Budding
2.2 The Six Major Classes of ARVs
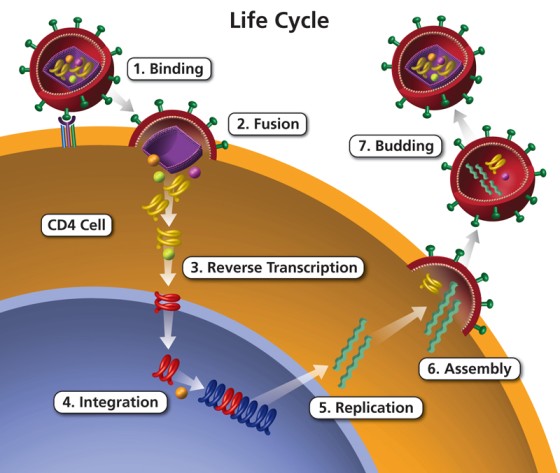
Each class of ARV attacks a different step in the HIV life cycle:
| Class |
What It Does |
Step Attacked |
| NRTIs |
Fake building blocks that stop DNA building |
Reverse Transcription |
| NNRTIs |
Block the reverse transcriptase enzyme directly |
Reverse Transcription |
| PIs |
Block the protease enzyme (stops virus maturation) |
Assembly / Maturation |
| INSTIs |
Block the integrase enzyme (stops HIV DNA mixing) |
Integration |
| Entry Inhibitors |
Block HIV from entering the CD4 cell |
Attachment/Fusion |
| PK Boosters |
Make other ARVs work better and longer |
Not an ARV itself |
MODULE 3: DETAILED STUDY OF EACH ARV CLASS
3.1 NRTIs (Nucleoside/Nucleotide Reverse Transcriptase Inhibitors)
Pronounced: "En-Ar-Tee-Eyes"
What They Do:
NRTIs are "fake DNA building blocks." HIV needs real building blocks (nucleotides) to make its DNA. NRTIs pretend to be real building blocks, but when HIV tries to use them, the DNA chain stops growing. It's like giving a builder fake bricks — the wall cannot be completed.
How They Work (Detailed Pharmacology):
- HIV has an enzyme called reverse transcriptase.
- This enzyme reads HIV's RNA and builds a complementary DNA strand.
- NRTIs look like the natural nucleosides that reverse transcriptase needs. However, they lack a crucial 3'-OH group needed to attach the next nucleotide.
- Reverse transcriptase picks up the NRTI instead of the real building block.
- Once the fake building block is added, no more blocks can be added. The DNA chain is terminated (Chain Termination).
- Result: HIV cannot make copies of itself.
| Generic Name |
Abbreviation |
Brand Name |
Key Notes |
| Tenofovir |
TDF or TAF |
Viread (TDF), Vemlidy (TAF) |
Backbone of most regimens. TAF is safer for bones/kidneys. |
| Lamivudine |
3TC |
Epivir |
Very well tolerated. Also treats Hep B. |
| Emtricitabine |
FTC |
Emtriva |
Similar to 3TC. Can cause hyperpigmentation of palms/soles. |
| Zidovudine |
AZT or ZDV |
Retrovir |
Can cause severe anemia and bone marrow suppression. |
| Abacavir |
ABC |
Ziagen |
Must test for HLA-B*5701 gene to prevent fatal hypersensitivity. |
| Stavudine |
d4T |
Zerit |
NO LONGER RECOMMENDED — causes severe lipoatrophy & neuropathy. |
NRTI Clinical Summary: Drugs, Indications, Dosages, Contraindications & Side Effects
| Common Drugs |
Indications |
Standard Adult Dosages |
Contraindications |
Major Side Effects |
| Tenofovir (TDF) |
HIV-1, Chronic Hepatitis B |
300 mg once daily |
Severe renal impairment (CrCl < 30 mL/min) |
Nephrotoxicity, decreased bone mineral density. |
| Lamivudine (3TC) |
HIV-1, Chronic Hepatitis B |
300 mg once daily OR 150 mg twice daily |
Hypersensitivity |
Minimal; mild nausea, headache. |
| Zidovudine (AZT) |
HIV-1, PMTCT, Post-exposure prophylaxis |
300 mg twice daily |
Severe anemia, bone marrow suppression, neutropenia |
Macrocytic anemia, neutropenia, myopathy, hyperpigmentation. |
| Abacavir (ABC) |
HIV-1 (often when TDF is contraindicated) |
600 mg once daily OR 300 mg twice daily |
HLA-B*5701 positive (high risk of fatal hypersensitivity), severe hepatic impairment |
Hypersensitivity reaction (fever, rash, respiratory symptoms), possible increased CV risk. |
Common Side Effects of NRTIs:
- Nausea, vomiting, headache, and fatigue.
- Diarrhea.
- Lactic acidosis: Rare but serious. Occurs because NRTIs can mistakenly inhibit mitochondrial DNA polymerase gamma, starving human cells of ATP and causing lactic acid buildup.
- Lipodystrophy: Fat changes in body (especially with old drugs like d4T).
- Bone problems & Kidney problems: Specifically with Tenofovir Disoproxil Fumarate (TDF). It can cause Fanconi syndrome (kidney wasting) and osteoporosis.
🚨 NURSING ALERT: Lactic Acidosis
Symptoms: Deep, rapid breathing (Kussmaul breathing), muscle pain, weakness, stomach pain, feeling cold.
This is a medical emergency! If a patient on NRTIs presents with these, STOP the drug and call the doctor immediately. Check ABGs and lactate levels.
❓ Clinical Scenario: TDF Toxicity
Case: A 45-year-old man on TDF+3TC+DTG comes to the clinic complaining of severe bone pain and difficulty walking.
Nursing Action: As a nurse, you check his kidney function (creatinine) and bone density. You know that TDF can cause renal toxicity (which leaks phosphate) leading to bone weakening. The doctor may switch him to TAF (tenofovir alafenamide), which targets the HIV cell much more efficiently, meaning less drug floats in the blood to damage bones and kidneys.
🧠 MNEMONIC for NRTIs: "Tenofovir And Lamivudine Can Always Zap HIV"
- Tenofovir
- And (Abacavir)
- Lamivudine
- Can (EmtriCitabine - FTC)
- Always
- Zidovudine
- HIV
3.2 NNRTIs (Non-Nucleoside Reverse Transcriptase Inhibitors)
Pronounced: "En-En-Ar-Tee-Eyes"
What They Do:
NNRTIs also attack the reverse transcriptase enzyme, but they work differently from NRTIs. They bind directly to the enzyme and change its shape, so it cannot work anymore. Think of it like putting a wrong key in a lock — the lock changes shape and the real key cannot fit anymore.
How They Work (Detailed Pharmacology):
- Reverse transcriptase has an active pocket where it binds to nucleosides (where NRTIs work).
- NNRTIs do NOT act as fake building blocks. Instead, they fit into a different, allosteric pocket on the enzyme.
- When the NNRTI binds to this pocket, it forces a conformational (shape) change in the active site of the enzyme.
- The enzyme becomes "deformed" and paralyzed. It cannot build DNA anymore. HIV replication stops. (This is non-competitive inhibition).
| Generic Name |
Abbreviation |
Brand Name |
Key Notes |
| Efavirenz |
EFV |
Sustiva, Stocrin |
Crosses blood-brain barrier. Causes vivid dreams, dizziness. Avoid in 1st trimester pregnancy. |
| Nevirapine |
NVP |
Viramune |
High risk for severe liver rash (Stevens-Johnson syndrome). Requires 2-week dose lead-in. |
| Etravirine |
ETR |
Intelence |
Second-line use. Works even against some NNRTI-resistant HIV. |
| Rilpivirine |
RPV |
Edurant |
Must take with full meal. Absolutely AVOID proton pump inhibitors (omeprazole). |
| Doravirine |
DOR |
Pifeltro |
Newer drug, fewer CNS side effects than Efavirenz. |
NNRTI Clinical Summary: Drugs, Indications, Dosages, Contraindications & Side Effects
| Common Drugs |
Indications |
Standard Adult Dosages |
Contraindications |
Major Side Effects |
| Efavirenz (EFV) |
HIV-1 (First-line alternative) |
400 mg or 600 mg once daily (at bedtime) |
Severe psychiatric disorders, 1st trimester pregnancy (historical caution) |
CNS effects (vivid dreams, dizziness, depression), rash, hepatotoxicity. |
| Nevirapine (NVP) |
HIV-1, PMTCT (neonatal prophylaxis) |
200 mg once daily for 14 days, then 200 mg twice daily |
High CD4 count in women (>250) or men (>400) due to fatal hepatotoxicity risk |
Severe hepatotoxicity, Stevens-Johnson syndrome (severe rash). |
| Rilpivirine (RPV) |
HIV-1 (Viral load < 100,000) |
25 mg once daily (with a full meal) |
Use with Proton Pump Inhibitors (PPIs) completely contraindicated |
Depression, insomnia, rash, QTc prolongation. |
Common Side Effects of NNRTIs:
- Rash (skin reaction — very common and potentially fatal with Nevirapine).
- Liver problems (hepatotoxicity — especially with Nevirapine in patients with high CD4 counts).
- Central Nervous System (CNS) effects: (with Efavirenz): vivid dreams, dizziness, confusion, mood changes, "hangover" feeling in the morning.
- Lipid changes: Total cholesterol and triglycerides go up.
🚨 NURSING ALERT: Nevirapine Rash
NVP rash can be mild or progress to a life-threatening skin peeling condition (Stevens-Johnson syndrome or TEN). If rash appears with a fever, blistering, or mouth sores → STOP THE DRUG IMMEDIATELY. Always start NVP at a lower dose for the first 2 weeks to let the liver adjust, then increase to normal dose.
❓ Clinical Scenario: Efavirenz & Pregnancy/CNS
Case: A 28-year-old woman on an EFV-based regimen tells you she is 8 weeks pregnant.
Nursing Action: EFV is known to be teratogenic (can cause neural tube birth defects) in the first trimester. Furthermore, it can cause severe psychiatric problems (depression, suicidal thoughts). As a nurse, you urgently inform the doctor to switch her to a DTG-based regimen (TDF+3TC+DTG), which is safe in pregnancy and lacks the CNS toxicity.
🧠 MNEMONIC for NNRTIs: "Every Nurse Eats Red Delicious Oranges"
- Efavirenz
- Nevirapine
- Etravirine
- Rilpivirine
- Doravirine
- Oranges (just for the "O" sound to finish the sentence!)
3.3 PIs (Protease Inhibitors)
Pronounced: "Pee-Eyes"
What They Do:
PIs block the protease enzyme. After HIV makes new proteins inside the cell, protease is needed to cut these proteins into the right sizes so new viruses can be assembled. PIs stop this cutting process. Think of it like a pair of scissors — PIs take away the scissors, so the virus parts cannot be put together properly.
How They Work (Detailed Pharmacology):
- HIV translates its genetic code into long, inactive "polyproteins" (like a long, uncut string of sausages).
- The viral protease enzyme specifically cleaves (cuts) these polyproteins into smaller, functional structural proteins and enzymes.
- These pieces are needed to build the core of new, mature HIV viruses.
- PIs bind directly to the active site of the protease enzyme.
- Because protease cannot cut the protein chains, the new HIV viruses that bud from the cell are immature, defective, and non-infectious. Result: HIV cannot spread to other cells.
| Generic Name |
Abbreviation |
Brand Name |
Key Notes |
| Lopinavir/Ritonavir |
LPV/r |
Kaletra |
Commonly used in children (available as liquid/pellets). Causes severe diarrhea. |
| Atazanavir/Ritonavir |
ATV/r |
Reyataz + Norvir |
Can cause harmless but visible jaundice (yellow eyes) and kidney stones. |
| Darunavir/Ritonavir |
DRV/r |
Prezista + Norvir |
Preferred PI in 2026 WHO guidelines due to high barrier to resistance. |
| Ritonavir |
RTV |
Norvir |
Used strictly as a "booster," not alone for its antiviral effect. |
PI Clinical Summary: Drugs, Indications, Dosages, Contraindications & Side Effects
| Common Drugs |
Indications |
Standard Adult Dosages |
Contraindications |
Major Side Effects |
| Lopinavir/Ritonavir (LPV/r) |
HIV-1 (Second-line, Pediatric first-line) |
400/100 mg twice daily |
Co-administration with amiodarone, simvastatin, rifampicin (without dose adjustment) |
Severe diarrhea, hyperlipidemia, insulin resistance, PR/QT prolongation. |
| Atazanavir/Ritonavir (ATV/r) |
HIV-1 (Second-line alternative) |
300/100 mg once daily |
Co-administration with PPIs (requires stomach acid for absorption) |
Indirect hyperbilirubinemia (jaundice), nephrolithiasis (kidney stones), cholelithiasis. |
| Darunavir/Ritonavir (DRV/r) |
HIV-1 (Second/Third-line preference 2026) |
800/100 mg once daily |
Severe hepatic impairment, sulfa allergy (caution) |
Hepatotoxicity, skin rash, hyperlipidemia. |
Common Side Effects of PIs (Think "Metabolic Syndrome"):
- Diarrhea (very common with LPV/r).
- Nausea and vomiting.
- Lipid abnormalities: High cholesterol, high triglycerides. PIs interfere with lipid metabolism in the liver.
- Insulin resistance: Can lead to hyperglycemia and clinical diabetes.
- Fat redistribution (Lipodystrophy): Buffalo hump on the back, big belly (visceral fat), but thin arms/legs and sunken cheeks.
- Kidney stones and Jaundice (specifically with Atazanavir).
🚨 NURSING ALERT: PI and Drug Interactions
PIs interact with MANY other drugs because they drastically affect the CYP3A4 enzyme system in the liver. Always check for drug interactions before prescribing! Common dangerous interactions include statins (cholesterol drugs - can cause severe muscle breakdown), erectile dysfunction drugs, and some TB drugs (rifampicin drops PI levels to zero!).
❓ Clinical Scenario: PI Side Effects
Case: A 50-year-old man on LPV/r comes to the clinic with severe diarrhea (5–6 watery stools per day) and high cholesterol.
Nursing Action: As a nurse, you educate him about taking his medication WITH food to significantly reduce stomach upset. You also advise him to reduce fatty foods and increase dietary fiber. The doctor may add a cholesterol-lowering drug (statin), but you must strictly check for interactions first (e.g., Atorvastatin dose must be lowered; Simvastatin is totally contraindicated!).
🧠 MNEMONIC for PIs: "Lions And Dragons Roar"
- Lopinavir
- And (Atazanavir)
- Darunavir
- Ritonavir (the booster)
3.4 INSTIs (Integrase Strand Transfer Inhibitors)
Pronounced: "In-Stees"
What They Do:
INSTIs are the newest and best class of ARVs. They block the integrase enzyme, which HIV uses to insert its DNA into the human cell's DNA. Think of it like a thief trying to break into a house — INSTIs lock the door so the thief cannot get inside.
How They Work (Detailed Pharmacology):
- After reverse transcription, a double-stranded HIV DNA is formed in the cytoplasm.
- The integrase enzyme grabs this HIV DNA and carries it into the cell nucleus.
- Integrase then performs "strand transfer"—it cuts the human DNA and pastes the HIV DNA permanently into the host chromosome. Once integrated, the cell becomes a permanent HIV factory.
- INSTIs bind to the active site of the integrase enzyme, paralyzing it. HIV DNA stays outside the nucleus and eventually degrades. The human cell is saved from being hijacked!
| Generic Name |
Abbreviation |
Brand Name |
Key Notes |
| Dolutegravir |
DTG |
Tivicay |
Preferred first-line anchor drug in Uganda and globally. |
| Bictegravir |
BIC |
Biktarvy |
Very effective, minimal side effects (co-formulated). |
| Raltegravir |
RAL |
Isentress |
First INSTI approved. Dosed twice daily (less convenient). |
| Cabotegravir |
CAB |
Vocabria |
Long-acting injectable (given every 2 months!). |
INSTI Clinical Summary: Drugs, Indications, Dosages, Contraindications & Side Effects
| Common Drugs |
Indications |
Standard Adult Dosages |
Contraindications |
Major Side Effects |
| Dolutegravir (DTG) |
HIV-1 (First-line preferred) |
50 mg once daily |
Co-administration with dofetilide (antiarrhythmic) |
Insomnia, weight gain, headache, rare hepatic toxicity. |
| Bictegravir (BIC) |
HIV-1 (Used in fixed-dose combo) |
50 mg once daily |
Co-administration with dofetilide or rifampicin |
Weight gain, nausea, headache, diarrhea. |
| Raltegravir (RAL) |
HIV-1 (Alternative/PEP) |
400 mg twice daily OR 1200 mg once daily |
Hypersensitivity |
Myopathy, rhabdomyolysis, insomnia, rash. |
Why DTG is the BEST Choice (Uganda & WHO 2026):
- High barrier to resistance: HIV finds it very hard to mutate and become resistant to DTG.
- Rapid viral suppression: Viral load drops significantly faster than with EFV or PIs.
- Fewer side effects: Much better tolerated than EFV (no nightmares/depression).
- Once-daily dosing: Easy for patients to remember, promoting adherence.
- Low drug interactions: Safer to use with other medications.
- Safe in pregnancy: Fully approved for pregnant and breastfeeding women.
- Low cost: Affordable for massive public health programs like Uganda's.
Common Side Effects of INSTIs:
- Insomnia (difficulty sleeping - usually passes after a few weeks).
- Headache, mild nausea, dizziness.
- Weight gain: Especially pronounced in women and when combined with TAF.
- Liver enzyme elevation (rare).
🚨 NURSING ALERT: Weight Gain with DTG
Some patients gain significant weight (5-10 kg) on DTG. Monitor weight and BMI at every visit. Encourage a healthy diet and aerobic exercise. Do NOT stop the drug — this weight gain is manageable and is partly due to a "return to health" phenomenon as the virus stops burning the body's calories.
❓ Clinical Scenario: DTG Side Effects
Case: A 35-year-old woman starts TDF+3TC+DTG (TLD). After 3 months, her viral load is completely undetectable, but she has gained 5 kg. She is very worried about her body image.
Nursing Action: As a nurse, you enthusiastically celebrate her undetectable viral load! Reassure her that weight gain is a known side effect of DTG and shows the medicine is working. You counsel her on portion control, reducing sugary drinks, and walking 30 minutes daily. You schedule her for weight monitoring every month.
🧠 MNEMONIC for INSTIs: "Doctor Bic Rides Cars"
- Dolutegravir
- Bictegravir
- Raltegravir
- Cabotegravir
3.5 Entry Inhibitors
What They Do: These drugs stop HIV from entering the CD4 cell in the first place. They are like guards at the gate who refuse to let HIV inside.
Types of Entry Inhibitors:
- Fusion Inhibitor (Enfuvirtide / T-20): Blocks the viral envelope from fusing with the CD4 cell membrane. Given by subcutaneous injection twice daily. Side effects include severe injection site reactions (pain, redness, nodules).
- CCR5 Antagonist (Maraviroc): Blocks the human CCR5 co-receptor on CD4 cells. HIV cannot latch on. Pharmacological catch: Requires a "tropism test" first to ensure the patient's specific HIV strain actually uses CCR5 (and not CXCR4). Side effects include liver toxicity.
Usage: These are NOT first-line drugs. They are used only in special salvage cases (third-line or heavy resistance).
Entry Inhibitors Clinical Summary: Drugs, Indications, Dosages, Contraindications & Side Effects
| Common Drugs |
Indications |
Standard Adult Dosages |
Contraindications |
Major Side Effects |
| Maraviroc (MVC) |
CCR5-tropic HIV-1 (Salvage therapy) |
150, 300, or 600 mg twice daily (depends on interacting drugs) |
CXCR4-tropic HIV, severe renal impairment |
Hepatotoxicity (severe), upper respiratory infections, rash. |
| Enfuvirtide (T-20) |
HIV-1 Treatment-experienced (Salvage) |
90 mg subcutaneously twice daily |
Hypersensitivity |
Injection site reactions (98% of patients), bacterial pneumonia, hypersensitivity. |
3.6 Pharmacokinetic Boosters
What They Are: These are NOT ARVs themselves. They are drugs that slow down the breakdown of other ARVs (especially PIs) in the liver, making them work longer and better.
How They Work: The liver uses the CYP3A4 enzyme to destroy drugs. Boosters forcefully inhibit (block) this enzyme. As a result, the main ARV stays in the blood at high concentrations for 24 hours. This allows for lower doses of the main ARV and once-daily dosing!
Drugs in this Class:
- Ritonavir (Norvir): The original booster.
- Cobicistat (Tybost): A newer booster used for PIs and INSTIs.
PK Boosters Clinical Summary: Drugs, Indications, Dosages, Contraindications & Side Effects
| Common Drugs |
Indications |
Standard Adult Dosages |
Contraindications |
Major Side Effects |
| Ritonavir (RTV) |
Boosting agent for PIs (LPV, ATV, DRV) |
100-200 mg per day alongside the primary PI |
Co-administration with amiodarone, simvastatin, rifampicin (massive CYP3A4 interactions) |
GI intolerance (nausea/diarrhea), lipid abnormalities, circumoral paresthesia (tingling around mouth). |
| Cobicistat (COBI) |
Boosting agent for INSTIs (Elvitegravir) or PIs (DRV, ATV) |
150 mg once daily alongside primary drug |
Co-administration with highly dependent CYP3A4 drugs |
Slight increase in serum creatinine (without actual renal failure), GI upset. |
🚨 NURSING ALERT: Ritonavir and Drug Interactions
Because Ritonavir intentionally breaks the liver's drug-clearing enzyme, it interacts with ALMOST EVERYTHING. Always ask patients about ALL medications they take, including herbal remedies. Common dangerous interactions: TB drugs (rifampicin), hormonal contraceptives (makes them fail!), and statin cholesterol drugs.
MODULE 4: ARV REGIMENS USED IN UGANDA
4.1 First-Line ART Regimens
What is First-Line? First-line regimens are the FIRST combination of drugs given to a person newly diagnosed with HIV. Uganda follows WHO guidelines.
PREFERRED FIRST-LINE REGIMEN (Adults & Adolescents ≥30 kg):
TLD = TDF + 3TC + DTG
- TDF = Tenofovir Disoproxil Fumarate (NRTI Backbone)
- 3TC = Lamivudine (NRTI Backbone)
- DTG = Dolutegravir (INSTI Anchor)
Why TLD is Preferred:
- One pill, once daily (Fixed Dose Combination).
- High effectiveness & high barrier to resistance.
- Fewer side effects than EFV (Efavirenz).
- Safe in pregnancy and breastfeeding.
- Affordable for Uganda's national program.
Dosing Instructions: One tablet once daily, with or without food. Take at the SAME TIME every day.
| Alternative Regimen |
When to Use It (Clinical Rationale) |
| TAF + FTC + DTG |
If the patient develops severe kidney disease or bone osteoporosis from TDF. |
| TDF + 3TC + EFV 400mg |
If DTG is totally out of stock or specifically contraindicated. |
| ABC + 3TC + DTG |
If TDF is contraindicated (e.g., existing kidney disease with GFR < 60 mL/min). |
When to Use EFV Instead of DTG:
- Severe depression or active psychosis (DTG rarely can worsen mood).
- Neurological disease where DTG side effects cannot be assessed.
- Concurrent use of benzodiazepines or carbamazepine (seizure drugs that interact heavily).
- Severe liver disease.
- HIV/TB co-infection using bedaquiline (MDR-TB drug).
- When hormonal contraception is the only family planning method available (though guidelines on this are constantly evolving).
When to Use ABC (Abacavir) Instead of TDF:
- Kidney disease (GFR < 60 mL/min). TDF destroys tubules; ABC is safely metabolized by the liver.
- Adolescents below 35 kg.
Crucial Clinical Rule: You MUST test for the HLA-B*5701 gene first! If the patient is positive, NEVER give ABC. It will trigger a massive Type IV Hypersensitivity reaction (fever, rash, respiratory failure) that is frequently fatal upon rechallenge!
4.2 First-Line for Special Populations
Pregnant and Breastfeeding Women:
- Preferred: TDF + 3TC + DTG (Exactly the same as adults).
- Start ART on the SAME DAY as diagnosis to protect the baby!
- Viral load is checked at 3 months after starting, then every 3 months until the end of breastfeeding.
- If already on TLE (TDF+3TC+EFV) and viral load is perfectly suppressed, stay on it until 6–9 months postpartum, then seamlessly switch to TLD.
Children Under 3 Years:
- Preferred: ABC + 3TC + LPV/r
- LPV/r is preferred because it comes in a liquid/pellet formulation (easier to swallow) and has a very high barrier to resistance for babies who spit up medicine.
Children 3–10 Years:
- Preferred: ABC + 3TC + EFV (or DTG if available in pediatric dosing).
- Use NVP only if EFV is strictly contraindicated.
4.3 Second-Line ART Regimens
When Do We Switch to Second-Line?
- When viral load is NOT suppressed after intensive adherence counseling.
- When there is confirmed treatment failure (defined as two consecutive viral loads > 1,000 copies/mL).
- When there is severe drug toxicity that cannot be medically managed.
Principle of Switching:
- Change the anchor drug (the "third drug") — usually stepping up from an NNRTI/INSTI (EFV/DTG) to a powerful boosted Protease Inhibitor (PI).
- Keep or swap the NRTI backbone (If they were on TDF, switch to AZT. If they were on AZT, switch to TDF).
| If First-Line Was: |
Second-Line Becomes: |
| TDF + 3TC + DTG/EFV |
AZT + 3TC + ATV/r or LPV/r |
| AZT + 3TC + DTG/EFV |
TDF + 3TC + ATV/r or LPV/r |
Note: DRV/r (Darunavir/Ritonavir) is the preferred PI in the 2026 WHO updates! Always use boosted PIs to ensure 24-hour coverage.
4.4 Third-Line ART Regimens
When Do We Use Third-Line?
- When a patient clinically and virologically fails second-line therapy.
- When there is extensive multi-drug resistance.
Third-Line Options:
- Rule: Use drugs from NEW classes the patient has never seen before.
- Requires genotypic resistance testing (mapping the exact mutations in the patient's HIV).
- May include: DRV/r + RAL (Integrase) + ETR (Etravirine), or Entry inhibitors depending on the resistance profile.
❓ Clinical Scenario: Treatment Failure & 3rd Line
Case: A 42-year-old man has been on second-line AZT+3TC+LPV/r for 2 years. His viral load is 45,000 copies/mL. He swears he takes his medication daily.
Nursing Action: As a nurse, you know this is definitive treatment failure. The doctor orders a resistance test. The results show massive resistance to both NRTIs and PIs. The patient is switched to a highly complex third-line regimen with new drugs (e.g., DRV/r + RAL + ETR). You must provide intensive, empathetic adherence counseling because third-line options are limited—if this fails, he has no backup options left!
MODULE 5: NURSING MANAGEMENT OF ARVs
5.1 Before Starting ART (Pre-ART Assessment)
As a nurse, you must meticulously assess the patient BEFORE giving the first dose to prevent fatal complications (like IRIS - Immune Reconstitution Inflammatory Syndrome).
- Clinical Assessment:
- Check for opportunistic infections (TB, cryptococcal meningitis, pneumonia).
- Crucial Rule: If TB or cryptococcal meningitis is present, START treatment for the OI first, then begin ART after 2–8 weeks. (Starting ART immediately wakes up the immune system too fast, causing massive inflammation that can kill the patient).
- Check WHO clinical stage.
- Check CD4 count and viral load.
- Laboratory Tests (and WHY we do them):
- HIV test: Confirm diagnosis before starting lifelong therapy.
- CD4 count & Viral load: Baseline to measure future success.
- Hemoglobin: Check for baseline anemia, especially before prescribing AZT (which causes bone marrow suppression).
- Creatinine and eGFR: Check kidney function before prescribing TDF (which clears through and can damage renal tubules).
- Liver function tests (LFTs): Before prescribing NVP or EFV (hepatotoxic).
- Hepatitis B and C screening: Determines if TDF/3TC should be prioritized (they treat both!).
- HLA-B*5701 test: Before ABC to prevent fatal hypersensitivity.
- Pregnancy test: For women of childbearing age (guides regimen choice/counseling).
- TB screening: (Cough, fever, weight loss, night sweats).
- Psychosocial Assessment:
- Assess readiness to start ART (it is a lifelong commitment).
- Check for depression, anxiety, substance use.
- Assess social support (family, friends, partner).
- Assess disclosure status (who knows their status?).
- Assess food security (do they have food to take with drugs like LPV/r?).
- Adherence Preparation:
- Use the ART readiness checklist.
- Explain that ART is LIFELONG.
- Explain the absolute importance of taking drugs at the SAME TIME every day to prevent viral mutation and resistance.
- Discuss possible side effects and how to manage them. Provide a treatment buddy.
5.2 Patient Education (Counseling Points)
As a nurse, teach EVERY patient the following:
- How to Take ARVs:
- Take at the SAME TIME every day. Do NOT miss doses. Do NOT share drugs with anyone.
- Do NOT stop taking drugs, even if you feel better. (Feeling better means the drugs are working!).
- If you miss a dose, take it as soon as you remember, unless it is almost time for the next dose (do not double dose).
- Food and ARVs:
- DTG, TDF, 3TC (TLD): Can take with or without food.
- EFV: Take on an EMPTY stomach (best at bedtime to sleep through the dizziness/CNS effects).
- LPV/r, ATV/r: Take WITH food (increases absorption and reduces diarrhea).
- RPV (Rilpivirine): MUST take WITH food (needs acidic environment).
- Side Effects to Report Immediately:
- Severe rash with fever or blistering (SJS).
- Yellow eyes or skin (jaundice/liver failure).
- Severe stomach pain with vomiting (pancreatitis/lactic acidosis).
- Shortness of breath. Severe muscle pain or weakness.
- Signs of depression or suicidal thoughts (EFV toxicity).
- Drug Interactions:
- Do NOT take herbal remedies without asking the doctor. Tell the nurse/doctor about ALL other medications.
- Some ARVs interact with TB drugs, contraceptives, and traditional medicines.
- Pregnancy and Breastfeeding:
- DTG is SAFE in pregnancy. Do NOT stop ART during pregnancy.
- Breastfeeding is SAFE while on ART (if viral load is undetectable). The baby will also receive prophylaxis.
- U=U (Undetectable = Untransmittable):
- If viral load is undetectable for 6+ months, you CANNOT transmit HIV through sex. This is a powerful message for reducing stigma!
5.3 Monitoring Patients on ART
Clinical Monitoring (At Every Visit): Weight, Blood pressure, General health and well-being, Signs of opportunistic infections, Side effects of ARVs, Adherence assessment.
| Laboratory Test |
Frequency & Rationale |
| Viral load |
At 3 months after starting, then every 6–12 months. (The absolute gold standard for measuring treatment success). |
| CD4 count |
At baseline, then every 6–12 months (if available). (Measures immune recovery). |
| Creatinine/eGFR |
Every 6 months (if on TDF). |
| Liver function |
Every 6 months (if on NVP or EFV). |
| Lipid profile |
Every 6–12 months (if on Protease Inhibitors). |
| Hemoglobin |
Every 6 months (if on AZT). |
🧠 MNEMONIC for Monitoring: "Viral Counts Create Liver Laughter"
- Viral load
- Counts (CD4 count)
- Create (Creatinine)
- Liver (Liver function)
- Laughter (Lipid profile)
5.4 Managing Common Side Effects
| Side Effect |
Drug(s) Causing It |
Nursing Management |
| Nausea/vomiting |
Most ARVs |
Take with food, small frequent meals, ginger tea. |
| Diarrhea |
LPV/r, most ARVs |
Oral rehydration salts (ORS), increase fluids, low-fat diet. |
| Headache & Insomnia |
EFV, DTG |
Paracetamol, rest, hydration. Take EFV at bedtime, avoid caffeine. |
| Rash |
NVP, EFV |
Mild: antihistamines; Severe: stop drug, refer immediately. |
| Weight gain |
DTG, TAF |
Diet counseling, exercise, monitor weight. |
| Lipodystrophy |
d4T (old), PIs |
Switch drug if possible, exercise. |
| Kidney & Bone problems |
TDF |
Monitor creatinine, calcium, vitamin D. Switch to TAF. |
| Liver problems |
NVP, EFV, PIs |
Monitor LFTs, stop if severe. |
5.5 Adherence Support
Why Adherence is CRITICAL: Missing even a few doses drops the drug concentration in the blood. HIV rapidly mutates to survive this low drug level, leading to drug resistance. Once resistance develops, the drug may NEVER work again. Uganda has limited and expensive third-line options.
Strategies to Improve Adherence:
- Education: Explain WHY adherence matters. Use visual aids/diagrams. Involve family members or treatment buddies.
- Practical Support: Pillboxes with days of the week, phone alarms, community health worker linkage.
- Address Barriers: Transport (Provide multi-month drugs), Stigma (Counsel on disclosure, provide privacy), Side effects (Manage early), Mental health (Screen for depression).
- Differentiated Service Delivery (DSD): Stable patients (viral load suppressed > 1 year) can get:
- Longer drug refills (3–6 months)
- Community drug distribution / Fast-track refill lines
- Reduced clinic visits and Peer support groups.
MODULE 6: PHARMACOVIGILANCE (DRUG SAFETY MONITORING)
What is Pharmacovigilance? It means "watching over drugs" — monitoring and reporting side effects to keep patients safe. In Uganda, ARVs are given to millions of people. New drugs (like DTG) need ongoing safety monitoring because rare side effects may only appear after long-term population use. Reporting via the "Yellow Card System" helps improve national guidelines.
6.2 Common Drug Toxicities (High Yield!)
| Toxicity |
Signs/Symptoms |
Common Causes |
Nursing Action |
| Anemia |
Pale skin, fatigue, shortness of breath |
AZT |
Check hemoglobin, switch drug if severe. |
| Liver toxicity |
Yellow eyes/skin, dark urine, abdominal pain |
NVP, EFV, PIs, TB drugs |
Stop drug, check LFTs. |
| Kidney toxicity |
Swelling, reduced urine, fatigue |
TDF |
Check creatinine, switch to TAF. |
| Lactic acidosis |
Deep breathing, muscle pain, weakness |
d4T, AZT |
EMERGENCY — stop NRTIs, refer. |
| Hypersensitivity |
Fever, rash, muscle pain, flu-like |
ABC (if HLA-B*5701 positive) |
STOP immediately, never rechallenge! |
| Psychiatric effects |
Depression, suicidal thoughts, vivid dreams |
EFV |
Switch to DTG. |
How to Report: Recognize → Document → Report (Yellow card) → Manage → Follow up.
MODULE 7: SPECIAL CONSIDERATIONS FOR UGANDAN COMMUNITIES
7.1 HIV and TB Co-Infection:
- Why It Matters: TB is the leading cause of death among people with HIV in Uganda (~40% co-infection rate).
- Management: Screen ALL HIV patients for TB at every visit. If TB is diagnosed, start TB treatment FIRST. Start ART 2–8 weeks after starting TB treatment.
- Drug Interactions: Rifampicin (TB drug) heavily induces CYP3A4, destroying ARV levels. Use rifabutin instead if available. If not, and patient needs a PI, use double-dose LPV/r.
7.2 HIV and Hepatitis B Co-Infection:
- Management: Screen ALL HIV patients for Hepatitis B. If positive, specifically use TDF + 3TC (or FTC) in their regimen because these drugs treat BOTH viruses.
- Physiological Danger: NEVER stop TDF or 3TC suddenly in Hep B patients! The Hepatitis B virus will rebound massively, causing a severe, potentially fatal "hepatic flare" (liver failure).
7.3 Prevention of Mother-to-Child Transmission (eMTCT):
- The Four Approaches: 1. Primary prevention, 2. Prevent unintended pregnancies, 3. Prevent transmission (ART), 4. Treatment and support.
- For the Baby: All HIV-exposed babies get NVP (Nevirapine) prophylaxis for 6 weeks (low risk) or 12 weeks (high risk). High-risk babies get triple drug prophylaxis (ABC + 3TC + LPV/r).
- Testing the Baby: DNA PCR testing at 4–6 weeks, 9 months, and 6 weeks after stopping breastfeeding. Rapid antibody test at 18 months.
7.4 Adolescents and Young People:
- Challenges: Stigma, difficulty disclosing status, peer pressure, substance use, transitioning to adult care.
- Nursing Strategies: Adolescent-friendly clinic hours, peer support groups, comprehensive sexuality education, tech reminders (SMS).
MODULE 8: EXAM TIPS AND QUICK REVIEW
| Key Fact |
Exam Answer |
| Preferred first-line in Uganda (adults) |
TDF + 3TC + DTG (TLD) |
| Preferred first-line in pregnancy |
TDF + 3TC + DTG |
| Preferred first-line in children <3 years |
ABC + 3TC + LPV/r |
| When to start ART |
SAME DAY as diagnosis (if no TB/crypto) |
| Goal of ART |
Undetectable viral load |
| What does U=U mean? |
Undetectable = Untransmittable |
| Test before giving ABC |
HLA-B*5701 |
| Most common side effect of LPV/r |
Diarrhea |
| Most common side effect of EFV |
Vivid dreams, dizziness |
| Drug to avoid in first trimester |
EFV |
MODULE 9: CLINICAL SCENARIOS FOR PRACTICE
🩺 Scenario 1: Newly Diagnosed Adult
Case: John, 28 years old, is newly diagnosed with HIV. His CD4 is 320, viral load is 45,000. He has no TB symptoms. He is not pregnant.
Answer: Start TLD (TDF + 3TC + DTG) same day. Counsel on adherence and side effects (insomnia, weight gain). Schedule viral load at 3 months. Provide condoms.
🩺 Scenario 2: Pregnant Woman with TB symptoms
Case: Mary, 24 years old, is 16 weeks pregnant and newly diagnosed with HIV. She has a cough and fever.
Answer: Screen for TB immediately. If NO TB: Start TLD same day. If TB is found: Start TB treatment first, start ART after 2 weeks. Counsel on exclusive breastfeeding for 6 months and ensure baby gets NVP prophylaxis at birth.
🩺 Scenario 3: Suspected Treatment Failure
Case: Peter has been on TLD for 2 years. His viral load is 8,500 copies/mL. He says he takes his drugs every day.
Answer: Do NOT switch immediately! Provide Intensive Adherence Counseling (IAC) for 3 months. Repeat viral load. If still not suppressed → switch to second-line (AZT + 3TC + ATV/r or LPV/r). Since he is on DTG, true resistance is rare — poor adherence is highly likely the real cause.
🩺 Scenario 4: Side Effect Management
Case: Grace, 35, on TLD for 6 months, complains she cannot sleep and has gained 7 kg. She wants to stop the drugs.
Answer: Reassure her — do NOT stop ART. For Insomnia: Take DTG in the morning instead of evening. For Weight gain: Counsel on diet and brisk walking. Monitor weight monthly.
MODULE 10: THE NURSE'S ROLE IN ARV THERAPY
10.1 Core Nursing Responsibilities:
- Screening & Testing: Offer tests, link to care.
- Initiation & Counseling: Use readiness checklist, offer same-day start.
- Monitoring & Adherence Support: Track viral load, use pillboxes, manage side effects early.
- Psychosocial & Prevention: Screen for depression, promote U=U, offer family planning.
📋 The 5 Rights of Medication Administration (Applied to ARVs)
- Right Patient: Confirm HIV status, check identity.
- Right Drug: Verify the regimen (TLD vs. TLE).
- Right Dose: One tablet once daily (for most fixed-dose combos).
- Right Route: Oral (swallow with water).
- Right Time: Same time every day! (Crucial for ARVs).
- PLUS the 6th Right: Right Documentation: Record every drug, side effect, and counseling session.
🏆 FINAL EXAM TIP for Pharmacology:
When answering pharmacology questions about ARVs, always structure your thought process:
- Mechanism: Which step of HIV life cycle does it block?
- Side effects: What should the nurse monitor for? (e.g., Creatinine for TDF).
- Interactions: What other drugs affect it? (e.g., Rifampicin vs. PIs).
- Nursing implications: What must the nurse teach, assess, and document?
REFERENCES
- World Health Organization (WHO) Consolidated Guidelines on HIV Prevention, Testing, Treatment, Service Delivery and Monitoring (2021/2026 updates).
- Ministry of Health Uganda: Consolidated Guidelines for the Prevention and Treatment of HIV and AIDS.
- Standard Nursing Pharmacology Textbooks on Antiretroviral Mechanisms and Patient Management.