

Aggression is generally defined as any behavior directed toward another individual that is carried out with the proximate intent to cause harm. The intent is key here; accidental harm is not considered aggression.
Aggression: It is harsh physical or verbal action intended to harm or injure another person. OR Aggression is verbal expression of readiness to cause an attack with threats.
- Behavioral: It must be an observable action, not just a thought or feeling.
- Intent to Harm: The actor must intend to cause some form of harm (physical, psychological, social).
- Targeted: It is directed at another living being, not an inanimate object (unless the object is destroyed with the intent to harm someone through its loss).
Violence is a subset of aggression. It refers to aggression that has as its goal extreme physical harm, injury, or death.
Violence: is a threat with physical attack that results into harm. OR Violence is showing marked physical force causing harm being inflicted on another person or object.
- Extreme Form of Aggression: All violence is aggression, but not all aggression is violence.
- Physical Harm: Specifically involves behaviors intended to cause severe physical injury or death.
- Instrumental (or Proactive) Aggression: Aggression committed to achieve a desired goal or outcome, rather than to cause harm for its own sake. It is premeditated and goal-oriented.
- Motivation: Often driven by anticipated rewards or benefits (e.g., money, power, resources).
- Example: A robber assaulting a victim to get their money; a hitman committing murder for hire; a bully intimidating someone to get their lunch money.
- Hostile (or Reactive/Emotional) Aggression: Aggression stemming from feelings of anger, frustration, or pain, with the primary goal of inflicting harm on another. It is often impulsive and unplanned.
- Motivation: To hurt the other person, often in response to a perceived threat, insult, or provocation.
- Example: Lashing out in anger during an argument; a spontaneous fight after a perceived slight; road rage.
- Physical Aggression: Involves causing physical harm to another person or animal.
- Examples: Hitting, kicking, pushing, punching, using weapons. Violence is a severe form of physical aggression.
- Verbal Aggression: Involves causing psychological or emotional harm through words.
- Examples: Yelling, screaming, insulting, threatening, name-calling, spreading rumors, cyberbullying.
- Relational Aggression: Harming others by damaging their social relationships or social status.
- Examples: Spreading rumors, social exclusion, manipulation, betraying confidences, ostracizing. Often seen in peer groups, especially among adolescents.
- Direct Aggression: The aggressive act is aimed directly at the target.
- Examples: A punch to the face, a direct insult.
- Indirect Aggression: The aggressive act is not directly aimed at the target, but causes harm through an intermediary or by damaging the target's possessions or reputation.
- Examples: Spreading rumors behind someone's back, vandalizing someone's property, passive-aggressive behaviors.
Violence is a global public health problem. The WHO defines violence broadly, encompassing physical, sexual, psychological, and neglect, and classifies it by perpetrator (self-directed, interpersonal, collective).
- Leading Cause of Death: Violence (especially interpersonal and self-directed) contributes significantly to mortality and morbidity worldwide, particularly among young people.
- Economic Burden: The economic costs of violence are enormous, including healthcare expenses, lost productivity, legal costs, and long-term consequences for victims and society.
This section will now explicitly incorporate your specific "causes" into the broader categories.
- Genetics and Heritability: Inherited from the parents (genetic). This reinforces the idea of a genetic predisposition.
- Neurobiological Factors (Expanded):
- Pre or post ictal phase of epilepsy: This is a crucial physiological state that can directly cause aggression due to altered brain activity.
- Hormonal dysfunction: Violent and aggressive behaviour is associated with hormonal dysfunction for example Cushing’s disease (hyperthyroidism). This adds a specific medical condition.
- Mental Illnesses & Neurological Conditions :
- Mental illnesses: This section will now explicitly detail how certain symptoms directly cause aggression:
- Hallucinations: Patient experiencing hallucinations where a patient may hear voices telling him/her to fight or may see the health service provide as a lion and so she is fighting in self defence.
- Delusions: The patient may also be experiencing delusions for example a patient may be having persecutory delusions whereby she is suspecting her and planning to do evil to the patient so she gets violent in self-defense. This highlights the self-defense motivation arising from distorted reality.
- Delusions and hallucinations especially auditory or visual types.
- Mental illnesses: This section will now explicitly detail how certain symptoms directly cause aggression:
- Personality Traits: Impulsive behaviour might be the cause if there is history of such behaviour. This directly links impulsive personality traits to aggressive causation.
- Cognitive Distortions: This still applies, especially how delusions lead to aggressive interpretations.
- Learned Behaviors: Learnt behaviour from friends or parents. This strongly supports Social Learning Theory. Peer group influence for example living with people who have naturally aggressive behaviour (learnt behaviour). This further emphasizes the role of observational learning and social reinforcement.
- Frustration: Frustration i.e. if one does not know what to do. This directly links to the Frustration-Aggression Hypothesis.
- Family Environment: Learnt behaviour from friends or parents and Inherited from the parents (genetic) (though genetic is biological, its manifestation within a family context is social).
- Socioeconomic Disadvantage: Common in poor families due to lack essentials for life. This clearly ties economic hardship to aggression.
- Institutional/Environmental Factors (New Sub-category): This will be a significant addition, integrating your points about the hospital environment.
- Forced Admissions/Discharges/Procedures:
- Forced admission of a patient with mental illness.
- Forced discharges of patients who prefer to stay in hospital than going back to the community (institutional neurosis).
- Forced procedures such as Female Genital Mutilation. (While FGM is often cultural, the "forced" aspect makes it an immediate cause of aggression in the context of resisting the procedure).
- Ward Environment & Routine:
- Boredom and being idle on the ward.
- Monotonous routine activities on the ward.
- The ward environment may be boring or filthy.
- Lack of Support/Communication/Neglect:
- Lack of communication between patient and staff.
- Staff may not be therapeutic to the patient. Poor nurse-patient relationship or patient being neglected by the health service provider.
- Medication might have been forced so the patient looks at relatives as enemies.
- Lack of financial support to the patient to return to hospital for review as prescribed by the psychiatrist or lack of review due to negligence of relatives.
- Stigmatization: Stigmatization by community members or family members whereby the patient is called such names like, “wire”, “zolo” hence making the patient become violent. This highlights how social invalidation and dehumanization can provoke aggression.
- Provocation: Provocation: by fellow patients, Staff , friends or relatives. This is a direct trigger.
- Forced Admissions/Discharges/Procedures:
- Substance Use:
- Alcohol and drug misuse. This reinforces a significant environmental cause.
This section will now be much more robust, explicitly listing all the indicators you provided.
- Restlessness: Restlessness moving up and down unable to sit still.
- Tense Body Language: Tense facial expression and body language.
- Verbal Escalation:
- Loud voice.
- Abusive language.
- Shouting.
- Use of obscenities.
- Argumentative.
- Scolding or annoying others.
- Threats: Verbal or physical threats. Threats of homicide or suicide.
- Object Use: Tendencies to move with harmful objects.
- Temper Tantrums: Temper tantrums (sudden outbursts and falling off).
- Negativism: Negativism - Doing the opposite of what is expected.
- Quietness/Withdrawal (Paradoxical Indicator):
- Isolated or withdrawn.
- Quietness - Not being able to say anything due to too much anger. This is a critical point, as quietness can sometimes precede an outburst, indicating extreme emotional buildup.
- Angry Mood: Angry mood often inappropriate to the situation.
- Disturbed Thought Process: Disturbed thought process. (Implies irrationality, difficulty processing information calmly).
- Suspiciousness: Suspiciousness. (Can lead to defensive aggression).
- Panic Attacks: Panic attacks. (High anxiety and fear can lead to 'fight or flight' response).
- Crying (Paradoxical Indicator): Crying without any clear reason. (Can indicate extreme emotional distress and overwhelm, which can precede aggression in some individuals).
- Disturbed Sleep: Disturbed sleep. (Often a sign of underlying distress, agitation, or mental health exacerbation).
The goal is to identify individuals at higher risk of future violent acts to implement appropriate interventions and ensure public safety.
- Low Base Rate Event: Violent behavior, especially severe violence, is a relatively rare event. Predicting low base rate events is inherently difficult, as even highly accurate predictors will result in many false positives (predicting violence that doesn't occur).
- Dynamic Nature of Risk: Risk factors are not static. An individual's risk for violence can change rapidly based on environmental stressors, treatment adherence, substance use, and mental state.
- Ethical Concerns: The implications of prediction are significant. False positives can lead to unnecessary restrictions on liberty, stigmatization, and misallocation of resources. False negatives can result in harm to others.
- Context Dependency: Violence is highly context-dependent. A person may be at risk in one situation but not another.
- Probabilistic, Not Deterministic: Predictions are always probabilistic (likelihoods), never deterministic (certainties).
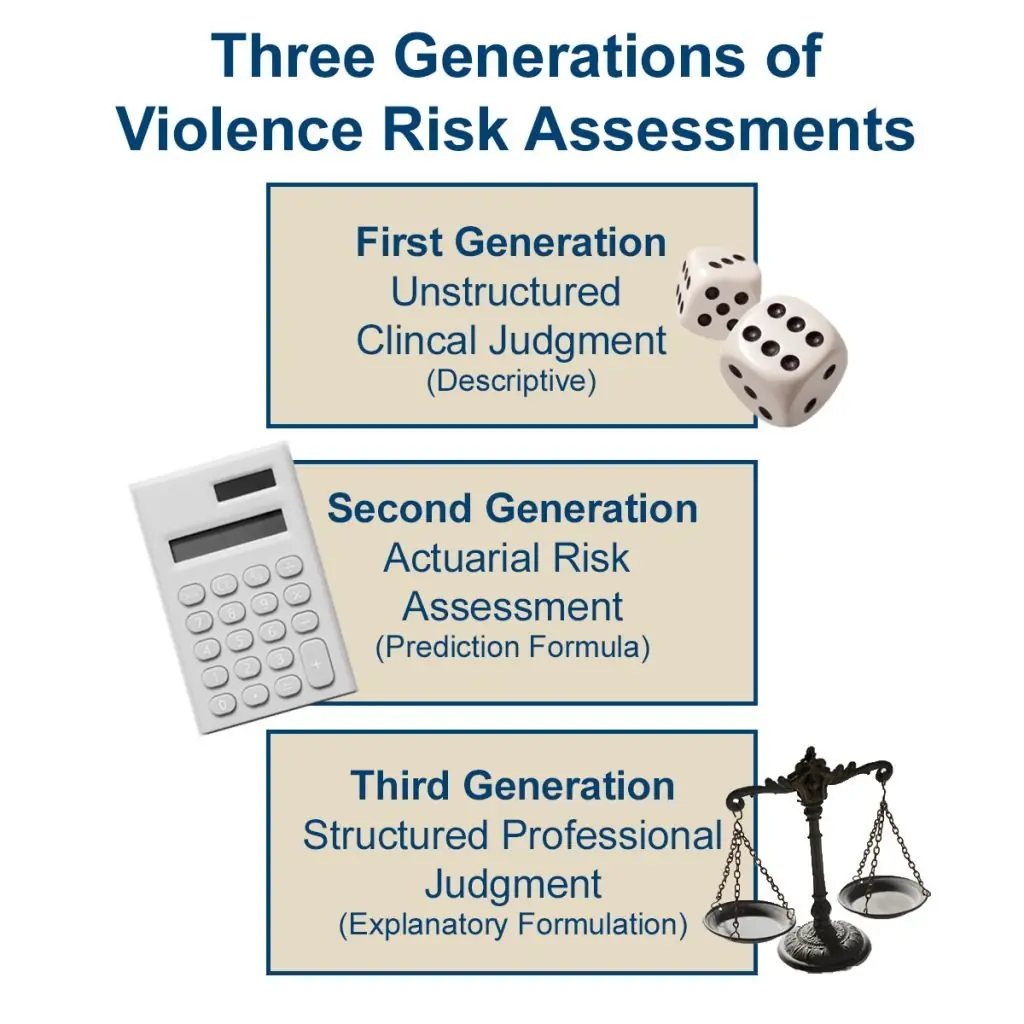
There are generally three generations or approaches to assessing the risk of violence:
- First Generation: Unstructured Clinical Judgment (UCJ):
- Method: Relies on the clinician's training, experience, intuition, and subjective assessment of various factors without standardized tools.
- Pros: Flexible, allows for consideration of unique individual factors.
- Cons: Highly subjective, low reliability (different clinicians often reach different conclusions), and generally poor predictive validity. Often prone to biases (e.g., overestimating risk).
- Status: While still part of clinical practice, it's generally considered insufficient as a standalone method for formal risk assessment.
- Second Generation: Actuarial Risk Assessment:
- Method: Uses empirically derived statistical formulas or algorithms based on specific, static risk factors (factors that don't change over time, like past criminal history, age of first offense). These factors are weighted and combined to produce a numerical probability or risk category.
- Examples: Violence Risk Appraisal Guide (VRAG), Static-99 (for sexual violence).
- Pros: Objective, quantifiable, high inter-rater reliability, and generally better predictive validity than UCJ for identifying groups at higher risk.
- Cons: Focuses almost exclusively on static (historical) factors, lacks consideration of dynamic (changeable) factors, provides a group probability rather than an individual prediction, and offers no guidance for intervention. Risk factors may be culturally biased.
- Status: Useful for large-scale screening and research, but limited in clinical utility for individual case management.
- Third Generation: Structured Professional Judgment (SPJ):
- Method: Combines the strengths of both clinical judgment and actuarial methods. Clinicians use a standardized set of empirically identified risk and protective factors (both static and dynamic) to guide their assessment. They then integrate this information with their clinical expertise to make a judgment about risk and provide recommendations for management.
- Examples:
- HCR-20 V3 (Historical, Clinical, Risk Management-20, Version 3): A widely used tool that assesses 20 risk factors across historical (past behavior), clinical (current mental state, symptoms), and risk management (future plans, supports) domains.
- Forensic Version of the Psychopathy Checklist-Revised (PCL-R): While not a direct violence predictor, it assesses psychopathic traits strongly correlated with persistent antisocial and aggressive behavior.
- Short-Term Assessment of Risk and Treatability (START): Focuses on both strengths and weaknesses (risk and protective factors) to provide a dynamic risk assessment.
- Pros: Improved predictive validity over UCJ, considers dynamic and protective factors (which are crucial for intervention planning), good inter-rater reliability, and provides actionable recommendations.
- Cons: Requires extensive training for clinicians, still relies on clinical judgment at the final stage, and can be time-consuming.
- Status: Considered the current best practice for violence risk assessment in many clinical and forensic settings.
- Historical (Static) Factors:
- Prior violence/criminal history (strongest predictor)
- Age at first violent offense
- Childhood conduct problems/antisocial behavior
- History of substance abuse
- Psychopathy (as measured by PCL-R)
- History of intimate partner violence
- Clinical (Dynamic) Factors:
- Current psychotic symptoms (especially command hallucinations or paranoid delusions)
- Impulsivity/poor impulse control
- Lack of insight into mental health issues
- Angry affect/hostility
- Treatment non-compliance
- Presence of acute stressors (e.g., job loss, relationship breakup)
- Lack of empathy/remorse
- Risk Management (Contextual/Future) Factors:
- Lack of social support
- Poor response to supervision/treatment
- Presence of destabilizers (e.g., access to weapons, negative peers)
- Absence of a viable release plan
- Lack of constructive leisure/employment activities
- Negative attitudes towards authority
It's equally important to assess factors that reduce the likelihood of violence. These are crucial for building resilience and informing treatment.
- Strong social support network
- Positive coping skills
- Stable and positive relationships
- Insight into one's problems
- Adherence to treatment
- Meaningful employment or education
- Prosocial attitudes
- Good problem-solving abilities
This is a psychiatric emergency. The management of aggression and violence, particularly in a psychiatric emergency, is paramount for the safety of the individual, other patients, and staff.
- To safeguard the public and the patient: This is the primary concern, ensuring physical safety for everyone involved.
- To treat and monitor the patient: Address the underlying causes and symptoms, and observe their response to interventions.
This phase focuses on de-escalation and ensuring safety.
- Preparation and Environment:
- Admission on Acute Ward: Patient should be admitted on acute ward and ensuring there are no harmful objects near the vicinity.
- Environmental Safety: Ensure that there is no weapon or dangerous tool available before approaching the patient. Remove any dangerous objects such as knives by requesting the patient to place them on the table or floor.
- Team Readiness: Ensure that there is enough man power to help you in case the patient gets more violent. Ensure sufficient staff are available.
- Removing Other Patients: Remove all other patients from the immediate environment.
- Initial Approach and De-escalation (Verbal & Non-Verbal):
- Maintain Calmness: Remain calm when dealing with this patient.
- Non-Threatening Stance: Move towards the patient with open hands to indicate no signs of harm. Approach the client from in front with open hands.
- Respectful Communication:
- Welcome the patient on the ward and address her by her name. Call the patient by names when approaching him or her.
- Talk to the patient and hear her response.
- Let patient express his feelings.
- Be firm and kind. Show the aggressive patients that you are in control of the situation.
- Transparency: In case the patient is hospitalized do not take her by surprise, explain all the procedures you are going to do assure the individual of his or her security.
- Empathy and Understanding: As a health worker should try to understand why he patient is aggressive before resorting to restraining methods. Help the patient to establish the true cause of anger.
- Ignoring Minor Provocations: If possible ignore initial derogatory remarks by the patient.
- Addressing Immediate Causes: Assess for possible causes of violence and aggression. If any try to eliminate the cause. (e.g., if boredom, offer activity; if uncomfortable, adjust environment).
- Physical Restraint (Last Resort):
- Justification: If not calmed down. When de-escalation fails and there's imminent danger.
- Safety First: Make sure that in the process of restraining nobody is hurt. Also minimize damage to property. Ensure that patient and staff are not injured during the restraint. Do not sit on the patient. Ensure that patients are not involved in the restraint.
- Technique: The patient should be approached convincingly but if he/she is still resistant, should be put on the bed swiftly or on the floor where he must readily be immobilized. Firmly hold the joints and limbs in firm position so as to avoid fractures and dislocation or hurting/injuries.
- Pre-existing Restraints: If the patient is chained, remove the chains and observe patient’s response.
- Distraction: Distract the patient’s attention as the rest of the manpower is getting close to the patient to restrain her.
- Chemotherapy (Pharmacological Intervention):
- Administration: Administer sedatives or tranquilizers if available in injection form. i.e. diazepam 10mg to 20mg t.d.s. The drugs include: Tranquillizers for example chlorpromazine, haloperidol. Sedatives are also important for example diazepam intramuscularly.
- Monitoring: Observe if the patient is still aggressive or violent. If yes repeat the sedation.
- Seclusion (Last Resort, Post-Restraint/Sedation):
- Placement: If still the same, put him/her in the side room (seclusion room). Do not lift the patient when taking him to the side room. Let the patient walk to the seclusion room.
- Documentation and Duration: Indicate the duration of the seclusion. Seclude the patient for specific period and indicate the reasons and goals of managing him in the side room.
- Continuous Observation: Observe if still aggressive or violent. Continue observing if he has calmed down. If so remove him but if not continue to seclude with treatment.
Once the immediate crisis has passed, the focus shifts to assessment, treatment, and prevention of recurrence.
- Comprehensive Assessment:
- Common Observations: Vitals, specific and general.
- Physical Health: Any physical illness.
- Mental Status: Patients mental status.
- Risk Factors: Risk of violence and aggression or indicators.
- Causative Factors: Assess for possible causes of violence and aggression. If any try to eliminate the cause.
- Therapeutic Relationship & Communication:
- Establish a positive nurse-patient relationship.
- Set or establish contract with the patient that he will not become violent.
- Continuous observation of client for escalation of anger.
- Treatment and Skill Building:
- Medication Management: Administer prescribed medications for underlying conditions.
- Emotional Regulation: Encourage the client to keep records of angry feelings that triggered him to become violent and how they were handled.
- Coping Strategies: Patient should be told to control emotions and be taught the skill of stress management.
- Discharge Planning and Community Support:
- Patient Education: Gradually tell the patient to avoid aggression and violence and avoid provoking situations. The nurse should talk to the patient to promise that he will not resort to violence if released back to his freedom.
- Family Involvement: Encourage family members to support the patient. Relatives should be educated about the signs of aggression and violence so that early intervention can be made.
- Addressing Stigma: Community should be taught about the dangers of stigmatisation.
- Follow-up Care: Advise family members to always refer patient when he becomes violent or aggressive. Lack of financial support to the patient to return to hospital for review as prescribed by the psychiatrist or lack of review due to negligence of relatives. (This implicitly highlights the need to address financial barriers to follow-up).
- Team Discussion: The clinical team should discuss the future of the patient. Make plans to release the patient.
- Comprehensive Recording: Document your care. This is crucial for legal, ethical, and clinical continuity of care.

Scenario: You are the nurse on duty on an acute psychiatric ward. You notice a male patient, Mr. X, who has been admitted for an acute psychotic episode, pacing rapidly, clenching his fists, and muttering loudly, directing angry comments towards another patient. He refuses to sit down when approached by a junior staff member. What are your immediate actions and subsequent management plan?
- Ensure Safety of All:
- "My immediate and paramount priority is the safety of all patients, staff, and Mr. X himself. I would ensure that any other patients are safely removed from the immediate vicinity, preferably to a quiet common area, to prevent them from becoming targets or escalating the situation."
- "I would quickly scan the environment for any potential weapons or harmful objects (e.g., chairs, sharp items) and remove them if safely possible, or note their presence for the team."
- Call for Assistance:
- "Concurrently, I would immediately call for additional trained staff (e.g., rapid response team, security if available, or designated 'show of force' staff) as per ward protocol. This ensures adequate manpower for safe de-escalation or, if necessary, physical intervention."
- Environmental Scan: (Already covered in safety, but re-emphasize as part of assessment).
- Patient Observation:
- "While calling for help, I would continuously observe Mr. X's behavior, body language, and verbalizations to gauge the level of threat and identify any potential triggers or immediate indicators of escalating aggression (e.g., specific threats, picking up objects, increased agitation, disturbed thought process)."
- "I would also consider if there are any immediate physical causes that could be contributing, such as pain, discomfort, or medication side effects."
- Identify Potential Triggers/Causes:
- "I would quickly consider recent events, e.g., medication changes, visitors, interaction with other patients, or if he's showing signs of delusions/hallucinations (e.g., 'muttering loudly, directing angry comments'). Understanding the 'why' helps in de-escalation."
- Maintain Calm & Non-Threatening Stance:
- "I would approach Mr. X calmly and confidently, maintaining a safe distance (e.g., 2-3 arm lengths) and ensuring I am not blocking his escape route. My body language would be open, with hands visible, indicating no threat."
- "I would avoid direct eye contact initially, or use intermittent eye contact, as prolonged direct eye contact can be perceived as confrontational."
- Verbal De-escalation (Therapeutic Communication):
- "I would address Mr. X by his preferred name, in a low, calm, and clear tone of voice. I would avoid shouting or speaking too quickly."
- "I would acknowledge his distress and feelings: 'Mr. X, I can see you're very upset/angry right now. Can you tell me what's going on?' or 'It looks like something is bothering you, Mr. X.'"
- "I would convey empathy and a willingness to listen, allowing him to express his feelings: 'Please tell me what's making you so angry.' 'I'm here to help.'"
- "I would be firm but kind in setting limits if needed, e.g., 'I want to help you, Mr. X, but I need you to lower your voice/stop directing comments at others.'"
- "I would avoid challenging his delusions or arguing, instead focusing on his feelings and offering to help with his distress."
- "I would try to offer choices and empower him if possible, e.g., 'Would you like to come to the quiet room with me, or would you prefer to sit here for a moment?'"
- Physical Intervention (Restraint - as a LAST resort):
- "If verbal de-escalation proves ineffective and Mr. X's aggression continues to escalate to the point of posing an immediate physical danger to himself or others (e.g., attempting to strike, picking up a weapon), I would initiate physical restraint with the assistance of the previously called-for staff."
- "This would be performed swiftly, safely, and collaboratively by the trained team, ensuring all limbs and joints are held firmly to prevent injury to Mr. X or staff. I would ensure we do not sit on him and that no other patients are involved."
- "Documentation of the decision, method, and duration of restraint would be immediate and thorough."
- Pharmacological Intervention (Chemotherapy):
- "Concurrently or immediately following safe restraint, I would administer prescribed 'STAT' (as needed) or emergency calming medication (e.g., an intramuscular benzodiazepine like Diazepam or an antipsychotic like Haloperidol, as per doctor's order/ward protocol), aiming to rapidly reduce his agitation and distress."
- "I would explain to Mr. X what medication I'm giving and why, if he is able to comprehend."
- Seclusion (as a LAST resort after restraint/medication):
- "If restraint and medication are still insufficient to de-escalate the situation and safety cannot otherwise be maintained, I would initiate seclusion. Mr. X would be gently guided, not lifted, to a designated seclusion room."
- "The seclusion would be for the shortest possible duration, with continuous observation, clear documentation of the reason, goals, and regular review."
- Monitoring:
- "After restraint/seclusion and medication, I would closely monitor Mr. X's vital signs, mental status, level of sedation, and any potential injuries. Regular observations would be continued until he is stable."
- Therapeutic Re-engagement:
- "Once Mr. X is calm, I would re-engage in therapeutic communication, discussing the incident without judgment. I would help him explore triggers, feelings, and alternative coping strategies. I would aim to re-establish a positive nurse-patient relationship."
- "I would explain the reasons for the interventions (e.g., 'We needed to keep everyone safe, including you')."
- Debriefing:
- "I would participate in a debriefing with the staff involved to discuss what happened, what worked well, what could be improved, and to offer support to staff."
- "A patient debrief would also occur when appropriate, to allow Mr. X to express his feelings about the incident."
- Documentation:
- "Thorough and accurate documentation of the entire incident, including observations, interventions (de-escalation, restraint, medication, seclusion), Mr. X's response, injuries (if any), and post-incident care, is critical."
- Care Plan Review:
- "I would contribute to a review of Mr. X's care plan with the multidisciplinary team, identifying new triggers, refining interventions, and incorporating new coping strategies to prevent future aggressive episodes."
- Safety First: Always prioritize the safety of everyone.
- De-escalation First: Always attempt verbal de-escalation before physical methods.
- Least Restrictive Means: Use the least restrictive intervention necessary.
- Team Approach: Emphasize working with trained staff.
- Respect & Dignity: Maintain the patient's dignity throughout the process.
- Documentation: Crucial for legal, ethical, and clinical reasons.
- Therapeutic Relationship: The ultimate goal is to restore the nurse-patient relationship and promote healing.
It’s great
Great work
Thanks,notes well explained
Great work
Notes are easier to understand
Good work and understandable