

STYE (HORDEOLUM)
A stye, also known as a hordeolum, is a localized infection of the hair follicle or the oil-producing (sebaceous) or sweat glands in the eyelid.
A stye, or hordeolum, is a localized, painful bacterial infection or inflammation of the glands or hair follicles at the edge of the eyelid.
Commonly caused by Staphylococcus aureus.
It often results from Staphylococcus aureus infection and can occur either externally (on the lid margin) or internally (within the eyelid).
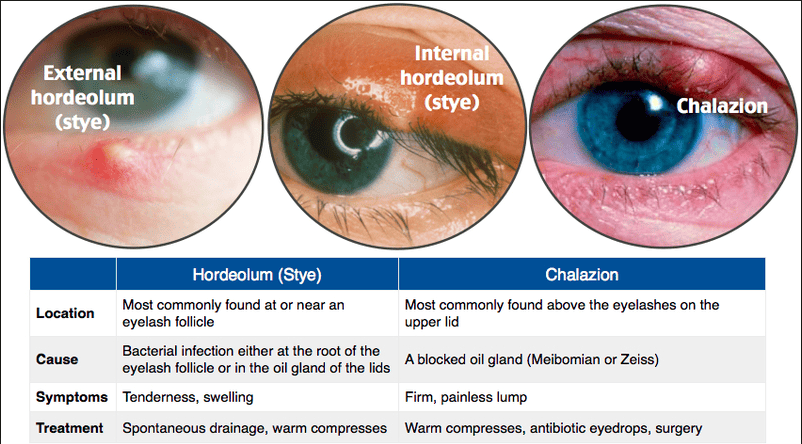
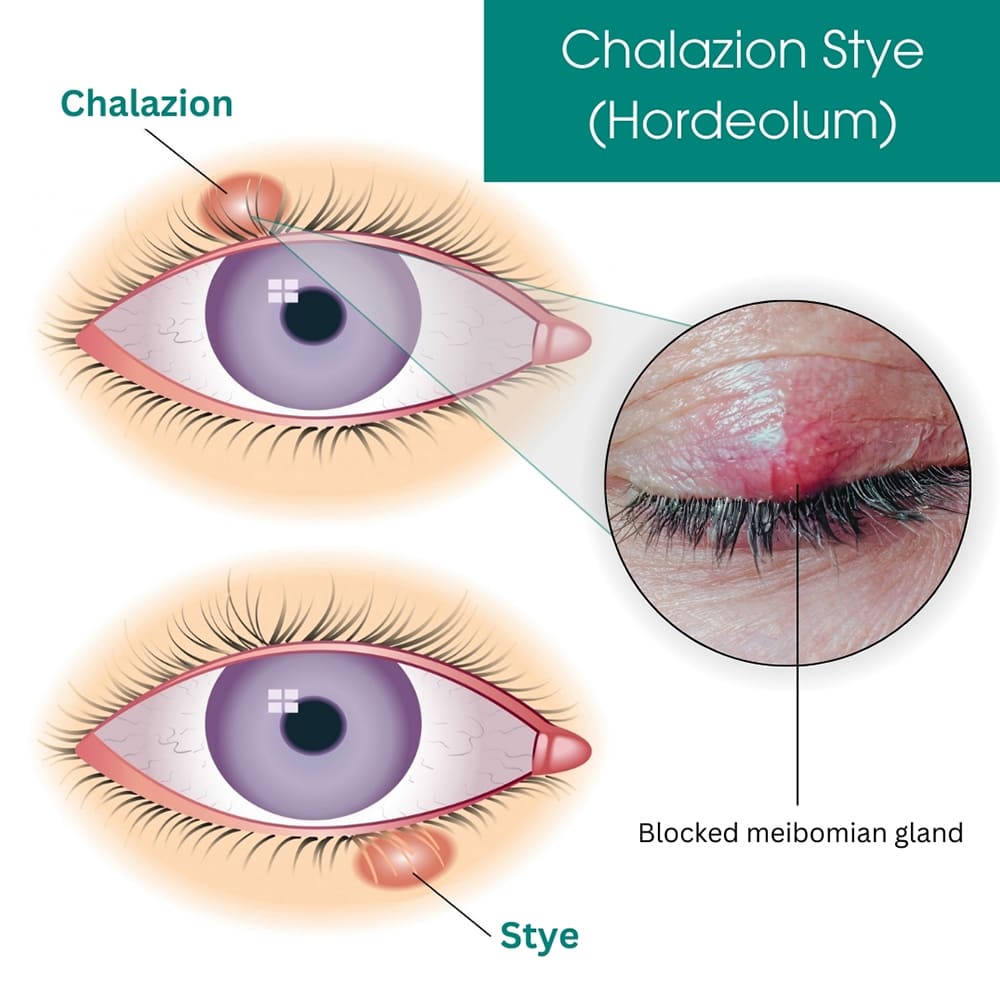
Types of Stye
1. Internal Hordeolum: Affects the Meibomian glands, which are sebaceous glands located within the eyelid.
Clinical Characteristics:
- The infection occurs deeper within the eyelid, often making it more painful and tender.
- Swelling may involve the entire eyelid.
- The internal stye can sometimes evolve into a chalazion if it becomes chronic and non-infectious.
2. External Hordeolum: Involves the glands of Zeis (sebaceous glands) or Moll glands (sweat glands) at the base of the eyelash follicle.
Clinical Characteristics:
- Appears as a small, red, painful lump resembling a pimple on the edge of the eyelid.
- Usually less painful than an internal hordeolum.
- Often associated with localized swelling and redness around the affected area.
Causes of Stye Formation
- Bacterial Infection: Most commonly caused by Staphylococcus aureus.
- Blocked Glands: Blockage in the sebaceous glands (Meibomian, Zeis, or Moll glands) can trigger inflammation.
- Poor Eyelid Hygiene: Failure to remove makeup or debris from the eyelid margins.
- Contact Lens Misuse: Wearing lenses without proper cleaning or disinfection can introduce bacteria.
- Pre-existing Conditions: Conditions such as blepharitis, rosacea, or seborrheic dermatitis increase susceptibility.
- Immune System Deficiency: Reduced immunity can predispose individuals to bacterial infections.
Clinical Features
Early Symptoms:
- Mild itching and discomfort in the affected area.
- A sensation of fullness or heaviness in the eyelid.
Progressive Signs:
- Pain: Localized tenderness and pain, especially on palpation.
- Redness: Visible inflammation and redness at the eyelid margin or deeper within the eyelid.
- Swelling: Puffy, swollen eyelid, which may extend to the surrounding areas.
- Pus Formation: Formation of a yellowish, fluid-filled pustule near the edge of the eyelid.
- Soreness: Persistent irritation and soreness over the affected site.
Advanced Symptoms:
- Drainage of Fluid: Spontaneous rupture may release yellowish or white pus, leading to symptom relief.
- Visual Obstruction: Swelling may partially block vision in severe cases.
Management of Stye
1. General Care
Avoid Rubbing or Touching the Eye:
- Rubbing can introduce additional bacteria and exacerbate the infection.
- Rationale: Prevents spreading the infection to other areas of the eyelid or eye.
Warm Compresses:
- Apply a warm or hot compress (clean cloth dipped in warm water) for 10–15 minutes, 3–4 times a day.
- Rationale: Encourages drainage of pus, relieves pain, and reduces swelling.
2. Medications
Antibiotic Eye Ointments:
- Tetracycline 1% eye ointment applied 2–4 times daily until 2 days after the symptoms subside.
- Rationale: Reduces bacterial load, speeds up healing, and prevents further spread of infection.
Analgesics:
- Oral pain relievers like ibuprofen or paracetamol for pain relief.
- Rationale: Helps manage discomfort and swelling.
3. Eyelash Removal
- Removal of loose or infected eyelashes may be performed by a healthcare provider.
- Rationale: Prevents recurrent infections by removing the source of blockage or bacterial growth.
4. Hygiene Practices
- Clean the eyelid regularly using a sterile saline solution or lid-cleaning wipes.
- Avoid sharing towels, makeup, or other personal items to prevent the spread of bacteria.
5. Lifestyle Modifications
- Maintain proper hygiene when wearing and handling contact lenses.
- Discontinue makeup use until the stye resolves.
6. Referral to a Specialist
- In cases where the stye does not resolve or becomes recurrent, refer the patient to an ophthalmologist.
- Persistent or worsening symptoms may require surgical drainage or further investigation.
Potential Complications of Stye
- Chalazion Formation: A chronic, painless lump that can form after an internal stye resolves but leaves a residual blocked gland.
- Preseptal Cellulitis: Infection spreading to the surrounding eyelid tissues, leading to redness, swelling, and warmth.
- Recurrent Styes: Especially common in individuals with underlying conditions like blepharitis or rosacea.
Prevention of Stye
- Good Eyelid Hygiene: Regular cleaning of the eyelid margins with gentle cleansers or baby shampoo diluted with water.
- Avoid Eye Contamination: Do not touch or rub the eyes with unclean hands. Avoid using expired or contaminated eye makeup products.
- Contact Lens Care: Follow proper cleaning, storage, and replacement practices for contact lenses.
- Manage Underlying Conditions: Treat chronic eyelid conditions like blepharitis or seborrheic dermatitis to prevent blockage of the glands.
- Boost Immune Health: Maintain a healthy diet, adequate hydration, and overall wellness to reduce susceptibility to infections.


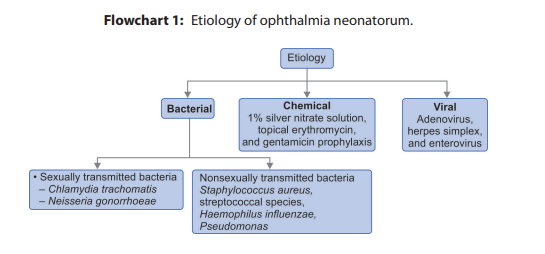
OPHTHALMIA NEONATORUM
Ophthalmia neonatorum, also known as neonatal conjunctivitis, is any eye infection in the first 28 days of life.
Pathophysiology:
Inflammation of the conjunctiva causes erythema, blood vessel dilation, tearing, and drainage. This reaction tends to be more serious due to reduced tear secretion, decreased immune function, decreased lysozyme activity, and the relative absence of lymphoid tissue of the conjunctiva. Neonate tears also lack immunoglobulin IgA.
