
By the end of this session, you should be able to:
- Explain the chain of disease transmission and its six links.
- Describe agents, reservoirs, portals, hosts, and the environment in disease spread.
- Explain vector-borne transmission using malaria as a detailed example.
- Show how immunity (natural, acquired, herd) affects disease spread.
- Identify practical points for prevention and control at every link in the chain.
A disease does not spread by magic. It needs a source, a route, and a susceptible person. Public health action asks: "Where can we interrupt the process?" As a nurse, your job is to spot the weak link and break it.
🩺 The Situation: A village reports many fever cases one week after heavy rains. Several homes have stagnant water nearby. Children are most affected.
Discussion: What information suggests possible disease transmission?
- Cases increased after a clear environmental change: heavy rain. This is a temporal clue — the exposure happened after the rain.
- Stagnant water may support mosquito breeding. This is an environmental clue — the vector's habitat expanded.
- Children may be more susceptible (immature immune systems) or more exposed (playing outdoors, not sleeping under nets, less likely to seek shelter).
- The team should describe cases by person, place, and time (Day 2 skills) before jumping to conclusions.
⚡ Key Principle: Transmission is suspected when cases show a pattern, not because of one patient only. One child with fever after rain is a clinical case. Twenty children with fever after rain near stagnant water is an epidemiological signal.
Disease transmission is the movement of an infectious agent from a source (reservoir) to a susceptible host. It may occur directly (person-to-person) or indirectly (through vectors, water, air, surfaces, or objects). Control focuses on interrupting the movement of the agent at any point along the chain.
The agent is the organism or particle that can cause disease. It is the "weapon" — but a weapon needs a wielder, a target, and a path to travel.
- Bacteria: Single-celled organisms. Examples: Mycobacterium tuberculosis (TB), Vibrio cholerae (cholera), Salmonella typhi (typhoid).
- Viruses: Tiny particles that need a host cell to reproduce. Examples: Measles virus, HIV, Influenza virus, Hepatitis B virus.
- Parasites: Organisms that live on or in a host. Examples: Plasmodium (malaria), Helminths (intestinal worms), Giardia (giardiasis).
- Fungi: Organisms that cause skin, lung, or systemic infections. Examples: Candida (thrush), dermatophytes (ringworm).
- Prions: Abnormal proteins (rare, but important — e.g., Creutzfeldt-Jakob disease).
📝 Exam Tip: When asked to "identify the agent," give the specific name (e.g., Plasmodium falciparum for malaria) and the type (parasite). Do not just say "germ" or "bug."
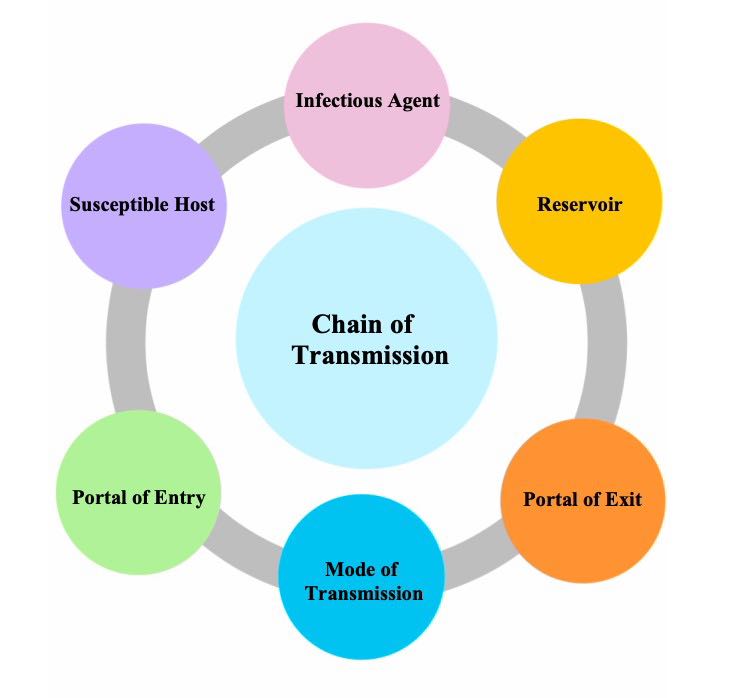
A disease spreads only when all links in the chain are present. Control works by breaking one or more links. You do not need to break every link — just one is enough to stop transmission.
AGENT → RESERVOIR → PORTAL OF EXIT → MODE OF TRANSMISSION → PORTAL OF ENTRY → SUSCEPTIBLE HOST
Break any one link → Transmission stops.
💡 Mnemonic — The Chain of Infection: "All Rabbits Prefer Many Peas Soup" = ARPMPS = Agent, Reservoir, Portal of exit, Mode of transmission, Portal of entry, Susceptible host. Another version: "All Residents Please Move Past Security."
What it is: The microorganism or particle that causes the disease.
Questions to ask:
- What causes the disease? (Bacterium, virus, parasite, fungus?)
- How strong (virulent) is the agent? Some agents need only a few organisms to cause disease (e.g., Shigella — very virulent). Others need many (e.g., Salmonella).
- Can the agent survive outside the body? (e.g., Clostridium difficile forms spores that survive on surfaces for months.)
Control strategies targeting the agent:
- Treatment: Antibiotics for bacteria, antimalarials for parasites, antivirals for viruses.
- Disinfection: Using chlorine, bleach, or alcohol to kill agents on surfaces.
- Sterilisation: Using heat (autoclave) or chemicals to destroy all living organisms on instruments.
- Safe handling of infectious materials: Proper disposal of sharps, soiled dressings, and laboratory waste.
What it is: A reservoir is where the agent normally lives, grows, or survives. It is the "home" of the agent. Without a reservoir, the agent dies out.
Types of reservoirs:
- Human reservoirs: People who are infected and shedding the agent — symptomatic or asymptomatic (carriers). Example: A person with typhoid who works as a cook ("Typhoid Mary").
- Animal reservoirs: Animals that harbour the agent. Example: Bats (Ebola, rabies), rats (Lassa fever), birds (avian influenza), dogs (rabies).
- Environmental reservoirs: Water, soil, food, or surfaces where the agent survives. Example: Unsafe water for cholera, soil for tetanus spores, hospital surfaces for MRSA.
⚠️ Important: A reservoir is not the same as a source. The source is the immediate origin of the agent for a specific case (e.g., the contaminated well that made Patient A sick). The reservoir is the long-term habitat (e.g., all unsafe water in the district). In exams, use "reservoir" when describing the chain of infection.
Control strategies targeting the reservoir:
- Identify and treat infected humans (screening, contact tracing, treatment).
- Isolate infectious patients to prevent them from acting as a reservoir.
- Clean and disinfect environmental reservoirs (water treatment, surface cleaning).
- Control animal reservoirs (vaccinate dogs for rabies, control rat populations).
What it is: The portal of exit is how the agent leaves the reservoir. The agent must have a way out before it can reach a new host.
Examples of portals of exit:
- Respiratory tract: Coughing, sneezing, talking (TB, measles, influenza, COVID-19).
- Gastrointestinal tract: Stool (cholera, typhoid, dysentery, hepatitis A).
- Genitourinary tract: Urine, semen, vaginal fluids (HIV, syphilis, gonorrhoea, schistosomiasis).
- Blood: Needle-stick injuries, transfusions, bites (HIV, hepatitis B, malaria).
- Skin and mucous membranes: Wound discharge, skin lesions, secretions (scabies, impetigo, Ebola).
Nursing actions to reduce portal of exit:
- Wound covering: Dress all open wounds with sterile, waterproof dressings.
- Masks: Patients with cough or TB should wear surgical masks.
- Safe waste handling: Dispose of soiled dressings, stool, and urine safely. Do not let infectious materials contaminate the environment.
- Cough etiquette: Teach patients to cough into their elbow or a tissue, not into the air.
What it is: The mode is how the agent travels from the reservoir (through the portal of exit) to the new host. This is the "bridge" between the old host and the new host.
| Mode | How It Works | Examples & Prevention |
|---|---|---|
| Direct Contact | Physical skin-to-skin or mucous membrane contact with an infected person or their fluids. | Scabies, impetigo, STIs, Ebola. Prevention: Gloves, hand hygiene, safe sexual practices, isolation. |
| Droplet | Larger respiratory particles (>5 microns) travel short distances (usually <1 metre) through coughing, sneezing, or talking. | Influenza, pertussis, meningitis, COVID-19 (in close contact). Prevention: Masks, physical distancing, cough etiquette. |
| Airborne | Tiny particles (<5 microns) or dust remain suspended in air and can travel long distances. Inhaled directly into the lungs. | TB, measles, chickenpox. Prevention: N95 masks, ventilation, negative-pressure rooms, UV light. |
| Food / Water | Ingestion of contaminated food or water. Agent enters through the gastrointestinal tract. | Cholera, typhoid, dysentery, hepatitis A. Prevention: Safe water, sanitation, handwashing, food hygiene, chlorination. |
| Vector-borne | A living organism (vector) carries the agent from one host to another. The agent may multiply or develop inside the vector. | Malaria (mosquito), sleeping sickness (tsetse fly), plague (flea). Prevention: Nets, insecticides, environmental management, larval control. |
| Blood / Body Fluids | Contact with infected blood, semen, vaginal fluids, or other body fluids through needles, sex, childbirth, or transfusions. | HIV, hepatitis B and C, syphilis. Prevention: Safe needles, condoms, screening blood, PPE, safe delivery practices. |
| Fomite / Vehicle | Indirect contact with contaminated objects (bedsheets, utensils, toys, door handles, medical equipment). | Norovirus, MRSA, COVID-19. Prevention: Environmental cleaning, disinfection, single-use equipment. |
📝 Exam Tip — Droplet vs. Airborne: This is a favourite exam trap. Droplet = larger particles, travel short distances, surgical mask is enough. Airborne = tiny particles, travel long distances, need N95/FFP2 respirator and special ventilation. TB and measles are airborne. Influenza is mainly droplet (though some airborne potential exists). Know the difference.
What it is: The portal of entry is how the agent enters the new host. The agent must find a way into the body to cause infection.
Examples of portals of entry:
- Mouth (ingestion): Contaminated food or water enters the GI tract. Example: Cholera, typhoid.
- Nose and lungs (inhalation): Airborne or droplet particles enter the respiratory tract. Example: TB, measles, influenza.
- Broken skin (inoculation): Cuts, wounds, needle-stick injuries, insect bites. Example: HIV (needle-stick), malaria (mosquito bite), tetanus (dirty wound).
- Genital tract: Sexual contact or childbirth. Example: HIV, syphilis, gonorrhoea, chlamydia.
- Placenta (vertical transmission): Mother to unborn baby. Example: HIV, syphilis, rubella, Zika.
- Mucous membranes (eyes, mouth, nose): Splashes of blood or body fluids. Example: Ebola, hepatitis B.
Control strategies targeting portal of entry:
- Hygiene: Handwashing before eating prevents oral entry.
- Protective barriers: Gloves, gowns, goggles, face shields prevent skin and mucous membrane entry.
- Vector control: Nets, repellents, and insecticides prevent mosquito bites (skin entry).
- Safe sex: Condoms prevent genital tract entry of STIs.
- Safe delivery practices: Preventing mother-to-child transmission of HIV and syphilis.
What it is: A susceptible host is a person who can develop the disease if exposed to the agent. Not everyone exposed gets sick — susceptibility varies.
Factors that increase susceptibility:
- Age: Very young (under 5) and very old (over 65) have weaker immune systems.
- Pregnancy: Pregnant women are more susceptible to malaria, listeriosis, and some viral infections.
- Malnutrition: Poor nutrition weakens immune defences. Vitamin A deficiency increases measles severity.
- HIV infection: Destroys CD4 cells, making the body vulnerable to opportunistic infections (TB, cryptococcal meningitis, PCP).
- Chronic diseases: Diabetes, cancer, and kidney disease weaken immunity.
- Lack of vaccination: No acquired immunity means the body has never "learned" to fight that specific agent.
- Stress and fatigue: Physical and emotional stress can temporarily suppress immune function.
- Medical procedures: Surgery, chemotherapy, and steroids can reduce immunity.
Control strategies targeting the susceptible host:
- Vaccination: The most effective way to reduce susceptibility.
- Nutrition support: Iron, vitamin A, and balanced diets strengthen natural immunity.
- Prophylaxis: Giving preventive medication (e.g., cotrimoxazole for HIV patients, IPTp for pregnant women).
- Health education: Teaching people to avoid exposure (sleep under nets, wash hands, use condoms).
- Early treatment: Treating infections promptly prevents complications and reduces spread.
📝 Exam Tip — Chain of Infection in Scenarios: When given a scenario, always identify all six links explicitly. Then state which link you would break first and why. This shows you understand both the theory and the practical application. Example: "In a cholera outbreak, I would break the mode of transmission first by providing safe water and promoting handwashing, because this protects the entire community immediately."
Disease occurrence depends on the interaction between three factors — like a three-legged stool. Remove one leg, and the disease falls.
AGENT (What causes the disease)
+
HOST (Who is affected)
+
ENVIRONMENT (Where it happens)
= DISEASE OCCURS
- Agent: Plasmodium parasite.
- Host: A child who has no net, poor nutrition, and no prior immunity (or a pregnant woman with reduced immunity).
- Environment: Stagnant water after rains, warm temperature, poor housing with no screens.
- Control implication: You can attack any of the three legs. Kill the agent (treatment), strengthen the host (nets, nutrition, vaccines), or change the environment (drain stagnant water, improve housing). The most effective programs attack all three.
💡 Key Insight: The chain of infection (6 links) and the triad (3 factors) are two ways of looking at the same problem. The chain focuses on the process of transmission. The triad focuses on the conditions that allow disease to occur. Both guide prevention. In exams, use whichever framework the question asks for.
🩺 The Situation: A patient with persistent cough is admitted to a crowded ward. Windows are closed and several patients are nearby. A nurse notices no cough mask is being used.
Task: Identify the reservoir, portal of exit, mode of transmission, and first control actions.
| Chain Link | In This Scenario |
|---|---|
| Reservoir | The infected patient (human reservoir). They may have TB, influenza, or another respiratory infection. |
| Portal of Exit | Respiratory droplets or aerosols released during coughing, sneezing, and talking. |
| Mode of Transmission | Droplet (if influenza/COVID-19 close contact) or airborne (if TB or measles). In a crowded, poorly ventilated ward, airborne transmission is highly likely for TB. |
| Portal of Entry | Inhalation through the nose and lungs of nearby patients and staff. |
| Susceptible Hosts | Other patients in the ward (especially those with HIV, malnutrition, or post-surgical status), visitors, and healthcare workers. |
- Mask the patient: Provide a surgical mask for the patient to wear when coughing. If TB is suspected, staff should wear N95 respirators.
- Improve ventilation: Open windows immediately. Turn on fans if available. Airborne pathogens disperse faster in moving air.
- Spacing / Cohorting: Move the patient away from others. If possible, place in a separate room or at least at the far end of the ward. If TB is suspected, isolate in a dedicated TB room.
- Triage: Fast-track the patient for evaluation, sputum testing, and diagnosis. Do not let them wait in a general waiting area.
- Report: Notify the infection control nurse or ward in-charge. Document the observation.
- Health education: Teach the patient cough etiquette (cough into elbow, not hands).
✅ Key Principle: Good nursing observation can prevent spread before laboratory confirmation. You do not need to wait for a lab result to start infection control measures. Act on suspicion.
Breaking the chain of infection follows a simple three-step logic:
- First, identify the likely link in the chain. What is the most obvious weakness? Is it the water source? The lack of nets? The crowded ward?
- Second, choose a safe action that breaks that link. Do not wait for perfect information. Choose an action that is safe, feasible, and likely to help.
- Third, monitor whether cases reduce. If cases continue to rise, you broke the wrong link or not enough links. Reassess and adapt.
⚠️ Important: Control does not always require knowing everything immediately. Start with safe actions that reduce spread. You can refine your strategy as more data comes in. This is called the "precautionary principle" in public health.
Vector-borne diseases are unique because they require a living intermediary — the vector. The vector is not just a passive carrier; it is often essential for the agent's life cycle.
- The vector picks up the agent from an infected host or reservoir (e.g., a mosquito bites a person with malaria).
- The agent survives or develops inside the vector (e.g., Plasmodium undergoes sexual reproduction in the mosquito's gut, then moves to the salivary glands). This is called the extrinsic incubation period.
- The vector transmits the agent during a later bite or contact with a new host (e.g., the infected mosquito bites a new person, injecting parasites with its saliva).
💡 Key Point: Not all mosquitoes transmit malaria. Only female Anopheles mosquitoes do. And they must be infected first. This means controlling the vector is a powerful prevention strategy — if you reduce mosquitoes, you break the chain even if infected people exist.
- Step 1: A female Anopheles mosquito bites a person infected with malaria. The mosquito ingests blood containing Plasmodium gametocytes (the sexual stage of the parasite).
- Step 2: Inside the mosquito's stomach, the gametocytes mature and fuse. The parasite then penetrates the mosquito's gut wall and forms oocysts.
- Step 3: After about 10-14 days (the extrinsic incubation period), the oocysts burst and release sporozoites that travel to the mosquito's salivary glands.
- Step 4: The mosquito bites another person. Sporozoites enter the new person's bloodstream through the mosquito's saliva.
- Step 5: Sporozoites travel to the liver, multiply, then enter red blood cells. The person develops fever, chills, and other symptoms of malaria.
- Rain creates stagnant water — puddles, tyre tracks, blocked gutters, rice paddies — where mosquitoes lay eggs.
- More mosquitoes emerge from these breeding sites, increasing the vector population.
- More contact between vector and humans occurs because mosquitoes are more numerous and people may sleep outdoors or with doors open when it is hot after rain.
- Risk is highest when people lack nets, screens, or timely treatment. A mosquito cannot transmit if it cannot bite (net) or if the person is already treated (reduces reservoir).
📝 Exam Tip: When asked "Why does malaria increase after rain?" always mention three things: (1) breeding sites increase, (2) mosquito population increases, (3) human-mosquito contact increases. Add lack of protection (nets, treatment) for full marks.
🩺 The Situation: Village A has many homes near stagnant water. Village B has fewer breeding sites and high net use. Both villages report fever cases.
Questions: Which village may have higher transmission risk, and what data should be collected?
- Village A likely has higher transmission risk due to abundant breeding sites (environmental factor) and possibly lower net use (host protection factor). The combination of more vectors and less protection creates a "perfect storm."
- Data to collect:
- Number of fever cases per week in each village (count and rate).
- Malaria test results (RDT or microscopy) — not all fever is malaria.
- Age distribution of cases — are children under 5 most affected?
- Insecticide-treated net (ITN) ownership and use rates in each village.
- Map breeding sites — count and type of stagnant water near homes.
- Compare cases over time — is Village A's peak earlier or higher?
- Control actions:
- Agent: Test and treat all confirmed cases promptly. Radical cure (complete treatment) reduces the reservoir.
- Vector: Reduce breeding sites (drain stagnant water, larviciding), promote net use, consider indoor residual spraying (IRS).
- Host: Distribute nets to Village A, promote consistent use, provide intermittent preventive treatment for pregnant women (IPTp).
- Environment: Improve drainage, cover water storage containers, clear vegetation around homes.
💡 Key Principle: Vector-borne control must address the agent, vector, environment, and host simultaneously. Focusing on only one is usually insufficient.
- Recognise unusual increases: Track fever cases and positive malaria tests weekly. A sudden spike is an early warning signal.
- Educate families: Teach proper net use (tuck under mattress, no holes, sleep under it every night, not just sometimes). Explain that nets work best when everyone sleeps under them.
- Environmental control: Advise families to drain stagnant water, cover water containers, and clear bushes near homes.
- Support prompt testing and treatment: Do not let patients wait. A child with fever should be tested within 24 hours. Positive cases should receive ACTs (artemisinin-based combination therapy) according to national guidelines.
- Protect vulnerable groups: Ensure pregnant women receive IPTp and children under 5 sleep under nets.
- Report: Notify the District Health Office if cases exceed expected levels or if treatment stock-outs occur.
🩺 The Situation: Twenty pupils develop diarrhoea within two days. Most drank from the same water tank. The tank was recently cleaned without chlorination.
Question: Which link in the chain should be broken first?
- Suspected mode: Water-borne transmission. The tank is the common source. The lack of chlorination after cleaning allowed contamination to survive or re-enter.
- Immediate action (break the mode of transmission):
- Provide safe water immediately. Do not wait for lab results. Bring bottled water, water trucking, or boil water for the school.
- Stop use of the tank temporarily. Put a lock on it or post a clear warning sign.
- Data collection (while protecting pupils):
- Symptoms — is it watery diarrhoea (cholera suspicion) or bloody (dysentery)?
- Onset dates — plot an epidemic curve. A single peak suggests a point source (the tank). Multiple waves suggest person-to-person spread.
- Class and age — are all classes affected or only those near the tank?
- Water consumed — how much did each pupil drink? Did any pupil NOT drink from the tank and still get sick? (If yes, another source exists.)
- Severity — how many are dehydrated? Any hospitalisations?
- Check water treatment, storage, and handwashing facilities. Was the tank properly sealed after cleaning? Were hands washed before handling the tap? Is there a handwashing station near the latrine?
⚡ Key Principle: Public health action should protect people while investigation continues. Never let children keep drinking suspect water while you wait for laboratory confirmation. Protection comes first.
Immunity is the body's ability to resist or fight infection. It is a critical factor in the chain of infection because it determines whether an exposed person becomes a case.
Before the immune system even "recognises" a specific germ, the body has physical and chemical defences:
- Skin: The largest organ. Intact skin is a nearly impenetrable barrier. Broken skin (cuts, wounds, IV sites) is a major portal of entry.
- Mucous membranes: Line the respiratory, GI, and genitourinary tracts. They trap pathogens in mucus and sweep them away (e.g., cilia in the lungs).
- Stomach acid: Kills most ingested bacteria and parasites. People on antacids or with low acid (achlorhydria) are more susceptible to food-borne infections.
- Normal flora (good bacteria): The gut, skin, and mouth are colonised by harmless bacteria that compete with pathogens for space and nutrients.
- Tears, saliva, and earwax: Contain enzymes (like lysozyme) that destroy bacterial cell walls.
- Keep skin intact — proper wound care, prevent pressure ulcers.
- Promote good nutrition — malnutrition weakens skin integrity and mucous membranes.
- Encourage breastfeeding — breast milk contains antibodies and immune cells that protect infants.
Acquired immunity develops after the body "learns" to recognise a specific pathogen. It is targeted and powerful.
Two types of acquired immunity:
- Active immunity: The body produces its own antibodies after exposure to the pathogen (natural infection) or a vaccine (artificial).
- Natural active: You get measles, recover, and your body remembers how to fight it.
- Artificial active: You receive the measles vaccine. Your body thinks it has seen measles and builds memory without getting sick.
- Advantage: Long-lasting, often lifelong. Memory B and T cells remain ready for decades.
- Passive immunity: You receive pre-made antibodies from another source. Your body does not produce them.
- Natural passive: A mother passes antibodies to her baby through the placenta (IgG) and breast milk (IgA).
- Artificial passive: Injection of immunoglobulin (e.g., rabies immunoglobulin after a dog bite, tetanus antitoxin).
- Advantage: Immediate protection. Disadvantage: Short-lived (weeks to months). No memory formed.
📝 Exam Tip: When asked about immunity types, always distinguish active vs. passive and natural vs. artificial. A common exam question: "A baby is protected from measles for 6 months after birth. What type of immunity is this?" Answer: Natural passive immunity (mother's antibodies via placenta and breast milk).
Herd immunity (also called community immunity) occurs when a large percentage of a population is immune to a disease, either through vaccination or prior infection. This indirectly protects people who are not immune.
- When most people are immune, the infectious agent cannot find enough susceptible hosts to keep spreading.
- The chain of transmission is broken at the host level — not because the vector or environment changed, but because the "fuel" (susceptible people) ran out.
- This protects vulnerable people who cannot be vaccinated: newborn babies, people with severe allergies, immunocompromised patients (e.g., cancer patients on chemotherapy), and the very elderly.
Example — Measles: Measles is one of the most contagious diseases known. It requires about 95% vaccination coverage to achieve herd immunity. If coverage drops to 80%, outbreaks can occur. This is why every unvaccinated child is a risk to the whole community.
Example — Polio: Polio requires about 80-85% coverage for herd immunity. When coverage drops below this, the virus can circulate again — even in countries that were previously polio-free.
⚠️ Critical Point: Low immunisation coverage creates gaps for outbreaks. Herd immunity is not a fixed number — it depends on how contagious the disease is. Nurses must promote vaccination not just to protect the individual, but to protect the entire community. Every vaccination is a public service.
- High immunity can reduce outbreaks and severe disease. Even if cases occur, they are milder because the immune system responds faster.
- Low immunity can allow rapid spread. A population with no prior exposure to a new virus (e.g., COVID-19 in 2020) experiences explosive outbreaks.
- Groups with low immunity may become priority targets for vaccination or protection. In a measles outbreak, unvaccinated children under 5 are the first group to target.
- Waning immunity: Some vaccines or infections do not provide lifelong immunity. Booster doses may be needed (e.g., tetanus every 10 years, some COVID-19 boosters).
- Immune escape: Some pathogens mutate to evade existing immunity (e.g., influenza variants, Omicron COVID-19 variant). This is why new flu vaccines are needed every year.
🩺 The Situation: A school reports suspected measles. Some learners have vaccination cards; others do not. Several children share a crowded classroom.
Questions: Who is most at risk, and what should the health team check first?
- Most at risk: Unvaccinated or partially vaccinated learners. Measles requires two doses of vaccine for full protection. One dose gives about 85% protection; two doses give about 97%.
- Why crowded classrooms matter: Measles is airborne. In a crowded, poorly ventilated room, one infected child can infect 12-18 others. This is the basic reproduction number (R₀) of measles — one of the highest of any disease.
- What the health team should check first:
- Symptoms: Fever, cough, runny nose, red eyes (conjunctivitis), and Koplik spots (tiny white spots inside the cheek) — the pathognomonic sign of measles.
- Onset dates: When did the rash appear? Measles rash appears 3-4 days after fever starts.
- Class and age: Are all cases in one class? One grade? One dormitory?
- Vaccination status: Check immunisation cards for all students in affected classes. Calculate coverage: (Number vaccinated ÷ Total students) × 100.
- Contact history: Did any student recently travel to an area with a known measles outbreak?
- Actions:
- Isolate suspected cases: Keep them home for at least 4 days after rash onset.
- Report immediately: Measles is a notifiable disease in most countries. Notify the District Health Office within 24 hours.
- Support vaccination response: Organise a catch-up campaign for all unvaccinated children in the school and surrounding community.
- Protect close contacts: Infants under 9 months, pregnant women, and immunocompromised children should be kept away from the school.
💡 Key Principle: Susceptibility is not equal. Immunity strongly shapes who becomes ill. Two children sit next to each other in class. One is vaccinated, one is not. The measles virus does not "choose" — it simply cannot infect the immune child. Vaccination is the great equaliser.
🩺 The Situation: Three mothers develop wound infections after delivery. The ward recently lacked handwashing supplies. Different staff attended the deliveries.
Task: Identify the possible exposure, outcome, and links in the chain.
| Element | Description |
|---|---|
| Exposure | Poor hand hygiene by staff due to lack of soap and water. Contaminated instruments or environment may also be involved. |
| Outcome | Post-operative / post-partum wound infection (surgical site infection, SSI). |
| Agent | Bacteria — likely Staphylococcus aureus (including MRSA), Streptococcus, or gram-negative bacilli from the environment or staff hands. |
| Reservoir | Staff hands, contaminated surfaces, unclean instruments, or the mother's own skin flora (endogenous infection). |
| Portal of Exit | From staff hands or surfaces to the mother's wound during delivery or postnatal care. |
| Mode of Transmission | Direct contact (contaminated hands touching wound) and fomite (contaminated instruments, bed linens). |
| Portal of Entry | Broken skin at the episiotomy site, caesarean section wound, or perineal tear. |
| Susceptible Host | Post-partum mothers — especially those with anaemia, malnutrition, prolonged labour, or HIV (reduced immunity). |
- Restore supplies immediately: Handwashing soap, running water, alcohol-based hand rub, and sterile gloves must be available at every delivery station.
- Review infection prevention practices: Check whether staff are performing the "5 moments of hand hygiene" (before touching a patient, before aseptic procedure, after body fluid exposure, after touching a patient, after touching patient surroundings).
- Check records: Review delivery notes. Were aseptic techniques followed? Were instruments properly sterilised? Was the delivery environment clean?
- Report: Document the cluster as a healthcare-associated infection (HAI) and notify the infection control committee.
- Treat affected mothers: Wound cultures, appropriate antibiotics, and wound care.
⚡ Key Principle: Do not blame individuals first; study the system and fix modifiable risks. If three different staff attended the deliveries, the problem is likely the system (lack of supplies, poor protocols) rather than one careless nurse. Fix the system, and you protect all patients.
Control does not always require knowing everything immediately. Start with safe actions that reduce spread. Here is how to break each link:
| Link to Break | What to Do | Practical Examples |
|---|---|---|
| Break the Agent | Kill, weaken, or remove the infectious agent. | Correct diagnosis and treatment (antibiotics, antimalarials, antivirals). Sterilise equipment. Disinfect surfaces. Handle infectious materials safely (sharps containers, biohazard bags). |
| Break the Reservoir | Identify where the agent survives and remove or clean it. | Treat infected humans. Isolate infectious patients. Clean contaminated water (chlorination, boiling). Drain stagnant water. Remove animal reservoirs (dog vaccination for rabies, rat control). |
| Break Exit & Entry | Block the ways the agent leaves and enters the body. | Cover coughs and wounds (reduces exit). Use gloves, masks, and safe sharps practice (blocks entry). Promote safe delivery and wound care (prevents entry through broken skin). |
| Break Transmission | Interrupt the route between reservoir and host. | Hand hygiene breaks contact spread. Safe water breaks water-borne spread. Nets and vector control break mosquito spread. Ventilation and masks reduce respiratory spread. Condoms break sexual transmission. |
| Protect the Host | Strengthen the person so they resist infection. | Vaccination increases immunity. Nutrition support (iron, vitamin A, protein) strengthens natural defences. Prophylaxis (e.g., cotrimoxazole for HIV patients, IPTp for pregnant women) prevents infection. Health education helps people avoid exposure. |
📝 Exam Tip: When asked "How would you control this outbreak?" structure your answer by link in the chain. Say: "I would break the reservoir by... I would break transmission by... I would protect the host by..." This shows systematic thinking and earns full marks.
- Observation: Noticing patterns, clusters, and unusual increases.
- Safe practice: Hand hygiene, PPE, aseptic technique, safe injection practices.
- Reporting: Notifying supervisors, infection control nurses, and district health offices.
- Education: Teaching patients, families, and communities how to protect themselves.
🩺 The Situation: A clinic has more diarrhoea cases after a water pipe burst. A few children are severely dehydrated. The community still uses the damaged water source.
Task: What actions are needed immediately, and which link do they break?
| Immediate Action | Link Broken | Why It Matters |
|---|---|---|
| Treat dehydration and refer severe cases | Protects the host | Severe dehydration kills children fast. ORS, zinc, and IV fluids save lives. This is clinical care — but also public health, because treating cases reduces the reservoir (shorter shedding period). |
| Provide safe water or boil/chlorinate water | Breaks transmission | If people stop drinking contaminated water, new infections stop immediately. This is the fastest way to break a water-borne outbreak. |
| Investigate source and repair pipe | Controls reservoir | The broken pipe allowed sewage to enter the water supply. Fixing it removes the long-term reservoir. This prevents future outbreaks. |
| Educate on handwashing and safe storage | Breaks transmission + protects host | Even with safe water, dirty hands can contaminate it. Safe storage (covered containers) prevents recontamination at home. Education empowers the community. |
💡 Key Principle: Good control combines clinical care and public health prevention. You cannot choose between treating the sick child and fixing the pipe. You must do both — simultaneously. The nurse treats the patient; the public health nurse fixes the community.
Cover the answers and test yourself. If you can answer these clearly, you are ready for Day 3's exam!
- Name the six links in the chain of infection: Agent → Reservoir → Portal of Exit → Mode of Transmission → Portal of Entry → Susceptible Host.
Mnemonic: "All Rabbits Prefer Many Peas Soup" or "All Residents Please Move Past Security." - Give one example of a reservoir: A human with typhoid (human reservoir), a bat with Ebola (animal reservoir), or stagnant water with cholera bacteria (environmental reservoir).
Remember: A reservoir is where the agent normally lives and grows. - Give one example of a portal of entry: Mouth (ingesting contaminated water), nose (inhaling TB bacilli), broken skin (mosquito bite transmitting malaria), genital tract (sexual transmission of HIV).
The portal of entry is how the agent gets into the new host. - Explain how immunity changes disease spread: High immunity (through vaccination or prior infection) reduces the number of susceptible hosts, making it harder for the agent to spread. Low immunity allows rapid transmission. Herd immunity protects even unvaccinated individuals by reducing overall transmission.
Think of immunity as removing "fuel" from the fire of transmission. - What is the difference between droplet and airborne transmission? Droplet transmission involves larger particles that travel short distances (<1 metre) and are blocked by surgical masks. Airborne transmission involves tiny particles that remain suspended in air, travel long distances, and require N95 respirators and special ventilation. TB and measles are airborne; influenza is mainly droplet.
This is a favourite exam question. Memorise the examples and the PPE required. - Why is vector control important even if you treat all infected people? Treating infected people breaks the agent link but does not stop new mosquitoes from biting and transmitting. Vector control (nets, larviciding, drainage) breaks the transmission link and protects the entire community, including people who have not yet been infected.
In vector-borne diseases, you must attack both the human reservoir and the vector. - What is herd immunity, and why does it matter for measles? Herd immunity occurs when enough people are immune that the disease cannot spread easily. For measles, about 95% of the population must be vaccinated. If coverage drops, outbreaks occur — even among vaccinated people if immunity wanes. Herd immunity protects babies too young to be vaccinated and people who cannot receive vaccines for medical reasons.
Vaccination is not just personal protection — it is a community service. - In a maternity ward infection cluster, why should you "study the system, not blame the individual"? If multiple staff members are involved and multiple patients are affected, the problem is likely a system failure (lack of supplies, poor protocols, inadequate training) rather than one careless nurse. Blaming individuals creates fear and hides the real problem. Fixing the system (restoring soap, retraining staff, auditing practices) prevents future infections.
This is a core principle of patient safety and quality improvement. - What is the precautionary principle in outbreak control? The precautionary principle means taking protective action before all the evidence is in. If a water source is suspected of causing cholera, you do not wait for lab confirmation to provide safe water. You act on reasonable suspicion to prevent harm.
Public health prioritises prevention over perfect knowledge. - Give two nursing actions for each link in the chain of infection for malaria:
- Agent: Test and treat promptly with ACTs; ensure radical cure (complete treatment).
- Reservoir: Treat all confirmed cases; clear asymptomatic carriers in high-transmission areas (mass drug administration).
- Portal of Exit: Not applicable for malaria (agent is inside mosquito, not human excretions), but preventing human-mosquito contact reduces reservoir availability.
- Mode of Transmission: Distribute and promote insecticide-treated nets; drain stagnant water; use indoor residual spraying.
- Portal of Entry: Prevent mosquito bites (nets, repellents, screens, closing doors early).
- Susceptible Host: Vaccinate (RTS,S/AS01 malaria vaccine where available), provide IPTp for pregnant women, improve nutrition.
- World Health Organization (WHO) Guidelines on Core Components of Infection Prevention and Control Programmes.
- Centers for Disease Control and Prevention (CDC). Principles of Epidemiology in Public Health Practice.
- Gordis, L. (2013). Epidemiology (5th ed.). Saunders.
- Nelson, K. E., & Williams, C. M. (2014). Infectious Disease Epidemiology: Theory and Practice (3rd ed.). Jones & Bartlett Learning.
Quick Quiz
Disease Transmission and Control Quiz
Epidemiology and Biostatistics - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Disease Transmission and Control Quiz
Epidemiology and Biostatistics
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.