suturing with stitches, including:
To approximate wound edges until healing occurs. To speed up wound closure and healing. To reduce the risk of infection by minimizing handling. To provide a strong and secure closure, especially for long surgical incisions. To improve cosmetic outcomes by minimizing scarring. To reduce operation time compared to conventional suturing.
Equipment Required for Clip Removal
In addition to standard equipment for dressing a septic wound, the following specialized instruments are required for removing clips:
Procedure for Removing Clips
Pre-Procedure Preparation
 Explain the procedure to the patient to gain cooperation and reduce anxiety.
Explain the procedure to the patient to gain cooperation and reduce anxiety. Gather and organize all necessary equipment.
Gather and organize all necessary equipment. Position the patient comfortably and drape appropriately for privacy.
Position the patient comfortably and drape appropriately for privacy. Protect the bedding with a rubber sheet and cover to prevent contamination.
Protect the bedding with a rubber sheet and cover to prevent contamination. Remove the old dressing and discard it properly.
Remove the old dressing and discard it properly.
Clip Removal Procedure
Clean the wound using an antiseptic solution, starting from the cleanest area to the most contaminated part. Place a sterile gauze pad near the wound to collect removed clips. Hold the clip removal forceps in the right hand and the dissecting forceps in the left hand. Insert the lower blade of the clip remover under the center of the clip. Use the dissecting forceps to hold the clip in place as the removal forceps are squeezed. Gently press the forceps together – this action bends the clip outward, disengaging it from the skin.
Gently press the forceps together – this action bends the clip outward, disengaging it from the skin. Carefully remove the clip and place it on the sterile gauze.
Carefully remove the clip and place it on the sterile gauze. Repeat the process until all clips are removed.
Repeat the process until all clips are removed. Apply iodine or antiseptic to the puncture sites to prevent infection.
Apply iodine or antiseptic to the puncture sites to prevent infection. Dress the wound if necessary and secure the dressing with adhesive tape or a bandage. Ensure patient comfort and adjust their position as needed. Document the procedure, noting the appearance of the scar, wound healing progress, and any complications. Dispose of all used materials properly and return reusable instruments for sterilization.
Dress the wound if necessary and secure the dressing with adhesive tape or a bandage. Ensure patient comfort and adjust their position as needed. Document the procedure, noting the appearance of the scar, wound healing progress, and any complications. Dispose of all used materials properly and return reusable instruments for sterilization.
Post-Procedure Care and Monitoring
Assess the wound for signs of infection or delayed healing. Monitor for bleeding or wound dehiscence (reopening of the wound). Advise the patient to avoid excessive movement that could stress the healing wound. Provide pain relief if needed. Instruct the patient on proper wound care and when to seek medical attention.
Clinical Appearance of the Wound Bed
The appearance of the wound bed provides insight into healing progress and potential complications.