
By the end of this session, you should be able to:
- Define disease in simple public-health language.
- Classify diseases by cause, duration, transmission, and public-health importance.
- Distinguish communicable from non-communicable diseases.
- Describe disease patterns by person, place, and time.
- Prepare a simple descriptive epidemiology summary and a line list.
🎯 Ultimate Goal: By the end, you should be able to describe a community health problem clearly — because good description prevents confusion and supports action.
🧠 From Day 1 to Day 2: Day 1 asked: "What is happening?" Day 2 asks: "What type of disease is it?" Then: "Who is affected? Where? When?" Classification gives names; description gives patterns.
Disease classification helps nurses communicate clearly, decide urgency, and choose prevention measures. When you know what type of disease you are facing, you know what toolbox to open.
A disease is an abnormal condition that affects the body or mind and can reduce normal functioning. It is a departure from a state of complete physical, mental, and social well-being.
- Infectious: Malaria, tuberculosis (TB), measles, cholera, HIV/AIDS.
- Chronic / Metabolic: Hypertension, diabetes mellitus, obesity.
- Nutritional: Anaemia, malnutrition, vitamin A deficiency.
- Mental / Behavioural: Depression, substance-use disorder, anxiety.
- Genetic: Sickle cell disease, haemophilia, cystic fibrosis.
- Injury: Road traffic injuries, burns, falls.
💡 Key Insight: Disease is not just "being sick." It includes any condition that interferes with normal functioning — whether infectious, chronic, mental, or injury-related. A nurse must recognize all forms.
Classification is not just academic — it is a practical tool for action:
- To communicate the problem clearly: Saying "there is a measles outbreak" is more actionable than "children are sick."
- To choose the right prevention strategy: Vaccines for measles, nets for malaria, lifestyle change for hypertension.
- To plan resources: Drugs, staff, vaccines, lab supplies, hospital beds.
- To decide whether urgent public-health action is needed: One case of Ebola needs an emergency response; one case of hypertension needs clinic follow-up.
- To compare disease patterns across communities: Is our malaria rate higher than the neighbouring district? Why?
🏥 Example: Measles needs isolation and vaccination response; hypertension needs long-term care and lifestyle counselling. You cannot swap the responses. Classification tells you which playbook to use.
Understanding the cause (aetiology) of a disease tells us where to intervene. Here are the main categories:
| Cause Category | Simple Meaning | Examples |
|---|---|---|
| Infectious | Caused by living organisms (bacteria, viruses, parasites, fungi) that invade the body. | Malaria, TB, cholera, measles, HIV, pneumonia. |
| Nutritional | Due to deficiency or excess of nutrients. | Anaemia (iron deficiency), obesity (excess), kwashiorkor (protein deficiency). |
| Genetic / Inherited | Passed from parents to children through genes. Not contagious. | Sickle cell disease, haemophilia, Down syndrome. |
| Environmental | Related to surroundings — physical, chemical, or biological. | Lead poisoning, heat stroke, asthma from air pollution, snake bites. |
| Behavioural / Lifestyle | Linked to personal habits and choices. | Smoking-related lung disease, alcohol-related liver disease, sedentary lifestyle obesity. |
| Trauma / Injury | Caused by external physical force. | Road traffic injuries, burns, fractures, drowning. |
⚠️ Important Note: Many diseases have multiple causes. TB is infectious, but malnutrition and overcrowding (environmental/social) make it worse. Diabetes is partly genetic, but obesity (lifestyle) triggers it. Classification by cause helps us identify the main target for prevention.
How long a disease lasts affects how we manage it, what resources we need, and how we counsel patients.
| Type | Meaning | Examples |
|---|---|---|
| Acute | Starts quickly, lasts a short time (hours to days). Often severe but self-limiting or treatable. | Diarrhoea, malaria attack, food poisoning, flu, appendicitis. |
| Subacute | Between acute and chronic. Develops over weeks. Less sudden than acute, less persistent than chronic. | Subacute bacterial endocarditis, some forms of thyroiditis. |
| Chronic | Long-lasting (months to years, often lifelong). Requires ongoing management. | Hypertension, diabetes mellitus, asthma, HIV (if untreated), arthritis. |
| Recurrent | Comes and goes repeatedly. The person recovers between episodes but the disease returns. | Repeated malaria episodes (especially in high-transmission areas), asthma attacks, herpes simplex. |
📝 Exam Tip: When classifying by duration, ask: "How fast did it start? How long does it last? Does it come back?" Acute diseases need rapid response; chronic diseases need long-term care plans and patient education.
This classification is critical for communicable diseases because it tells us exactly how to break the chain of infection.
| Type | Meaning | Examples |
|---|---|---|
| Communicable | Can spread from person, animal, or environment to another person. Requires an infectious agent and a route of transmission. | Measles, TB, cholera, HIV, scabies. |
| Non-communicable | Does not spread directly from person to person. Caused by genetics, lifestyle, environment, or ageing. | Hypertension, diabetes, cancer, stroke, sickle cell disease. |
| Vector-borne | Spread through living organisms (vectors) that carry the pathogen from one host to another. | Malaria (Anopheles mosquito), dengue (Aedes mosquito), sleeping sickness (tsetse fly). |
| Water / food-borne | Spread through contaminated water or food. Often causes diarrhoeal diseases. | Cholera, typhoid, dysentery, hepatitis A. |
| Airborne / droplet | Spread through tiny respiratory droplets or dust particles in the air. Highly contagious in crowded settings. | TB, measles, influenza, COVID-19, pertussis (whooping cough). |
| Blood / body fluids | Spread through contact with infected blood, semen, vaginal fluids, or other body fluids. | HIV, hepatitis B and C, syphilis. |
💡 Mnemonic — Transmission Routes: "Airborne Water Vectors Blood Direct" = AWVBD. Think: "A Wise Veterinarian Blood Doctor." Each letter reminds you of a major transmission route.
Not all diseases are equal in terms of public health priority. We classify them by how much they threaten the community:
- Common: Affects many people. High burden on the health system. Example: Malaria, respiratory infections.
- Severe: Causes disability, complications, or death. Example: Ebola, cerebral malaria, stroke.
- Epidemic-prone: Can spread quickly and cause outbreaks. Example: Measles, cholera, influenza, meningitis.
- Preventable: Action can reduce or eliminate cases. Example: Vaccine-preventable diseases, many water-borne diseases.
- Priority / Notifiable: Requires surveillance, mandatory reporting, or immediate response. Example: All epidemic-prone diseases, maternal deaths, road traffic injuries (in some countries).
⚠️ Important: A rare disease may still be urgent if it is severe or epidemic-prone. One case of Ebola is a national emergency. One case of hypertension is a clinic appointment. Public-health importance is about population impact, not just individual suffering.
🩺 The Situation: A health centre lists five common problems: malaria, hypertension, measles, anaemia, and road injuries.
Task: Classify each one by cause, duration, transmission, and public-health importance. Which one may need urgent public-health action?
| Condition | Cause | Duration | Transmission | Public-Health Importance |
|---|---|---|---|---|
| Malaria | Infectious (parasite) | Acute / Recurrent | Vector-borne (mosquito) | Common, severe, preventable |
| Hypertension | Lifestyle / Genetic | Chronic | Non-communicable | Common, severe (stroke risk), preventable |
| Measles | Infectious (virus) | Acute | Airborne / droplet | Epidemic-prone, severe, preventable (vaccine) |
| Anaemia | Nutritional (iron deficiency) | Chronic | Non-communicable | Common, preventable (iron supplementation) |
| Road injuries | Trauma / External force | Acute | Non-communicable (injury) | Common, severe, preventable |
Conclusion: Measles may require the most urgent action because it is epidemic-prone — it can spread rapidly among unvaccinated children, causing an outbreak within days. The other conditions are serious but do not spread person-to-person.
The most useful first distinction in nursing and public health is whether a disease can spread between people or through vectors, water, food, or the environment. This single decision changes everything: isolation, contact tracing, reporting, and prevention strategy.
A communicable disease can be transmitted from an infected person, animal, or environment to another person. It requires three things to spread: an infectious agent, a source, and a route of transmission.
- They have an identifiable infectious agent (bacterium, virus, parasite, fungus).
- They can spread through a specific route of transmission (air, water, blood, vector).
- They may produce outbreaks — sudden increases in cases above the expected level.
- Control often requires breaking the chain of transmission (isolation, sanitation, vector control, vaccination).
- Surveillance and reporting are critical — many are notifiable by law.
| Route | How It Spreads | Ugandan Health Examples |
|---|---|---|
| Airborne / Droplet | Tiny particles or droplets from coughing, sneezing, or talking travel through the air. | TB, measles, influenza-like illness, pertussis, COVID-19. |
| Water / Food | Ingestion of contaminated water or food. Often causes diarrhoeal outbreaks. | Cholera, typhoid, dysentery, hepatitis A, food poisoning. |
| Vector-borne | An insect or animal carries the pathogen from one person to another. | Malaria (Anopheles mosquito), dengue, sleeping sickness, plague. |
| Blood / Body Fluids | Contact with infected blood, semen, vaginal fluids, or breast milk. | HIV, hepatitis B, hepatitis C, syphilis. |
| Direct Contact | Skin-to-skin or close physical contact with an infected person or their secretions. | Scabies, impetigo (skin infection), some STIs, Ebola (in late stages). |
📝 Exam Tip — Chain of Infection: To stop a communicable disease, break any link in the chain: Infectious Agent ➔ Reservoir ➔ Portal of Exit ➔ Route of Transmission ➔ Portal of Entry ➔ Susceptible Host. As a nurse, you can break the chain at multiple points: hand hygiene (route), vaccination (susceptible host), isolation (reservoir), safe water (portal of entry).
- Malaria: Vector-borne. Prevent with insecticide-treated nets (ITNs), indoor residual spraying (IRS), and larval source management.
- TB: Airborne. Prevent through early detection, directly observed treatment (DOT), proper ventilation, and cough etiquette.
- Cholera: Water/food-borne. Prevent with safe water, sanitation, handwashing, and oral cholera vaccination in outbreak settings.
- Measles: Highly infectious airborne. Prevent with routine measles vaccination (two doses) and outbreak response vaccination.
💡 Golden Rule: The transmission route tells us exactly where prevention should focus. You do not give mosquito nets for TB. You do not improve ventilation for cholera. Match the intervention to the route.
🩺 The Situation: Six nursing students in one hostel report cough and fever. Two have coughed for more than two weeks. Rooms are crowded and poorly ventilated.
Questions: Is this likely communicable or non-communicable? What information should be collected first?
- Likely communicable until proven otherwise. Cough + fever + shared living space + prolonged duration = red flags for TB or another respiratory infection.
- Information to collect first:
- Exact symptom onset dates for each student.
- Duration of cough (TB suspects: >2 weeks).
- Room allocation — who sleeps where? Shared rooms increase risk.
- Contact history — did any student recently visit a TB patient or work in a clinical area?
- Vaccination history (BCG status).
- HIV status (if known and consented — HIV increases TB susceptibility).
- Immediate actions:
- Refer students with cough >2 weeks for sputum smear microscopy or GeneXpert testing.
- Improve ventilation immediately — open windows, reduce crowding.
- Health education on cough etiquette and hand hygiene.
- Protect confidentiality while acting quickly. Stigma around TB can prevent students from seeking care.
A non-communicable disease does not spread directly from one person to another. It is caused by genetic, physiological, environmental, and behavioural factors, often in combination.
Examples: Hypertension, stroke, diabetes mellitus, cancer, asthma, chronic lung disease, sickle cell disease, mental health disorders.
- Often long-term and costly to manage: A diabetic patient needs lifelong medication, monitoring, and dietary support.
- May have no early symptoms: Hypertension is called the "silent killer" because it often has no warning signs until a stroke or heart attack occurs.
- Complications can be severe: Untreated diabetes leads to blindness, kidney failure, and amputations.
- Prevention requires lifestyle, screening, and follow-up: Not a single pill, but a lifetime of behaviour change.
- Nurses support adherence and patient education: You are the frontline counsellor, monitor, and motivator for NCD patients.
💡 Key Message: NCD control depends on prevention, early detection, and continuity of care. Unlike an acute infection where you treat and discharge, NCDs require building a long-term relationship with the patient.
| Feature | Communicable Disease | Non-Communicable Disease |
|---|---|---|
| Spread | Can spread from source to host (person-to-person, vector, water, air). | Does not spread directly from person to person. |
| Examples | Measles, TB, cholera, malaria, HIV, scabies. | Hypertension, diabetes, cancer, stroke, asthma, sickle cell disease. |
| Time Pattern | May cause sudden outbreaks and epidemics. | Usually a slow, long-term trend over years. |
| Control Strategy | Break transmission chain: isolate, vaccinate, treat, improve sanitation. | Prevent, screen, and manage risk factors: diet, exercise, smoking cessation, medication adherence. |
| Nursing Role | Detect, report, isolate, trace contacts, educate on prevention, administer vaccines. | Screen, counsel, monitor, follow up, support adherence, educate on lifestyle. |
| Reporting | Often mandatory (notifiable diseases). | Usually not mandatory unless part of a surveillance program. |
📝 Exam Tip: In an exam, if you are asked to compare communicable and non-communicable diseases, always mention at least: spread mechanism, examples, time pattern, control strategy, and nursing role. This shows comprehensive understanding.
🩺 The Situation: During a community outreach, 18 of 80 adults screened have high blood pressure. Most did not know their blood pressure status. Some report frequent headaches.
Questions: Is this communicable or non-communicable? What should the nurse do next?
- This is a non-communicable disease concern. Hypertension is not contagious — it is a chronic cardiovascular condition.
- What the nurse should do next:
- Repeat measurements correctly before classification. One high reading is not a diagnosis. Use proper technique: patient seated, arm supported, correct cuff size, rest 5 minutes before measuring.
- Record three readings on separate occasions if possible. Average them.
- Counsel on lifestyle: reduce salt intake, increase physical activity, limit alcohol, stop smoking, maintain healthy weight.
- Refer high readings according to national guidelines (e.g., systolic ≥140 or diastolic ≥90 on repeated measurement).
- Plan follow-up: schedule return visits, create a patient register for NCD tracking.
- Community education: raise awareness that hypertension is silent but dangerous. Encourage regular screening.
⚠️ Critical Point: A high reading is a signal for assessment, not a final diagnosis from one measurement. Always confirm before labelling a patient as hypertensive.
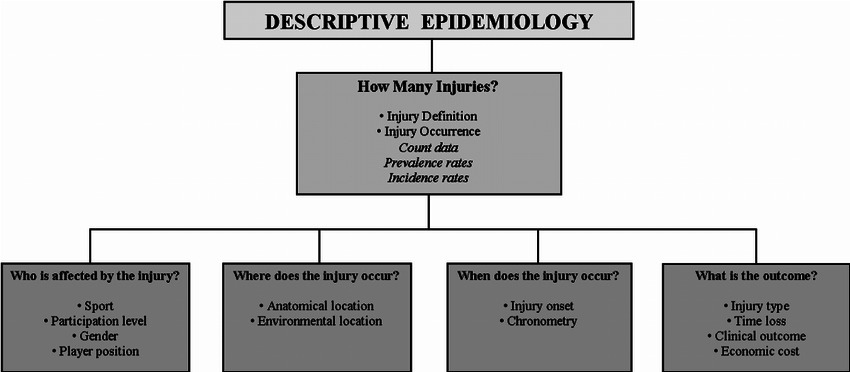
Descriptive epidemiology answers the three fundamental questions: Who is affected? Where are they? When is the problem occurring? It is the first step before you can explain why something is happening.
🧠 Simple Rule: Describe first, explain later. You cannot analyse what you have not described. Descriptive epidemiology is the foundation of all outbreak investigation and health planning.
| Question | Epidemiological Term | What to Describe | Why It Matters |
|---|---|---|---|
| Who? | Person | Age, sex, occupation, class, social status, vaccination status, risk behaviours. | Identifies vulnerable groups and targets interventions. |
| Where? | Place | Village, parish, ward, school, facility, water source, market, road. | Reveals clustering and points to environmental sources. |
| When? | Time | Day, week, month, season, year, date of symptom onset. | Shows trends, seasonality, and whether the problem is spreading. |
💡 Mnemonic: "Who Went Where When?" = 4 Ws (Who, Where, When + What is the disease). Descriptive epidemiology is about answering these questions with data.
Age is one of the most powerful descriptors in epidemiology because it reflects both biological vulnerability and social exposure.
- Under-fives may have more malaria, diarrhoea, pneumonia, and malnutrition because their immune systems are immature and they are often exposed to contaminated environments.
- Adolescents (10-19 years) may face specific reproductive health risks: teenage pregnancy, STIs, substance use, and mental health challenges.
- Adults (20-59 years) may have occupational exposures (farmers ➔ pesticides; health workers ➔ infections) and emerging NCDs (hypertension, diabetes).
- Older adults (60+ years) may have more hypertension, stroke, diabetes, arthritis, and cancers. Ageing reduces immune function and increases chronic disease burden.
❓ Ask: "Which age group carries the greatest burden?" Do not just count cases — calculate rates by age group (cases ÷ population in that age group) to see who is truly most at risk.
Sex (biological) and gender (social roles) influence exposure, risk, and service use in important ways:
- Pregnancy changes malaria risk (pregnant women are more susceptible) and anaemia risk (iron demands increase).
- Men may delay care-seeking for some conditions due to stigma, cost, or cultural norms of toughness.
- Women may face barriers to access or decision-making power — needing permission from a spouse to visit a clinic, for example.
- Biological differences: Women have higher rates of autoimmune diseases; men have higher rates of cardiovascular disease at younger ages.
❓ Ask: "Is the difference biological, social, or related to access?" If more women are diagnosed with depression, is it because women are more depressed, or because men do not seek care? Disaggregating data by sex reveals these patterns.
What people do for a living determines what they are exposed to:
- Farmers: Pesticide exposure, malaria risk (working near breeding sites), snake bites, sun exposure.
- Health workers: Infection exposure (TB, HIV needle-stick injuries), burnout, ergonomic injuries.
- Miners / factory workers: Respiratory hazards (silicosis, asbestosis), noise-induced hearing loss, chemical exposure.
- School children: Shared exposures in classrooms (measles, flu, intestinal parasites), overcrowding, poor sanitation.
- Commercial sex workers: High STI and HIV risk, violence, limited access to care.
❓ Ask: "What does this group do that may increase exposure?" Occupational epidemiology is about linking the job to the disease.
Social status — measured by income, education, housing, or occupation — is a powerful determinant of health:
- Poor households may have unsafe water, crowded housing, poor nutrition, and limited access to healthcare.
- Distance and transport costs may delay treatment. A patient who lives 20 km from the clinic and cannot afford a motorcycle taxi may wait until the disease is severe.
- Education affects health knowledge and service use. Mothers with secondary education are more likely to seek ANC and vaccinate their children.
- Equity matters: Public health is not just about reducing total disease — it is about reducing the gap between the rich and the poor. A disease that only affects the poor is still a public health emergency.
❓ Ask: "Who is most affected and least able to access care?" This is the equity question. It separates clinical medicine from public health.
Describing disease by place helps us see if cases are scattered randomly or clustered around a specific source.
- Describe cases by village, parish, ward, school, or facility.
- Look for clustering near water sources, markets, roads, schools, or swamps.
- Map cases when possible. Even a hand-drawn sketch map with dots for cases can reveal a pattern that tables cannot.
- Place helps target investigation and intervention. If all cases are near one borehole, you test the water. If all cases are in one dormitory, you inspect the ventilation.
❓ Ask: "Are cases scattered or clustered?" Clustering suggests a common source (contaminated water, shared meal, single event). Scattered cases suggest a widespread exposure (seasonal malaria, general poor sanitation).
Time tells us whether the problem is stable, increasing, or seasonal.
- Describe cases by day, week, month, or season.
- Look for sudden increases — a spike above the baseline suggests an outbreak.
- Compare with the usual pattern. Is this normal for this season, or unusual? Malaria peaks in rainy season — that is expected. Malaria peaking in dry season — that is unusual and needs investigation.
- Link timing to rainfall, school terms, religious events, harvest seasons, or mass gatherings.
- Time helps show whether the problem is spreading (propagated outbreak) or static (point source).
❓ Always Ask: "When did the symptoms begin?" Date of onset (when the person first felt sick) is more important than date of arrival at the clinic. A patient who arrived today may have been sick for 5 days — and those 5 days matter for tracing the source.
🩺 The Situation: A primary school reports 24 pupils with diarrhoea in three days. Most cases are in Primary 3 and Primary 4. The school water tank was cleaned last week.
Task: Describe the problem by person, place, and time. What should be checked first?
| Dimension | Description |
|---|---|
| Person | Pupils, especially P3 and P4. Are they sharing a classroom? A teacher? A toilet? A play area? Are they of a specific age (e.g., 8-10 years)? |
| Place | School, specifically classrooms and water points. Is there one shared water tap? One shared latrine? One food vendor? |
| Time | Three-day increase, starting after water-tank cleaning. Did the cleaning introduce contamination? Was chlorine used correctly? Did the tank sit empty and then refill with dirty water? |
- Water source — test for coliform bacteria or chlorine residual.
- Food — was there a shared meal, porridge, or snack?
- Handwashing facilities — are they functional? Is soap available?
- Onset dates — plot an epidemic curve (cases by date of onset) to see if it is a point source (single peak) or propagated (multiple waves).
✅ Key Principle: Immediate prevention can begin before laboratory confirmation when many pupils are at risk. Do not wait for lab results to provide safe water and improve hygiene.
A line list is a table where each row is one patient and each column is a piece of information. It is the most basic and most important tool in outbreak investigation. It turns chaos into organized data.
| Variable (Column) | Why It Matters |
|---|---|
| Name / ID | Avoids duplicate counting. Use initials or a code to protect confidentiality. |
| Age / Class | Describes the person pattern. Helps identify vulnerable groups. |
| Village / Classroom | Describes the place pattern. Reveals clustering. |
| Date of Onset | Describes the time pattern. Essential for the epidemic curve. |
| Symptoms / Test Result | Defines the case. Confirms that all "cases" truly have the same disease. |
| Exposure History | Suggests the possible source. What did they eat? Where did they go? Who did they contact? |
After collecting data, summarize the line list into a clear, actionable description:
| Person / Place / Time | Simple Finding |
|---|---|
| Person | 16 of 24 cases are in P3 and P4 (same age group, shared classroom or teacher). |
| Place | 18 cases are near the same water point (clustering suggests a common source). |
| Time | Cases started two days after tank cleaning (temporal link to an event). |
| Action Signal | Provide safe water immediately and inspect the tank. Do not wait for lab confirmation. |
| Next Step | Collect more data (water test, food history, stool samples) and notify supervisors. |
📝 Exam Tip: When asked to "describe an outbreak," always structure your answer using Person, Place, and Time. Use data from the scenario to support each dimension. Then suggest one immediate action and one next step.
- Count cases by age group, sex, class, or occupation.
- Ask: "Who has the highest number?" (Absolute count)
- Then ask: "Who has the highest risk?" (Rate = cases ÷ population in that group)
- Example: 10 cases in 50 pupils = 20% attack rate. 10 cases in 200 pupils = 5% attack rate. The same number of cases means very different risk. Always calculate rates when you have the denominator.
- List cases by village, ward, school block, or water point.
- Look for clusters around a shared exposure.
- Ask whether places differ in water, sanitation, crowding, or access to services.
- Use a simple sketch map when a formal map is unavailable. Even a hand-drawn map with dots for cases and X for water sources can improve outbreak understanding dramatically.
- Record the date symptoms started — not the date of clinic visit.
- Count cases by day or week.
- Look for a sudden rise (point source outbreak) or slow increase (propagated outbreak).
- Compare with what is normally expected — the baseline.
- Time helps show whether the problem is spreading (person-to-person transmission) or limited to one exposure (common source).
Students now practise describing a suspected outbreak using person, place, and time.
🩺 The Scenario:
- A village reports many children with fever and rash.
- Cases are mainly from two neighbouring schools.
- Some children missed routine immunisation.
- The health team must describe the situation before deciding action.
Task: Work in groups. Describe first, then suggest action.
- Identify which children are affected — by age, sex, class.
- Check vaccination status — this is critical for measles suspicion.
- Ask who is most at risk — unvaccinated children? Children in crowded classrooms?
- Prepare one sentence describing the person pattern.
- Example sentence: "Most cases are among unvaccinated children aged 5–9 years attending Primary School A and Primary School B."
- Place: List cases by school, village, or classroom. Are they clustered in one area?
- Time: List cases by date of rash onset. When did the first case appear? Are new cases still appearing?
- Ask whether cases are clustered (suggesting a common source) or scattered (suggesting widespread transmission).
- Ask whether cases are increasing (epidemic) or stable.
- Prepare one sentence for place and one for time.
- Example sentences: "Cases are clustered in two neighbouring schools in the eastern part of the village." / "Cases began on 3 July and have increased steadily, with 8 new cases reported today."
- Person: Children, especially those not fully immunised.
- Place: Two neighbouring schools and their surrounding villages.
- Time: Cases grouped by date of rash onset, with an increasing trend over the past week.
- Possible exposures: Shared classrooms, playgrounds, or a recent community gathering (funeral, market day, church event).
- Immediate action: Report to the District Health Office, assess all cases clinically, check vaccination coverage in both schools.
- Prevention: Isolate suspected cases (keep them home), support a vaccination response campaign, and conduct active case finding in the community.
💡 Key Principle: Person-place-time description helps the team decide where to investigate and who to protect first. It turns a vague "many children are sick" into a precise, actionable picture.
Fill in the blanks for any descriptive epidemiology problem:
- Health problem: __________________
- Person pattern: __________________
- Place pattern: __________________
- Time pattern: __________________
- Possible exposures: __________________
- Immediate action: __________________
Cover the answers and test yourself. If you can answer these clearly, you are ready for Day 2's exam!
- Define disease in your own words: An abnormal condition that affects the body or mind and reduces normal functioning. It can be infectious, chronic, nutritional, genetic, or injury-related.
Remember: Disease is broader than "infection." - Give two ways of classifying diseases: By cause (infectious, nutritional, genetic, environmental, lifestyle) and by transmission (communicable, non-communicable, vector-borne, water-borne, airborne).
Other valid answers: by duration (acute, chronic) or by public-health importance (common, severe, epidemic-prone). - Give two communicable and two non-communicable diseases:
Communicable: Measles, TB, malaria, cholera, HIV.
Non-communicable: Hypertension, diabetes, cancer, stroke, asthma, sickle cell disease.
Be ready to classify any disease the examiner names. - Explain person, place, and time using one example:
Example: In a school diarrhoea outbreak:
• Person: Pupils in P3 and P4 (age 8-10 years).
• Place: School water point and shared latrine.
• Time: Cases began 2 days after the water tank was cleaned, with a peak on day 3.
Always use a specific scenario — abstract definitions earn fewer marks. - State why a line list is useful: A line list organizes patient data into a simple table (one row per patient, one column per variable). It prevents duplicate counting, reveals person-place-time patterns, and forms the basis for all outbreak analysis.
Mnemonic: Line list = Logical Information Neatly Entered. - What is the difference between a case count and a rate? A case count is the absolute number of people affected. A rate is the number of cases divided by the population at risk, usually expressed as a percentage. A rate tells you the risk; a count alone does not.
Example: 10 cases in a class of 50 = 20% attack rate. 10 cases in a school of 500 = 2% attack rate. Very different situations. - Why is it important to record the date of symptom onset, not just the clinic visit date? The onset date tells you when the person was actually exposed and infectious. The visit date may be days later and does not reflect the true timeline of the outbreak. Onset dates are used to build the epidemic curve.
This is a favourite exam question. Memorize it. - What immediate action should a nurse take when a communicable disease is suspected in a hostel?
1. Do not panic — but act quickly.
2. Collect symptom details, onset dates, and contact history.
3. Refer suspects for testing (e.g., sputum for TB if cough >2 weeks).
4. Improve environmental conditions (ventilation, spacing, hygiene).
5. Educate contacts on signs to watch for.
6. Report to the relevant authority (ward in-charge, DHO).
7. Protect patient confidentiality at all times.
Show the examiner you know both clinical and public health actions.
- World Health Organization (WHO). (2018). Managing Epidemics: Key Facts about Major Deadly Diseases.
- Centers for Disease Control and Prevention (CDC). (2012). Principles of Epidemiology in Public Health Practice (3rd ed.).
- Gordis, L. (2014). Epidemiology (5th ed.). Saunders Elsevier.
- Uganda Ministry of Health. (2021). National Technical Guidelines for Integrated Disease Surveillance and Response (IDSR).
Quick Quiz
Disease Classification Quiz
Epidemiology and Biostatistics - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Disease Classification Quiz
Epidemiology and Biostatistics
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.