

Intracranial hemorrhage (ICH) is bleeding that occurs inside the skull (cranium). This bleeding can happen in three main places:
- Inside the brain tissue itself (brain parenchyma).
- Inside the ventricles (fluid-filled spaces in the brain).
- In the subarachnoid space (the space between the brain and the thin tissues that cover the brain).
Think of it like this: Imagine your brain is like a house. The bleeding can happen inside the rooms (brain tissue), in the plumbing system (ventricles), or in the space between the roof and the ceiling (subarachnoid space).
- Mortality rate: Almost 48% of patients die within 30 days after the bleed occurs. This means nearly half of all children and adults who experience ICH may not survive the first month.
- Percentage of cerebrovascular disorders: ICH accounts for 15-20% of all cerebrovascular (brain blood vessel) disorders.
- In paediatric populations, ICH is less common than in adults but carries significant morbidity and mortality, especially in newborns and infants.
- In Uganda, delayed presentation to healthcare facilities is common due to distance, cost, and cultural beliefs.
- Many children arrive at hospital when bleeding is already severe.
- Nurses are often the first healthcare providers to assess these children.
- Early recognition and rapid intervention can save lives.
- Atherosclerosis Leading to Aneurysms:
- Atherosclerosis is the hardening and narrowing of arteries due to buildup of fatty deposits (plaque).
- In children, this is rare but can occur in those with genetic lipid disorders or severe hypertension.
- The hardened artery walls become weak and may bulge out, forming an aneurysm (a weak, balloon-like swelling in the blood vessel wall).
- When this aneurysm bursts, it causes bleeding into the brain.
- Congenital Defects:
- Arteriovenous Malformation (AVM): This is a tangle of abnormal blood vessels connecting arteries and veins directly, without the normal capillary network in between.
- AVMs are present from birth (congenital).
- They are especially common in young girls for reasons not fully understood.
- The abnormal vessels are weak and prone to rupture.
- Hypertensive Vascular Disease:
- Hypertension means high blood pressure.
- In children, hypertension can be caused by:
- Pheochromocytoma: A rare tumor of the adrenal gland that produces excess adrenaline, causing very high blood pressure.
- Nephritic syndrome: A kidney disease where the kidneys become inflamed and cannot filter properly, leading to fluid retention and high blood pressure.
- Chronic kidney disease.
- Coarctation of the aorta (narrowing of the main artery).
- High blood pressure puts constant pressure on the small blood vessels in the brain, making them weak and likely to burst.
- Racial Factors:
- Black children and adults have a higher incidence of ICH compared to other racial groups.
- This may be due to higher rates of hypertension, sickle cell disease (which affects blood vessels), and limited access to preventive healthcare.
- Increased Age:
- Although this lecture focuses on paediatrics, remember that premature infants and newborns are at high risk for intraventricular hemorrhage due to fragile blood vessels.
- In adolescents, risk increases with age-related vascular changes, especially if they have underlying conditions.
- Other Important Causes in Children:
- Trauma: Falls, road traffic accidents, physical abuse (shaken baby syndrome), birth injury.
- Bleeding disorders: Haemophilia, thrombocytopenia (low platelets), vitamin K deficiency bleeding in newborns.
- Liver disease: The liver makes clotting factors; if diseased, bleeding risk increases.
- Brain tumors: Tumors can bleed into themselves.
- Infections: Meningitis can weaken blood vessel walls.
- Sickle cell disease: Very common in Uganda; causes blood vessel damage and stroke risk.
Imagine a water pipe in your house:
- If the pipe is strong and the water pressure is normal, everything works fine.
- If the pipe becomes weak (from disease, birth defects, or injury) OR the water pressure becomes too high (hypertension), the pipe can burst.
When a brain blood vessel bursts, blood spills out where it doesn't belong. This spilled blood:
- Compresses nearby brain tissue (squashes it).
- Irritates brain tissue and nerves.
- Increases pressure inside the skull (Intracranial Pressure - ICP).
- Cuts off oxygen supply to parts of the brain.
- Can cause brain cells to die within minutes.
- Caused by physical injury to the head.
- Examples: Road traffic accidents, falls from trees (common in Uganda), sports injuries, physical abuse, birth trauma.
- Types include: Epidural hematoma, Subdural hematoma, Contusions (bruising of brain tissue).
- Occurs without physical injury.
- Usually due to medical conditions like hypertension, bleeding disorders, or vascular malformations.
This happens suddenly without warning. There are two main types:
- Intracerebral Hemorrhage (ICH): Bleeding directly into the brain tissue. Usually caused by hypertension (high blood pressure). The blood forms a hematoma (a collection of clotted blood) within the brain. This hematoma pushes on and damages surrounding brain tissue.
- Subarachnoid Hemorrhage (SAH): Bleeding into the subarachnoid space. Most commonly caused by rupture of an aneurysm (a weak, bulging spot on a blood vessel). Blood mixes with the cerebrospinal fluid (CSF) that bathes the brain.
- Vascular malformations: These can cause both intracerebral AND subarachnoid bleeding mixed together.
- Hemorrhagic diathesis: This means the body has a tendency to bleed easily. Causes include:
- Low platelet count (thrombocytopenia).
- Haemophilia and other clotting factor deficiencies.
- Liver disease (liver makes clotting factors).
- Vitamin K deficiency (especially in newborns who haven't received vitamin K at birth).
- Disseminated intravascular coagulation (DIC).
- Hemorrhage into tumors: Some brain tumors have fragile blood vessels that bleed.
- Anticoagulant medications: Blood-thinning drugs can increase bleeding risk.
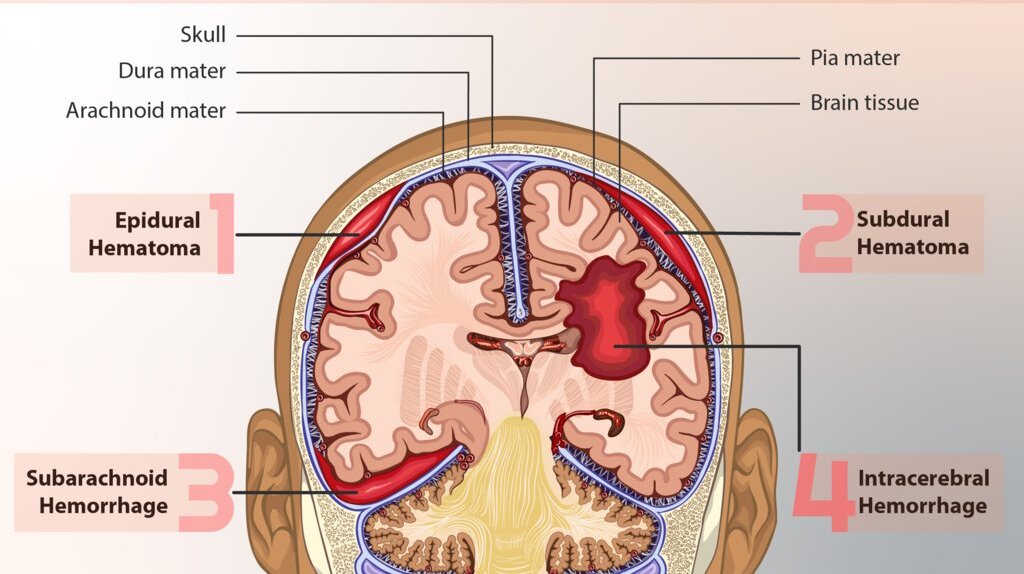
Definition: Epidural hematoma is the accumulation of blood between the Dura mater (the tough outer membrane covering the brain) and the skull, typically following a fracture of the skull.
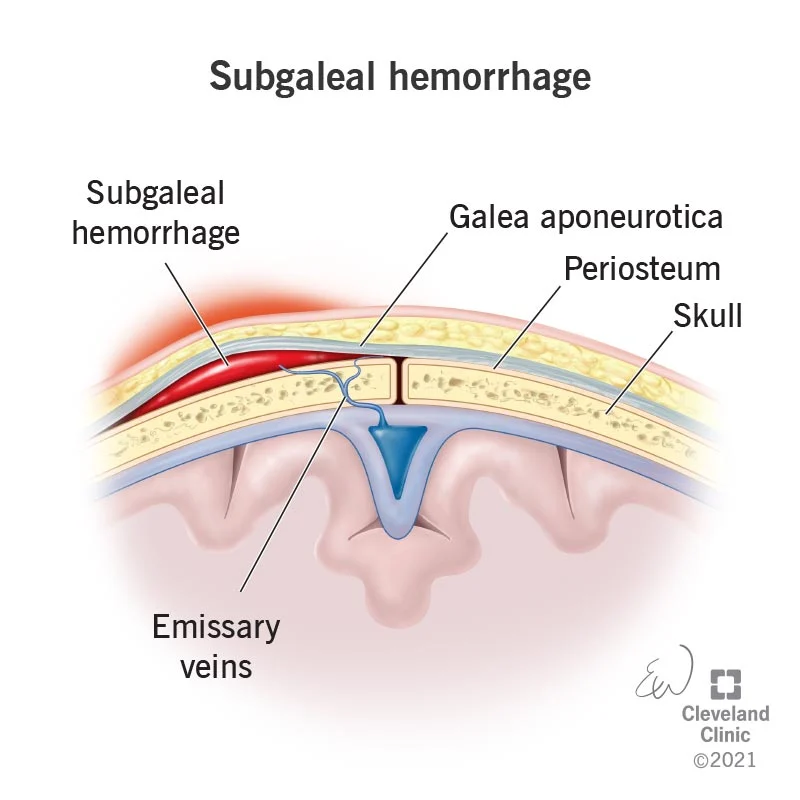
Subgaleal Hemorrhage Context: Subgaleal hemorrhage occurs when emissary veins between the skull and intracranial venous sinuses tear, leading to blood collection between the dura/aponeurosis and the periosteum of the skull.
- Arterial Rupture: Most commonly from the rupture of the middle meningeal artery.
- High-Pressure Bleeding: High-pressure bleeding is a prominent feature. The hematoma expands rapidly since the accumulating blood is arterial in origin.
- Compression: This rapid expansion causes compression of the Dura and flattening of the underlying gyri (brain's surface).
- The Classic Picture (Lucid Interval): An epidural hematoma may briefly lead to loss of consciousness, and then consciousness is regained later (a "lucid interval"). However, the patient develops progressive loss of consciousness if the hematoma is not drained early.
- Subgaleal hemorrhage may present as a large, boggy fluid collection palpable on the head’s surface.
- Characteristic of a subgaleal hemorrhage is that it is not restricted by suture lines and may shift with movement. This is in contrast to the more common cephalohematoma (a superficial collection of blood restricted to the space between the periosteum and skull, which is contained along suture lines).
- Neonates with subgaleal hemorrhage are at high risk for rapid decompensation; the subgaleal space can expand to collect a newborn’s entire intravascular blood volume if bleeding continues unrecognized.
- Swelling of the ears
- Increasing head circumference as bleeding expands into this space (leading to hydrocephalus).
- Hypovolemic shock
- Tachycardia and Hypotension
| Additional Clinical Symptoms | Why It Happens |
|---|---|
| Severe headache | Increased pressure in the skull, blood irritating tissues |
| Vomiting | Increased intracranial pressure (ICP) stimulating the vomiting center |
| Changes in Level of Consciousness (LOC) | Brain compression, reduced blood flow to brain |
| Focal seizures | Irritation of brain tissue; especially after brainstem involvement |
| Nuchal rigidity (stiff neck) | Blood irritating the meninges (coverings of the brain) |
| Visual disturbances | Pressure on optic nerve or visual pathways; papilledema |
Definition: Presence of blood on the surface of the brain beneath its outer covering. SDH is a collection of blood below the inner layer of the dura mater but external to the arachnoid membrane.
- A subdural hemorrhage occurs when bridging veins carrying blood through the dura mater to the arachnoid mater of the meninges are torn.
- This causes bleeding, with blood collecting below the dura and brain.
- It develops most often from the rupture of veins which cross the surface convexities of the cerebral hemispheres.
Subdural hematoma may be acute or chronic:
- Acute subdural hematoma: Develops following trauma and consists of clotted blood, often in the front parietal region. There is no significant compression of gyri initially. Since the accumulated blood is of venous origin, symptoms appear slowly and may become chronic with the passage of time if not fatal.
- Chronic subdural hematoma: Occurs often with brain atrophy. Chronic subdural hematoma is composed of liquid blood. Separating the hematoma from the underlying brain is a membrane composed of granulation tissue.
- Because subdural bleeders are located within the skull, there is often no physical sign on the scalp that reflects injury. Instead, the presence of hemorrhage may initially be unrecognized.
- For most neonates, subdural hemorrhage remains asymptomatic and resolves without consequence.
- Clinical problems can arise in the case of large volume hemorrhage or if bleeding slowly continues over hours or even days, as in cases of bleeding disorders.
- Symptomatic neonates often present 24–48 hours after birth with nonspecific signs such as apnea, respiratory distress, altered neurologic state, or seizures.
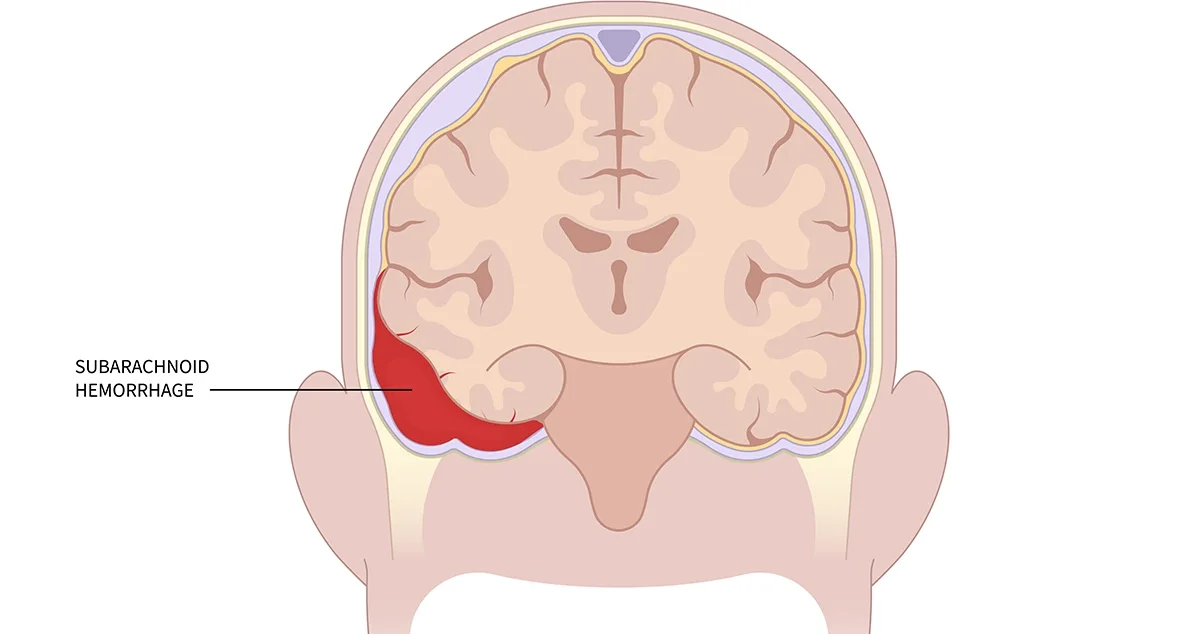
Definition: There’s bleeding between the brain and the thin tissues that cover the brain. These tissues are called meninges. Subarachnoid hemorrhage occurs when the veins of the subarachnoid villi are torn, leading to a collection of blood in the subarachnoid space.
- Hemorrhage into the subarachnoid space is most common, caused by the rupture of an aneurysm, and rarely, the rupture of a vascular malformation.
- Of the three types of aneurysms affecting the larger intracranial arteries—berry, mycotic, and fusiform—berry aneurysms are most important and most common.
- Berry Aneurysms Details:
- They are saccular in appearance with a rounded or lobulated bulge arising at the bifurcation of intracranial arteries and varying in size from 2 mm to 2 cm or more.
- They account for 95% of aneurysms which are liable to rupture.
- Berry aneurysms are rare in childhood but increase in frequency in young adults and middle life.
- They are, therefore, not congenital anomalies but develop over the years from a developmental defect of the media of the arterial wall at the bifurcation of arteries, forming thin-walled saccular bulges.
- Although most berry aneurysms are sporadic in occurrence, there is an increased incidence of their presence in association with congenital polycystic kidney disease and coarctation of the aorta.
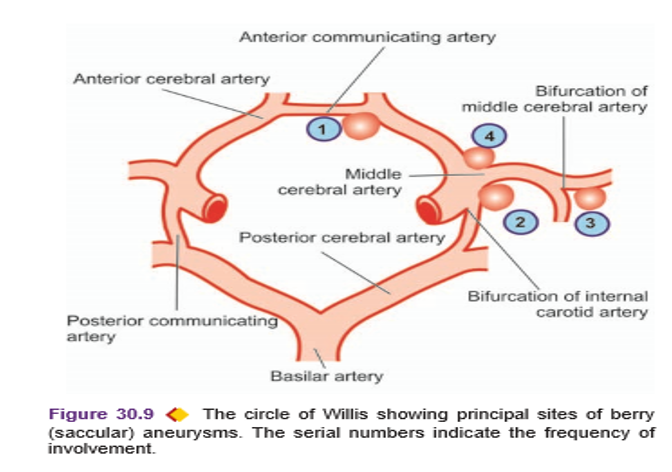
In more than 85% of cases of subarachnoid hemorrhage, the cause is massive and sudden bleeding from a berry aneurysm on or near the circle of Willis. The four most common sites are:
- In relation to the anterior communicating artery.
- At the origin of the posterior communicating artery from the stem of the internal carotid artery.
- At the first major bifurcation of the middle cerebral artery.
- At the bifurcation of the internal carotid into the middle and anterior cerebral arteries.
- A sudden, sharp headache usually comes before a subarachnoid hemorrhage (often described as "the worst headache of my life").
- Typical symptoms also include loss of consciousness and vomiting.
Definition: An intracerebral brain hemorrhage (ICH) is bleeding inside the brain caused by the rupture of a damaged blood vessel in the head. As the amount of blood increases, the build-up of pressure can lead to brain damage, unconsciousness, or even death.
- This involves bleeding into the brain’s ventricular system, where the cerebrospinal fluid is produced and circulates through towards the subarachnoid space.
- It can result from physical trauma or from hemorrhaging in a stroke (Hypertension - HTN). This is the most common type of ICH that occurs with a stroke. It’s not usually the result of injury (spontaneous).
- Spontaneous intracerebral hemorrhage occurs mostly in patients of hypertension.
- Children with systemic diseases that manifest with HTN are at risk because they develop micro aneurysms in very small cerebral arteries in the brain tissue.
- Rupture of one of the numerous micro aneurysms is believed to be the cause of intracerebral hemorrhage.
- Not common to have recurrent intracerebral hemorrhages, unlike the case of subarachnoid hemorrhages.
- The common sites of hypertensive intracerebral hemorrhage are the region of the basal ganglia (particularly the putamen and the internal capsule), pons, and the cerebellar cortex.
- There are very few clinical symptoms of ICH initially.
- When present, signs may include an acute drop in hematocrit, new-onset hypotension, and lethargy.
- However, these symptoms are often present in extremely low birth weight (ELBW) and premature infants.
A prominent warning sign is the sudden onset of neurological deficit. This is a problem with the brain’s functioning. The symptoms progress over minutes to hours and they include:
- Headache accompanied by neck stiffness
- Drowsiness
- Difficulty speaking/crying
- Nausea and Vomiting
- Decreased consciousness, Seizure, or Coma
- Weakness in one part of the body
- Elevated blood pressure
- Cognitive dysfunction or memory loss
- Sudden tingling, weakness, numbness, or paralysis of the face, arm, or leg, particularly on one side of the body
- Loss of balance or coordination in older children
- Babies less than 12 months old may develop a swollen fontanel, or soft spot on the head.
- Hypovolemic Shock:
- What is it?: The body loses too much blood, leading to insufficient blood volume to maintain blood pressure and organ perfusion.
- How it happens in ICH: Although the bleeding is inside the skull, massive bleeding can still cause significant blood loss from circulation.
- Signs to watch for: Rapid, weak pulse (tachycardia), Low blood pressure (hypotension), Cold, clammy skin, Rapid breathing, Decreased urine output, Altered mental status, Delayed capillary refill (more than 2 seconds).
- Acute Hydrocephalus:
- What is it?: Buildup of cerebrospinal fluid (CSF) in the ventricles because blood clots block the normal flow pathways.
- Signs in children: Rapidly increasing head circumference (in infants whose skull bones haven't fused), Bulging fontanelle (soft spot on baby's head), Sunset eyes (eyes look downward, white showing above iris), Vomiting, Irritability, Lethargy.
- Management: Emergency insertion of an external ventricular drain (EVD) to remove excess fluid.
- Focal Seizures / Seizure Disorders:
- Blood and its breakdown products irritate brain tissue.
- This irritation can trigger abnormal electrical activity = seizures.
- Seizures further increase ICP and oxygen demand.
- Some children develop epilepsy (recurrent seizures) as a long-term complication.
- Other Complications (Crucial exhaustive list):
- Cerebral vasospasm: Blood vessels narrow 3-14 days after SAH, reducing blood flow and causing stroke.
- Rebleeding: Especially dangerous in aneurysmal SAH.
- Hyponatremia: Low sodium levels due to SIADH (Syndrome of Inappropriate Antidiuretic Hormone) or cerebral salt wasting.
- Neurogenic pulmonary edema: Fluid in lungs due to brain injury.
- Cardiac arrhythmias: Brain injury affects heart regulation.
- Deep vein thrombosis (DVT): From prolonged bed rest.
- Pressure ulcers: From immobility.
- Aspiration pneumonia: From impaired swallowing and consciousness.
- Long-term neurological deficits: Paralysis, speech problems, cognitive impairment, behavioral changes.

- CT Scan (Computed Tomography):
- What is it?: A special X-ray that takes detailed pictures of the brain in slices.
- Why it's used: FAST — takes only minutes, Can detect fresh blood easily (blood appears bright white on CT), Shows the size and location of hemorrhage, Can see if blood has entered ventricles, Can see skull fractures.
- When to do it: IMMEDIATELY for any child with suspected ICH.
- Limitations: Radiation exposure (but benefits outweigh risks in emergency), May miss very small bleeds or bleeds more than a few days old, Requires child to stay still (may need sedation).
- MRI (Magnetic Resonance Imaging):
- What is it?: Uses magnetic fields and radio waves to create detailed brain images.
- Why it's used: Better than CT for detecting small bleeds, old bleeds, and vascular malformations. No radiation. Better for looking at brainstem and posterior fossa.
- When to do it: When CT is inconclusive or for follow-up.
- Limitations: Takes longer (30-60 minutes), Child must stay very still (often needs sedation or general anesthesia), Cannot use if child has certain metal implants, Less available and more expensive in Uganda.
- Cerebral Angiography:
- What is it?: A special X-ray test where dye is injected into blood vessels to see the arteries and veins of the brain.
- Why it's used: Gold standard for diagnosing aneurysms, Shows exact location, size, and shape of aneurysms, Identifies vascular malformations, Helps plan surgical or endovascular treatment.
- How it's done: A catheter (thin tube) is inserted into an artery in the groin. It is threaded up to the brain arteries. Dye is injected. X-ray pictures are taken.
- Risks: Allergic reaction to dye, Damage to blood vessels, Stroke, Kidney problems from dye.
- Lumbar Puncture (Spinal Tap):
- What is it?: A needle is inserted into the lower back to collect cerebrospinal fluid (CSF).
- Why it's used: To confirm subarachnoid hemorrhage when CT is negative but suspicion remains high. Blood in CSF indicates SAH.
🚨 CRITICAL SAFETY RULES — NEVER do lumbar puncture if:
- There is evidence of increased intracranial pressure (ICP)
- CT shows mass effect or shift of brain structures
- Child has papilledema (swollen optic disc)
- Child is unconscious or has deteriorating consciousness
- Why it's dangerous with high ICP: Removing fluid from the spinal canal can cause the brain to shift downward (herniation), which can be fatal.
- When it IS safe: CT scan shows NO evidence of increased ICP, CT is negative for hemorrhage, But clinical suspicion of SAH remains high, Child is awake and cooperative.
- Other Important Tests (Crucial exhaustive list):
- Complete Blood Count (CBC): To check for anemia from blood loss, platelet count.
- Coagulation profile (PT, PTT, INR): To check blood clotting ability.
- Blood glucose: Both high and low sugar can worsen brain injury.
- Electrolytes: Especially sodium (hyponatremia is common after SAH).
- Liver function tests: If liver disease is suspected as cause.
- Blood culture: If infection (mycotic aneurysm) is suspected.
- Echocardiogram: To check heart function (neurogenic cardiac changes).
- Chest X-ray: If aspiration or neurogenic pulmonary edema suspected.
Goal of Medical Management: Prevent further bleeding, Control intracranial pressure, Maintain adequate blood flow to the brain, Prevent complications, Support vital functions.
- Why bed rest? Movement and activity increase blood pressure. Increased blood pressure increases risk of rebleeding. Rest allows the body to start healing.
- Why sedation? Anxiety and pain increase blood pressure. Agitated children may move excessively. Sedation keeps the child calm and cooperative.
- Nursing considerations: Explain to family why the child must stay still. Keep the room quiet and dimly lit. Minimize unnecessary procedures and disturbances. Use sedation as prescribed (e.g., midazolam, morphine). Monitor respiratory rate closely with sedation — it can slow breathing.
- When to use: If the child has a bleeding disorder. If the child is on anticoagulant medications (like warfarin). If liver disease prevents normal clotting factor production. If vitamin K deficiency is present (common in newborns who didn't receive vitamin K at birth).
- Fresh Frozen Plasma (FFP): Contains all clotting factors. Given intravenously. Helps the blood to clot and stop bleeding.
- Vitamin K: Essential for the liver to make clotting factors II, VII, IX, and X. Given by injection (intramuscular or intravenous). In newborns, vitamin K is given at birth to prevent hemorrhagic disease of the newborn.
- Nursing considerations: Monitor for allergic reactions to FFP. Check coagulation studies before and after administration. Vitamin K given IV can cause flushing and hypotension — give slowly.
- Why give prophylactically (before seizures occur)? Seizures increase brain metabolism and oxygen demand. Seizures increase intracranial pressure. Blood in the brain is irritating and can trigger seizures. Preventing seizures is easier than treating them.
- Common medications: Phenytoin (Loading dose followed by maintenance), Levetiracetam (Keppra) (Increasingly preferred; fewer side effects), Phenobarbital (Especially in neonates).
- Nursing considerations: Monitor drug levels (especially phenytoin). Watch for side effects: drowsiness, rash, gum swelling (phenytoin). Ensure airway is protected if seizures occur despite prophylaxis. Have emergency seizure medications available (diazepam, lorazepam).
- Why it's important: Pain increases blood pressure. Pain causes agitation and movement. Children in pain cannot rest and heal.
- Medications used: Acetaminophen/Paracetamol (First line for mild pain; doesn't affect platelets), Morphine or other opioids (For severe pain; use cautiously as they can depress respiration and affect pupil assessment). Avoid NSAIDs (ibuprofen, aspirin) if bleeding risk or low platelets, as they can worsen bleeding.
- Nursing considerations: Use pain assessment scales appropriate for age (FLACC for infants, Wong-Baker FACES for older children). Monitor respiratory rate with opioid use. Document pain scores before and after medication.
- Why use them? Children with ICH are on bed rest. Immobility increases risk of deep vein thrombosis (DVT) — blood clots in leg veins. DVT can break off and travel to lungs (pulmonary embolism), which can be fatal.
- How they work: SCDs: Inflatable sleeves wrapped around legs that periodically squeeze and release, mimicking muscle movement and promoting blood flow. Anti-embolism stockings: Tight-fitting stockings that compress leg veins and improve blood return to the heart.
- Nursing considerations: Ensure proper fit — too tight can restrict blood flow, too loose won't work. Check skin under devices/stockings every shift for pressure areas. Remove and inspect legs for signs of DVT (Swelling, Warmth, Redness, Pain, Tenderness). In very small children, SCDs may not be available; passive range of motion exercises by nurses are important.
- Blood Pressure Control:
- Goal: Lower blood pressure to prevent rebleeding, but NOT too low (brain still needs blood flow).
- Target: Usually systolic BP 120-140 mmHg or mean arterial pressure (MAP) appropriate for age.
- Medications: Labetalol (IV; reduces BP without affecting cerebral blood flow much), Nicardipine (IV infusion; easy to titrate). Avoid nitroprusside if possible — can increase ICP.
- Nursing actions: Continuous BP monitoring (arterial line if available). Titrate medications carefully. Watch for hypotension (too low BP) which can cause brain ischemia.
- Intracranial Pressure (ICP) Management:
- Elevate head of bed 15-30 degrees (promotes venous drainage).
- Osmotic therapy: Mannitol: IV osmotic diuretic; pulls fluid from brain tissue into blood vessels, then kidneys excrete it. Monitor serum osmolality (keep <320 mOsm/kg). Watch for dehydration and electrolyte imbalances. Check urine output. Hypertonic saline (3%): Alternative to mannitol; draws fluid from brain tissue. Monitor sodium levels closely. Risk of central pontine myelinolysis if corrected too fast.
- CSF drainage: External ventricular drain (EVD) if hydrocephalus present.
- Hyperventilation: Briefly used in emergency to reduce ICP by causing vasoconstriction. Target PaCO2: 30-35 mmHg. Do NOT maintain for long — causes excessive vasoconstriction and brain ischemia.
- Temperature control: Fever increases ICP and brain metabolism. Use antipyretics and cooling blankets.
- Sedation and paralysis: If ICP remains high despite other measures, neuromuscular blockade may be used (e.g., vecuronium) — but this requires ventilator support.
- Fluid Management:
- Goal: Maintain euvolemia (normal fluid status) — not too much, not too little.
- Avoid hypotonic fluids (like 5% dextrose in water) — they can worsen brain swelling.
- Use isotonic fluids: Normal saline (0.9%) or lactated Ringer's.
- Monitor: Intake and output strictly, Daily weights, Serum sodium (hyponatremia worsens brain swelling), Urine specific gravity.
- Prevention of Vasospasm (especially after SAH):
- Nimodipine: Calcium channel blocker given orally or via NG tube. Reduces risk of cerebral vasospasm. Given for 21 days after SAH. Can cause hypotension — monitor BP.
- "Triple-H therapy" (if vasospasm occurs): Hypertension (Deliberately raise BP to force blood through narrowed vessels), Hypervolemia (Increase blood volume), Hemodilution (Thin the blood slightly to improve flow).
- Nursing: Very close monitoring in ICU setting required.
- Electrolyte Management:
- Hyponatremia (low sodium) is common after SAH. Can be due to SIADH or cerebral salt wasting. SIADH: Restrict fluids. Cerebral salt wasting: Give salt and fluids. Nursing: Monitor sodium levels, urine sodium, fluid balance.
- Hypernatremia can occur with mannitol or diabetes insipidus.
- Hypokalemia (low potassium) from diuretics.
- Hypomagnesemia can worsen vasospasm.
- Nutritional Support:
- Children with brain injury need adequate nutrition for healing.
- If unconscious or unable to swallow: nasogastric (NG) tube feeding.
- Start feeds early (within 24-48 hours if possible).
- Monitor gastric residuals. Prevent constipation (straining increases ICP).
- Infection Prevention:
- Children with ICH are vulnerable to infections: Pneumonia (From aspiration or prolonged ventilation), Urinary tract infection (From catheterization), Meningitis (From CSF leaks or EVD), Wound infection (After surgery).
- Nursing actions: Strict hand hygiene. Oral care every 2-4 hours. Elevate head of bed to prevent aspiration. Aseptic technique for all invasive procedures. Monitor for signs of infection: fever, increased white blood cells, purulent secretions.
- Gastrointestinal Protection:
- Brain injury increases risk of stress ulcers.
- Prophylaxis: Proton pump inhibitors (e.g., omeprazole) or H2 blockers (e.g., ranitidine).
- Monitor for signs of GI bleeding: coffee-ground vomitus, black tarry stools (melena), dropping hemoglobin.
- Glycemic Control:
- Both high and low blood sugar worsen brain injury.
- Target: Blood glucose 80-180 mg/dL. Monitor regularly. Use insulin infusion if needed.
- What is it? A surgical operation where a piece of the skull bone is removed (bone flap) to access the brain. The hematoma (blood clot) is evacuated (removed). The bone flap may be replaced or stored and replaced later.
- When is it needed? Large intracerebral hematoma causing significant mass effect. Epidural hematoma causing rapid neurological deterioration. Subdural hematoma. Cerebellar hematoma >3 cm. Any hematoma causing brain herniation signs.
- Nursing care before surgery: Fast the child (no food or drink) — usually 6 hours for solids, 2 hours for clear fluids. Obtain informed consent from parents/guardians (explain in local language). Ensure blood is available for transfusion. Shave hair as needed. Administer preoperative medications. Insert urinary catheter. Mark surgical site.
- Nursing care after surgery: Neurological monitoring: GCS (Glasgow Coma Scale), pupil size and reaction, limb movement — every 15 minutes initially, then hourly. ICP monitoring if device in place. Head positioning: Usually flat or slightly elevated as ordered. Wound care: Keep dressing clean and dry; watch for CSF leak (clear fluid), bleeding, infection signs. Pain management. Seizure prophylaxis. Prevent complications: DVT, pneumonia, pressure ulcers. Family support: Explain what to expect, reassure, involve in care when possible.
What is it? A minimally invasive procedure done through blood vessels. A catheter is inserted into an artery (usually in the groin) and guided to the brain. Used to treat aneurysms and vascular malformations without open surgery.
- Aneurysm Coiling: Tiny platinum coils are inserted into the aneurysm through the catheter. The coils fill the aneurysm and promote blood clotting inside it. This seals off the aneurysm from the main blood vessel. Advantages: No open brain surgery, faster recovery. Disadvantages: May not work for all aneurysm shapes; risk of coil compaction or aneurysm recurrence.
- Parent Artery Occlusion: The artery that feeds the aneurysm is deliberately blocked. Used when the aneurysm cannot be coiled or clipped. Requires good collateral blood flow (other pathways to supply that brain area). Risk: Stroke if collateral flow is insufficient.
Nursing care:
- Post-procedure bed rest: Usually 4-6 hours with leg straight (groin site must clot).
- Groin site monitoring: Check for bleeding, hematoma, pulse in the leg.
- Neurological checks: Watch for stroke signs (weakness, speech problems, vision changes).
- Hydration: Encourage fluids to flush out contrast dye.
- Monitor kidney function: Contrast can damage kidneys.
- Burr Holes: Small holes drilled in the skull. Used to drain epidural or subdural hematomas in emergency. Less invasive than craniotomy.
- External Ventricular Drain (EVD) Placement: A catheter inserted into the ventricle to drain CSF. Relieves hydrocephalus and reduces ICP. Nursing: Keep EVD system at correct height (usually level with tragus of ear or as ordered). Do NOT clamp or raise/lower without doctor's order. Monitor CSF color, amount, and pressure. Strict aseptic technique — risk of meningitis. Do NOT let drainage chamber overfill.
- Decompressive Craniectomy: Removal of a large piece of skull to allow swollen brain to expand outward. Used when ICP is life-threatening and other measures fail. Skull bone stored (often in abdomen) or synthetic patch used for later replacement.
Why it's the most important nursing duty: Changes in neurological status are often the FIRST sign of deterioration. Early detection allows early intervention, which saves lives and brain function.
- Level of Consciousness (LOC): Use Glasgow Coma Scale (GCS) for children >5 years. Use Paediatric GCS modifications for younger children.
- Components: Eye opening (1-4): Spontaneous, to speech, to pain, none. Verbal response (1-5): Oriented, confused, inappropriate words, incomprehensible sounds, none. Motor response (1-6): Obeys commands, localizes pain, withdraws, flexion, extension, none.
- Score interpretation: 15 = Fully conscious, 13-14 = Mild brain injury, 9-12 = Moderate brain injury, 3-8 = Severe brain injury (coma).
- Document GCS every hour initially, then every 2-4 hours as stable. Report ANY decrease in GCS immediately.
- Pupillary Assessment: Check size, shape, and reaction to light.
- Normal: Equal, round, reactive to light and accommodation (PERRLA).
- Abnormal signs: One pupil larger than the other (anisocoria), Fixed and dilated pupil (bad sign — brain herniation), Pinpoint pupils (brainstem issue, opioid effect), Sluggish reaction.
- How to check: Shine penlight into each eye; both pupils should constrict equally. Document and report changes immediately.
- Vital Signs:
- Blood Pressure (BP): High BP can cause rebleeding. Low BP reduces brain perfusion. Watch for Cushing's Triad (late sign of increased ICP): Increased systolic BP with widened pulse pressure, Bradycardia (slow heart rate), Irregular respirations.
- Pulse (PR): Tachycardia early, bradycardia late.
- Respiratory Rate (RR): Changes in breathing pattern indicate brainstem involvement (Cheyne-Stokes: Alternating deep and shallow breathing, Central neurogenic hyperventilation: Deep, rapid breathing, Ataxic breathing: Completely irregular).
- Temperature: Fever increases ICP and brain metabolism; hypothermia may be induced therapeutically.
- Check and document every 15-30 minutes in acute phase.
- Motor Function: Check strength in all four limbs. Compare left and right sides. Use grading scale (0-5): 0 = No movement, 1 = Flicker, 2 = Movement without gravity, 3 = Movement against gravity, 4 = Movement against some resistance, 5 = Normal strength. New weakness on one side suggests expanding hematoma or new bleed.
- Neurological Flow Record: A special chart to document all neurological observations over time. Shows trends and changes. Nurses must maintain this meticulously.
What are they? Special measures to prevent aneurysm rupture or rebleeding before definitive treatment.
- Absolute Bed Rest: Child must stay in bed at all times. Use bedpan or diapers for toileting. No walking to bathroom. Turn gently with log-roll technique.
- Quiet, Non-Stressful Environment: Keep room lights dim. Minimize noise — no loud talking, no television, no radio unless very quiet. Limit alarms and beeping when possible. Cluster care activities to allow rest periods.
- Restrict Visitors: Only immediate family allowed. Limit to 1-2 people at a time. Visitors must be calm and quiet. No children as visitors (they may be noisy or carry infections). Explain to family WHY these restrictions are necessary.
- Avoid Straining (Valsalva Maneuver Prevention): The Valsalva maneuver is straining while holding your breath (like when pushing to defecate). This suddenly increases blood pressure and can burst an aneurysm.
- How to prevent: For toileting: Instruct child (if old enough) to exhale while voiding or defecating, not hold breath. Stool softeners: Give regularly to prevent constipation. No straining to pass stool. No coughing: Treat cough promptly; if child needs to cough, teach them to do it gently with mouth open. No nose blowing: Teach child to wipe nose gently instead. No heavy lifting: Even lifting a water jug can be too much.
- Eliminate Caffeine: Caffeine increases blood pressure and heart rate. No tea, coffee, cola drinks, energy drinks, chocolate. Provide alternatives: water, diluted juice, milk.
- Minimize External Stimuli: No sudden surprises or shocks. Gentle touch and voice. Warn child before any procedure ("I'm going to check your temperature now"). Keep room temperature comfortable.
- Administer All Personal Care: Nurses should do everything for the child. Bathing in bed. Oral care. Feeding (if not self-feeding). Changing clothes and linens. This minimizes child's exertion.
- Elevate Head of Bed 15-30 Degrees. Why: Promotes venous drainage from the head, which reduces intracranial pressure. How: Use pillows or adjust bed angle.
- Exceptions: If BP is very low, flat position may be needed to maintain brain perfusion. After certain surgeries, surgeon may order different positioning. Always follow doctor's specific orders.
- Keep head in midline position (not turned to side) to avoid compressing neck veins.
- Avoid hip flexion (bending at waist) as it increases abdominal pressure and can raise ICP.
- Anti-Embolism Stockings or Sequential Compression Devices: Apply correctly. Check skin underneath. Remove for skin inspection as per protocol.
- Leg Observations: Check both legs every shift for: Swelling: Measure calf circumference; compare left and right. Warmth: Use back of hand to compare temperature. Redness: Look for erythema. Pain or tenderness: Ask child or observe facial expressions in non-verbal children. Homan's sign (pain on dorsiflexion of foot): NOT routinely checked anymore as it can dislodge clots. Document findings.
- Passive Range of Motion Exercises: If child is unconscious or unable to move: Move each joint through its full range gently. Do this at least twice daily. Prevents joint stiffness AND promotes circulation. In children with ICH, coordinate with physiotherapist.
Activities to Avoid (that suddenly increase BP):
| Activity | Why It's Dangerous | Nursing Action |
|---|---|---|
| Valsalva maneuver (straining) | Sudden BP spike | Stool softeners, teach exhaling during toileting |
| Straining during defecation | BP spike | Regular laxatives, monitor bowel movements |
| Caffeine intake | Increases BP and heart rate | Remove all caffeinated items from diet |
| Emotional stress | Adrenaline release increases BP | Calm environment, sedation if needed |
| Physical exertion | Increases cardiac output and BP | Complete bed rest |
| Pain | Increases BP | Regular analgesia |
| Full bladder | Increases BP | Regular toileting, catheter if needed |
- Fluid Volume Expanders: Used if child is in shock or has low blood volume. Examples: Normal saline, lactated Ringer's, blood products. Nursing: Check type and expiry. Monitor infusion rate. Watch for fluid overload (crackles in lungs, swelling). Monitor urine output.
- Anti-Seizure Medications: Give exactly on time — missed doses can trigger seizures. Monitor therapeutic levels. Watch for side effects. Never stop abruptly — taper as ordered.
- Analgesics: Assess pain before and after. Monitor respiratory depression with opioids. Use non-pharmacological methods too (positioning, distraction, calm environment).
- Other Medications: Mannitol: Give as bolus over 15-20 minutes; use filter; check serum osmolality. Nimodipine: Give via NG tube if child can't swallow; don't crush enteric-coated tablets. Antihypertensives: Titrate carefully; monitor BP continuously if possible. Proton pump inhibitors: Give before meals if oral.
Report IMMEDIATELY if you observe:
| Sign | What It May Mean |
|---|---|
| Sudden severe headache | Rebleeding, increased ICP |
| Repeated vomiting | Increased ICP |
| Decreased level of consciousness | Expanding hematoma, brain herniation |
| Unequal pupils | Brain herniation (uncal) |
| Fixed dilated pupil | Severe brainstem compression |
| New weakness on one side | Expanding hematoma, stroke |
| Seizures | Blood irritation, increased ICP |
| Decreased or absent breathing | Brainstem failure |
| Cushing's triad | Critical increased ICP |
| Fever | Infection or brain injury response |
| CSF leak from nose or ear | Basal skull fracture |
- Communication: Explain the condition in simple, non-medical language. Use interpreters if needed (Uganda has many languages). Be honest but hopeful. Update family regularly, even if no change.
- Emotional Support: Allow family to express fears and grief. Provide privacy for crying or prayer. Connect with hospital chaplain or counselor if available. Recognize that in Uganda, extended family may be involved in decision-making.
- Education: Teach family about: Why child must stay still. Importance of quiet environment. Signs to watch for and report. Long-term outlook and rehabilitation needs. How to prevent future ICH (blood pressure control, safety).
- Involvement in Care: When stable, allow family to help with simple care. This empowers them and builds confidence for home care.
- Discharge Planning: Arrange follow-up appointments. Ensure family understands medications. Provide written instructions in local language if possible. Refer to rehabilitation services (physiotherapy, speech therapy, occupational therapy). Connect with community health workers for home follow-up.
| Nursing Diagnosis | Goals | Interventions |
|---|---|---|
| Ineffective tissue perfusion (cerebral) related to bleeding or increased ICP | Maintain adequate cerebral perfusion | Monitor neuro signs, maintain BP in ordered range, position head properly, administer osmotic agents, prepare for surgery if needed |
| Risk for increased intracranial pressure | ICP remains within normal limits | Avoid Valsalva, control pain, prevent seizures, manage fluids, monitor for signs of increased ICP |
| Impaired physical mobility related to neurological deficit | Prevent complications of immobility | Passive ROM, position changes every 2 hours, DVT prevention, pressure injury prevention |
| Risk for aspiration related to decreased LOC | No aspiration events | Elevate head of bed, check swallowing before oral feeding, suction as needed, oral care |
| Anxiety (family) related to critical illness | Family copes effectively | Regular updates, emotional support, involve in care, provide information, connect with support services |
| Risk for infection related to invasive procedures | No infection | Aseptic technique, hand hygiene, monitor for signs of infection, prophylactic antibiotics if ordered |
| Impaired skin integrity related to immobility | No pressure injuries | Turn every 2 hours, pressure-relieving mattress, skin inspection, nutrition support, keep skin dry |
Yaa you’ve simplified the topic for me thanks
Long live sir
Well done. We request for more past papers and nursing care plans thank you
We just love your research, keep the candle burning
A good one….. thanks