
Attention-Deficit/Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterized by a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development.
- Inattention means a person wanders off task, lacks persistence, has difficulty sustaining focus and is disorganized and these problems are not due to defiance or lack of comprehension.
- Hyperactivity means a person seems to move about constantly, including in situations in which it is not appropriate or excessively fidgets, taps, or talks.
- Impulsivity means a person makes hasty actions that occur in the moment without first thinking about them and that may have high potential for harm or a desire for immediate rewards or inability to delay gratification. An impulsive person may be socially intrusive and excessively interrupt others to make important decisions without considering the long-term consequences.
It is one of the most common neurodevelopmental disorders of childhood and often persists into adulthood.
- Neurodevelopmental: This classification emphasizes that ADHD is a disorder of brain development and function, rather than solely a behavioral or psychological issue. It involves differences in brain structure, function, and connectivity, particularly in areas related to executive functions such as attention, impulse control, and regulation of activity level.
- Persistent Pattern: The symptoms are not transient; they are ongoing, lasting for at least six months, and are inconsistent with the individual's developmental level.
- Interferes with Functioning or Development: The symptoms must cause significant impairment in at least two settings (e.g., home, school, work, social situations). This impairment can affect academic performance, occupational success, social relationships, and overall quality of life.
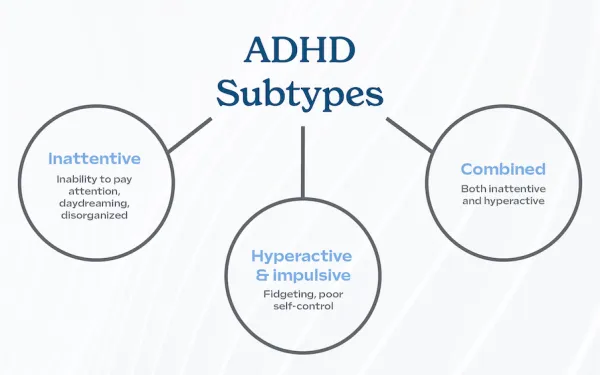
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), specifies three primary presentations, or subtypes, of ADHD based on the predominant symptoms experienced by the individual over the past six months:
- Predominantly Inattentive Presentation:
- Individuals primarily exhibit symptoms of inattention, with fewer hyperactive-impulsive symptoms.
- Symptoms often include: Difficulty sustaining attention in tasks or play activities, being easily distracted, not seeming to listen when spoken to directly, often losing things necessary for tasks or activities, difficulty organizing tasks and activities, avoiding or disliking tasks that require sustained mental effort, and being forgetful in daily activities.
- Predominantly Hyperactive-Impulsive Presentation:
- Individuals primarily exhibit symptoms of hyperactivity and impulsivity, with fewer inattentive symptoms.
- Symptoms often include: Fidgeting or squirming, often leaving seat in situations when remaining seated is expected, running about or climbing in situations where it is inappropriate, difficulty playing or engaging in leisure activities quietly, often "on the go" or acting as if "driven by a motor," talking excessively, blurting out answers before questions have been completed, difficulty waiting their turn, and often interrupting or intruding on others.
- Combined Presentation:
- Individuals meet the criteria for both inattention and hyperactivity-impulsivity.
- This is the most common presentation of ADHD.
The etiology of Attention-Deficit/Hyperactivity Disorder (ADHD) is complex involving a significant interplay of genetic, neurobiological, and environmental factors. It is not caused by poor parenting, too much sugar, or excessive screen time, although these factors can exacerbate symptoms or influence management.
- High Heritability: Genetic factors are considered the strongest contributors to ADHD. Studies, particularly twin and family studies, show that ADHD is highly heritable, with heritability estimates ranging from 70% to 80%. This means that if a parent has ADHD, their child has a significantly higher chance of also having it.
- Polygenic Disorder: ADHD is not typically linked to a single gene but rather to the combined effect of multiple genes, each contributing a small amount to the overall risk. Many of these genes are involved in the regulation of neurotransmitters (especially dopamine and norepinephrine) and brain development.
- Neurotransmitter System Genes: Research often points to genes involved in dopamine regulation (e.g., dopamine receptor genes DRD4 and DRD5, and dopamine transporter gene DAT1) and norepinephrine regulation as key players, affecting brain circuits related to reward, motivation, attention, and executive function.
- Prefrontal Cortex: Involved in attention, decision-making, impulse control, and working memory. Studies often show reduced activity or smaller volume in certain areas of the prefrontal cortex in individuals with ADHD.
- Basal Ganglia: Important for regulating movement, reward, and motivation.
- Cerebellum: Involved in motor control, timing, and cognitive functions.
- Default Mode Network (DMN): Differences in the connectivity and activity of the DMN, which is active when the brain is at rest, have been observed.
- Dopamine: Reward, motivation, pleasure, attention, and executive control.
- Norepinephrine: Alertness, arousal, attention, and decision-making.
- Imbalances or inefficiencies in these systems are thought to contribute to the core symptoms of ADHD.
While not primary causes, certain environmental factors can increase the risk of developing ADHD or exacerbate its symptoms.
- Maternal Smoking, Alcohol, or Drug Use during Pregnancy: Exposure to toxins during crucial periods of fetal brain development can increase the risk.
- Maternal Stress/Anxiety during Pregnancy: Emerging research suggests a potential link, though more studies are needed.
- Premature Birth / Low Birth Weight: Babies born significantly premature or with very low birth weight have a higher risk of developing ADHD.
- Brain Injury: Traumatic brain injury in early development can sometimes lead to ADHD-like symptoms.
- Exposure to Environmental Toxins: Lead exposure in early childhood has been linked to an increased risk of ADHD symptoms.
- Severe Early Deprivation: Extreme neglect or institutionalization in early childhood, although rare, can lead to attention and hyperactivity problems that mimic ADHD.
- Note: While family stress, chaotic home environments, or poor parenting do not cause ADHD, they can significantly worsen symptoms and make management more challenging.
Attention-Deficit/Hyperactivity Disorder (ADHD) is characterized by a persistent pattern of inattention and/or hyperactivity-impulsivity. core manifestations significantly interfere with an individual's functioning in multiple areas of life.
The core symptoms of ADHD are categorized into two main domains: Inattention and Hyperactivity-Impulsivity. To meet diagnostic criteria, an individual must display a certain number of symptoms in one or both domains, with onset before age 12, present in two or more settings, and causing significant impairment.
(At least six symptoms for children up to age 16, or five for adolescents 17 and older and adults; symptoms must have been present for at least 6 months)
- Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or during other activities (e.g., overlooks or misses details, work is inaccurate).
- Often has difficulty sustaining attention in tasks or play activities (e.g., has difficulty remaining focused during lectures, conversations, or lengthy reading).
- Often does not seem to listen when spoken to directly (e.g., mind seems elsewhere, even in the absence of any obvious distraction).
- Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e.g., starts tasks but quickly loses focus and is easily sidetracked).
- Often has difficulty organizing tasks and activities (e.g., difficulty managing sequential tasks; difficulty keeping materials and belongings in order; messy, disorganized work; has poor time management; fails to meet deadlines).
- Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (e.g., schoolwork or homework; for older adolescents and adults, preparing reports, completing forms, reviewing lengthy papers).
- Often loses things necessary for tasks or activities (e.g., school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones).
- Is often easily distracted by extraneous stimuli (for older adolescents and adults, may include unrelated thoughts).
- Is often forgetful in daily activities (e.g., doing chores, running errands; for older adolescents and adults, returning calls, paying bills, keeping appointments).
(At least six symptoms for children up to age 16, or five for adolescents 17 and older and adults; symptoms must have been present for at least 6 months)
- Often fidgets with or taps hands or feet or squirms in seat.
- Often leaves seat in situations when remaining seated is expected (e.g., leaves his or her place in the classroom, in the office or other workplace, or in other situations that require remaining in place).
- Often runs about or climbs in situations where it is inappropriate (Note: In adolescents or adults, may be limited to feeling restless).
- Often unable to play or engage in leisure activities quietly.
- Is often "on the go" acting as if "driven by a motor" (e.g., is uncomfortable being still for extended time, as in restaurants, meetings; may be experienced by others as restless or difficult to keep up with).
- Often talks excessively.
- Often blurts out an answer before a question has been completed (e.g., completes people's sentences; cannot wait for turn in conversation).
- Often has difficulty waiting his or her turn (e.g., while waiting in line).
- Often interrupts or intrudes on others (e.g., butts into conversations, games, or activities; may start using other people's things without asking or receiving permission; for adolescents and adults, may intrude into or take over what others are doing).
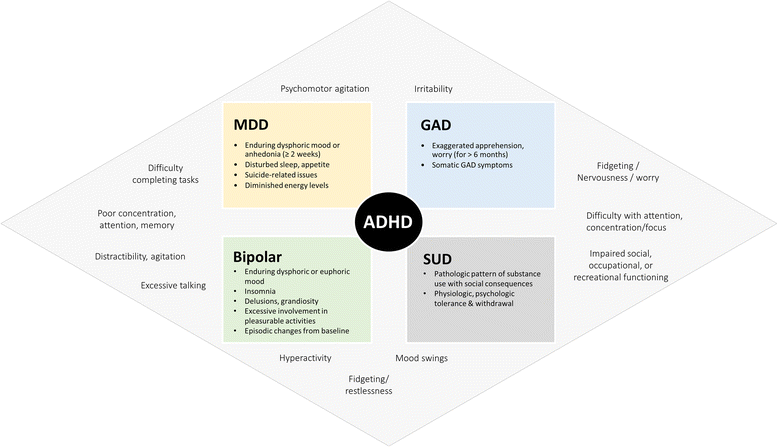
Comorbidity is the rule rather than the exception in ADHD, with many individuals having at least one other mental health or learning disorder. These co-occurring conditions can significantly impact the presentation of ADHD symptoms, complicate diagnosis, and require integrated treatment approaches.
- Oppositional Defiant Disorder (ODD) and Conduct Disorder (CD): ODD involves a pattern of angry/irritable mood, argumentative/defiant behavior, or vindictiveness. CD involves a more severe pattern of antisocial behavior, aggression, destruction of property, deceitfulness, or serious rule violations.
- Anxiety Disorders: Generalized anxiety disorder, social anxiety, separation anxiety, panic disorder.: Can lead to internalizing behaviors, perfectionism, or avoidance, and can make ADHD symptoms (e.g., inattention due to worry) worse.
- Depressive Disorders (Major Depressive Disorder, Persistent Depressive Disorder): Can be difficult to differentiate from ADHD symptoms (e.g., fatigue, lack of motivation). ADHD can increase the risk of depression due to chronic challenges and low self-esteem.
- Specific Learning Disorders (SLDs): Difficulties in learning and using academic skills (e.g., reading/dyslexia, written expression/dysgraphia, mathematics/dyscalculia).
- Autism Spectrum Disorder (ASD): Both disorders involve challenges with attention, social interaction, and sensory processing. ADHD symptoms can be present in individuals with ASD, and vice versa.
- Tourette's Syndrome and Chronic Tic Disorders: Involuntary, repetitive movements or vocalizations (tics).
- Substance Use Disorders (SUDs): Individuals with untreated ADHD, especially the combined type, have a significantly higher risk of developing SUDs, particularly nicotine and alcohol.
- Sleep Disorders: Insomnia, restless legs syndrome, sleep apnea.
The process is conducted by a trained healthcare professional, such as a pediatrician, child psychiatrist, psychologist, or neurologist, and often involves a multidisciplinary team approach.
- No Single Test: There is no blood test, brain scan, or single psychological test that can definitively diagnose ADHD.
- Clinical Evaluation: Diagnosis is based on a careful clinical assessment of symptoms and their impact on functioning, using established diagnostic criteria (DSM-5).
- Multisource Information: Information is gathered from various settings and multiple informants (e.g., parents, teachers, caregivers, the individual themselves).
- Developmental area: Symptoms must be inconsistent with the individual's developmental level.
- Pervasiveness and Impairment: Symptoms must be present in two or more settings (e.g., home, school, work, social situations) and cause significant impairment in major life activities.
- Exclusion of Other Conditions: Other medical or psychological conditions that could explain the symptoms must be considered and ruled out.
- Initial Clinical Interview and History Taking:
- Patient Interview: For adolescents and adults, a detailed interview to understand their current symptoms, their impact, and their history.
- Parent/Caregiver Interview: For children and younger adolescents, interviews with parents or primary caregivers are essential to gather information about:
- Developmental History: Milestones, early behaviors, temperament.
- Symptom Onset and Duration: When symptoms first appeared, how long they have been present, and their course over time (DSM-5 requires symptoms to be present before age 12, though this can be recalled retrospectively).
- Symptom Severity and Pervasiveness: How severe the symptoms are, and in which settings they occur (e.g., home, school, daycare, social gatherings).
- Impact on Functioning: How symptoms affect academic performance, social relationships, family life, self-care, and daily activities.
- Family Medical and Psychiatric History: To identify any genetic predispositions or co-occurring family conditions.
- Past Medical History: Including pregnancy and birth history, illnesses, injuries, and medication use.
- Information from Multiple Informants:
- Teacher Reports: For school-aged children, information from teachers is critical as they observe behavior in a structured, demanding environment. Teachers can provide insights into inattention, hyperactivity, impulsivity, academic performance, and social interactions in the classroom.
- Other Caregivers: Reports from daycare providers, coaches, or tutors can also be valuable.
- Standardized Rating Scales (Behavior Rating Scales):
- Purpose: These are questionnaires completed by parents, teachers, and often the individual themselves (for older children/adults) to systematically assess ADHD symptoms and related behaviors. They compare the individual's behavior to age and gender norms.
- Common Scales:
- Conners 3rd Edition (Conners 3): Widely used for children and adolescents, with parent, teacher, and self-report forms.
- ADHD Rating Scale-5 (ADHD-RS-5): Directly maps to DSM-5 criteria.
- Vanderbilt ADHD Diagnostic Teacher and Parent Rating Scales: Popular in educational and clinical settings.
- Adult ADHD Self-Report Scale (ASRS): For adults.
- Interpretation: Scores are typically compared to normative data to indicate the likelihood and severity of ADHD symptoms.
- Observation:
- Clinical Observation: The clinician observes the individual's behavior during the evaluation, noting attention span, activity level, impulsivity, and social interaction.
- Naturalistic Observation (less common): Sometimes, a professional may observe the child in a classroom or home setting, though this is often impractical.
- Psychological and Educational Testing (Optional but often recommended):
- Neuropsychological Testing: Can assess specific cognitive functions often impacted by ADHD, such as executive functions (working memory, inhibitory control, planning), attention, and processing speed. This helps identify specific areas of strength and weakness and rule out other conditions.
- Achievement Testing: To screen for specific learning disorders, which frequently co-occur with ADHD.
- Intellectual Assessment (IQ Testing): To ensure symptoms are not better explained by intellectual disability.
- Six (or more) symptoms of inattention and/or six (or more) symptoms of hyperactivity-impulsivity for at least 6 months.
- Several inattentive or hyperactive-impulsive symptoms were present before age 12 years.
- Several symptoms are present in two or more settings.
- There is clear evidence that the symptoms interfere with, or reduce the quality of, social, academic, or occupational functioning.
- The symptoms do not occur exclusively during the course of schizophrenia or another psychotic disorder and are not better explained by another mental disorder.
Evidence consistently supports a combination of medication and behavior therapy as the most effective approach, especially for children.
Medication do not offer permanent cure for ADH but may help someone with the condition to concentrate better, be less impulsive, fell calmer and learn to practice new skills. Drugs licensed for treatment of ADHD include;
- Methylphenidate one tablet once a day
- Lisdexamfetamine once capsule once a day
- Dexamfetamine one tablet once or twice a day
- Atomoxetine one capsule once or twice a day
- Guanfacine one tablet once a day
- tricyclic antidepressants
- Antipsychotics
- serotonin specific reuptake inhibitors
Medications do not cure ADHD but can significantly reduce core symptoms, allowing individuals to benefit more from behavioral and educational interventions.
- Stimulants (First-line for most ages):
- Mechanism of Action: Increase the availability of dopamine and norepinephrine in the brain, primarily by blocking their reuptake and, to a lesser extent, by promoting their release. This enhances signaling in brain regions responsible for attention, focus, and impulse control (e.g., prefrontal cortex).
- Examples:
- Methylphenidate-based: Ritalin, Concerta, Daytrana (patch), Focalin, Quillivant XR, Adhansia XR.
- Amphetamine-based: Adderall, Vyvanse, Dexedrine, Mydayis.
- Forms: Available in short-acting (taken 2-3 times/day) and long-acting (once daily) formulations. Long-acting forms are often preferred for convenience and smoother symptom control.
- Efficacy: Highly effective in reducing core symptoms (inattention, hyperactivity, impulsivity) in approximately 70-80% of individuals.
- Common Side Effects: Decreased appetite/weight loss, sleep disturbances (insomnia), headache, stomachache, irritability, increased heart rate and blood pressure (usually minor).
- Nursing Considerations: Monitor growth, weight, blood pressure, and heart rate. Educate on administration (e.g., timing to avoid sleep issues), potential side effects, and importance of adherence. Assess for effectiveness and adjust dose as prescribed.
- Non-Stimulants (Alternatives or adjuncts):
- Mechanism of Action: Work differently than stimulants, often by selectively targeting norepinephrine or other neurotransmitter systems.
- Examples:
- Atomoxetine (Strattera): Selective norepinephrine reuptake inhibitor (SNRI). Takes several weeks for full effect.
- Guanfacine (Intuniv) and Clonidine (Kapvay): Alpha-2 adrenergic agonists. Can be particularly helpful for hyperactivity, impulsivity, tics, and sleep disturbances.
- Bupropion (Wellbutrin): A dopamine and norepinephrine reuptake inhibitor, sometimes used off-label, especially with comorbid depression.
- Efficacy: Less rapid and generally less potent in symptom reduction compared to stimulants, but effective for many, especially those who don't respond to or tolerate stimulants.
- Common Side Effects:
- Atomoxetine: Nausea, stomach upset, fatigue, dry mouth, suicidal ideation (rare).
- Guanfacine/Clonidine: Drowsiness, fatigue, low blood pressure, dizziness.
- Nursing Considerations: Educate on delayed onset of action for atomoxetine. Monitor blood pressure and heart rate for alpha-2 agonists, especially during initiation and discontinuation.
These strategies teach skills, modify behaviors, and create supportive environments.
- Behavior Therapy (Parent Training in Behavior Management for Children): Teaches parents specific skills to reinforce desired behaviors and reduce unwanted ones.
- Key Strategies:
- Positive Reinforcement: Praising, rewarding, or providing privileges for target behaviors (e.g., following instructions, completing tasks).
- Consistent Consequences: Implementing clear, predictable consequences for problematic behaviors (e.g., time-out, loss of privileges).
- Token Economy: Using a system of earning points or tokens for positive behaviors that can be exchanged for rewards.
- Structuring the Environment: Creating predictable routines, minimizing distractions, providing clear rules.
- Efficacy: Highly effective, especially for younger children, in improving behavior, parent-child relationships, and reducing ADHD symptoms. Often considered first-line for preschoolers with ADHD.
- Key Strategies:
- Behavioral Interventions in the School Setting: Classroom management techniques (e.g., daily report cards, positive reinforcement, clear rules), preferential seating, frequent breaks, reduced workload, use of organizational aids, peer tutoring.
- Efficacy: Improves academic performance, on-task behavior, and social interactions in school.
- Organizational Skills Training (for Older Children, Adolescents, and Adults): Teaches explicit strategies for time management, planning, organization, and problem-solving.
- Strategies: Using planners, calendars, checklists, breaking down large tasks, decluttering, managing distractions.
- Efficacy: Helps improve academic performance, reduce procrastination, and enhance daily functioning.
- Cognitive Behavioral Therapy (CBT) (for Adolescents and Adults): Helps individuals identify and change unhelpful thought patterns and behaviors.
- Strategies: Addressing negative self-talk, developing problem-solving skills, improving emotional regulation, managing impulsivity, stress management.
- Efficacy: Particularly useful for managing comorbid conditions (anxiety, depression), improving self-esteem, and developing coping strategies for ADHD-related challenges. Does not directly treat core ADHD symptoms but helps manage their impact.
- Social Skills Training: Explicitly teaches social cues, communication skills, conflict resolution, and empathy. Improves social interactions and peer relationships.
- Individualized Education Programs (IEPs) or 504 Plans: Legally mandated plans in schools to provide accommodations (e.g., extended time on tests, quiet testing environment, preferential seating, reduced distractions, use of technology) and specialized instruction to meet academic needs.
- Parent and Patient Education: Crucial for understanding ADHD, treatment options, potential side effects, and strategies for managing symptoms at home and in school/work.
- Regular Exercise: Can improve focus, reduce hyperactivity, and boost mood.
- Healthy Diet: While diet doesn't cause ADHD, balanced nutrition supports overall brain health. Some individuals report sensitivity to certain foods, though evidence for widespread dietary changes is limited.
- Adequate Sleep: Essential for managing symptoms; sleep hygiene strategies are critical.
- Mindfulness and Meditation: Can help improve attention regulation and emotional control in some individuals.
Children with ADHD need guidance and understanding from their parents, families, and teachers to reach their full potential and to succeed. For school age children, frustration, blame and anger may hinder recovery in other wards children need special help to overcome negative feeling and to develop new skills and attitudes.
- Social skills training; this will help the child learn how to behave in social situations by learning how their behaviours affect others
- Parenting skills training (behavioural parent management training) this teaches parents the skills to encourage and reward positive behaviours in their children. It helps parents learn how to use a system of rewards and consequences to change a child’s behaviour
- Stress management techniques, these can benefit parents of children with ADHD by increasing their ability to deal with frustration so that they can respond calmly to their child’s behaviour
- Support groups; these help parents and families connect with others who have similar problems and concerns. Groups often meet regularly to share frustration and successes to exchange information about recommended specialists and strategies and to talk with experts
- Diet; sugar, food colourings and additives as well as caffeine should be excluded in the patients diet as they aggravate hyperactivity
Help the child with ADHD to stay organised and stay organised by;
- Keeping a routine and a schedule. Keep the same routine every day from wake-up time to bedtime. Include times of homework, outdoor play and indoor activities. Write all changes on the schedule in advance as possible
- Organizing everyday items; have a place for everything and keep everything in its place. This includes clothing, backpacks and toys
- Using homework and notebook organizers. Stress to the child the importance of writing down assignments and bringing home necessary books
- Being clear and consistent. Children with ADHD need consistent rules they can understand and follow
- Giving praise or rewards when rules are followed. Children with ADHD often receive and expect criticism. Look for good behaviour and praise it.
- Develop a trusting relationship with the child that conveys acceptance of the child separate from unacceptable behaviour
- Ensure patient has a safe environment free from dangerous objects that can injure him due to random hyperactive movements
- Keep the child in an environment that is free from distractions to help him comply on given tasks
- Ensure child’s attention by calling his name and maintain an eye contact before giving instructions
- Ask patient to repeat instructions before beginning the task
- establish goals that allow the patient to complete part of the task, rewarding each step completion with a break for physical activity
- Provide assistance on one-to-one basis beginning with simple concrete instructions
- Gradually decrease the amount of assistance given to task performance while assuring patient that assistance is available if still needed
- Offer recognition for successful attempts and positive reinforcement for attempts made
- Provide quiet environment, self-contained classrooms an small group activities
- Help the patient to learn how to take his turn, wait in line and follow rules
- Provide information an materials related to the child’s disorder and effective parenting techniques
- Explain and demonstrate positive parenting techniques to parents such as being vigilant in identifying the child’s behaviour and responding positively to that behaviour
- Co-ordinate overall treatment plan with schools, child and family
- Impaired Attention
- Related to: Neurotransmitter imbalance (e.g., dopamine, norepinephrine dysregulation) affecting executive function, difficulty processing multiple stimuli, inconsistent processing of information.
- As evidenced by: Difficulty sustaining focus on tasks, frequent distractibility, difficulty following instructions, losing belongings, making careless errors, poor academic/work performance, difficulty with organization.
- Rationale: This is a direct reflection of the inattentive symptoms, impacting learning, task completion, and safety.
- Impaired Organizational Ability
- Related to: Deficits in executive function (e.g., planning, sequencing, prioritizing), difficulty with time management, chronic inattention.
- As evidenced by: Disorganized living/work space, difficulty completing multi-step tasks, frequently missing deadlines, misplacing items, poor planning for future events.
- Rationale: Directly addresses the functional impact of inattention and executive dysfunction on daily living and responsibilities.
- Deficient Knowledge (e.g., of effective study strategies, time management, disease process)
- Related to: Impaired attention, difficulty with information processing, lack of prior education on condition.
- As evidenced by: Verbalization of unfamiliarity, inappropriate or inefficient performance of tasks, frequent academic/work difficulties despite effort, questions about ADHD.
- Rationale: Individuals and families often lack comprehensive understanding of ADHD and effective coping strategies.
- Risk for Injury
- Related to: Impulsive behavior, hyperactivity, reduced hazard perception, restless motor activity, difficulty inhibiting responses.
- As evidenced by: (This is a "risk for" diagnosis, so it doesn't have "as evidenced by" statements, but rather risk factors like:) Frequent accidents or near-misses, engaging in dangerous activities, difficulty adhering to safety rules, tendency to rush tasks.
- Rationale: Hyperactivity and impulsivity increase the likelihood of accidents and unsafe behaviors.
- Impaired Impulse Control
- Related to: Neurotransmitter dysregulation affecting inhibitory control, difficulty delaying gratification, underdeveloped prefrontal cortical function.
- As evidenced by: Interrupting others, blurting out answers, difficulty waiting turns, making hasty decisions, engaging in risky behaviors, frequent social conflicts.
- Rationale: Directly addresses the core impulsive symptom, impacting social interactions and decision-making.
- Disrupted Sleep Pattern
- Related to: Hyperactivity, restlessness, difficulty winding down, medication side effects (stimulants), comorbid anxiety.
- As evidenced by: Difficulty falling asleep, frequent awakenings, non-restorative sleep, daytime fatigue, irritability.
- Rationale: Sleep disturbances are common in ADHD and can exacerbate symptoms.
- Low Self-Esteem
- Related to: Chronic academic/social difficulties, negative feedback from peers/adults, perception of personal failures, co-occurring anxiety/depression.
- As evidenced by: Negative self-talk, withdrawal from social situations, difficulty accepting compliments, expression of feelings of worthlessness, avoidance of new challenges.
- Rationale: Repeated failures and criticisms can significantly erode self-worth.
- Impaired Social Interaction
- Related to: Impulsivity (e.g., interrupting), difficulty with turn-taking, inattention to social cues, difficulty regulating emotions, peer rejection.
- As evidenced by: Few close friendships, reports of being disliked, difficulty maintaining conversations, conflicts with peers, misinterpreting social cues.
- Rationale: Core symptoms of ADHD can interfere with developing and maintaining healthy social relationships.
- Ineffective Coping (Individual or Family)
- Related to: Inadequate problem-solving skills, overwhelming demands of managing ADHD symptoms, insufficient support systems, presence of co-occurring conditions, caregiver burden.
- As evidenced by: Verbalization of inability to cope, difficulty with decision-making, maladaptive behaviors, strained family relationships, exacerbation of symptoms.
- Rationale: Addresses the challenges individuals and families face in managing a chronic condition.
- Risk for Inadequate protein energy nutritional intake (especially relevant with stimulant medication)
- Related to: Anorectic side effects of stimulant medication, decreased appetite.
- As evidenced by: (Risk diagnosis) Reports of decreased appetite, weight loss, verbalization of food aversion after starting medication.
- Rationale: Stimulants can suppress appetite, necessitating monitoring of nutritional intake.
Given the chronic nature of the condition, its varied presentations across age groups, and the complexity of multimodal treatment, nurses are often at the forefront of assessment, education, advocacy, and coordination of care.
- Screening: Nurses in various settings (pediatric clinics, schools, primary care) are often the first to screen for ADHD symptoms during routine visits. They can administer standardized screening tools and observe behaviors indicative of ADHD.
- Detailed History Taking: Collecting comprehensive developmental, medical, family, and psychosocial histories from patients and families.
- Symptom Evaluation: Systematically assessing for core ADHD symptoms (inattention, hyperactivity, impulsivity) and their impact on functioning across multiple settings (home, school, work, social).
- Comorbidity Assessment: Identifying potential co-occurring conditions (e.g., anxiety, depression, learning disabilities, ODD, sleep disorders) that frequently accompany ADHD and can complicate diagnosis and treatment.
- Differential Diagnosis Support: Gathering information to help rule out other medical or psychiatric conditions that might mimic ADHD symptoms.
- Psychoeducation: Providing individuals and families with accurate, evidence-based information about ADHD, including its neurobiological basis, symptoms, course, and treatment options. Dispelling myths and reducing stigma.
- Treatment Rationale: Explaining the purpose, expected benefits, potential side effects, and administration guidelines for both pharmacological and non-pharmacological interventions.
- Behavior Management Strategies: Teaching parents and caregivers effective behavioral techniques (e.g., positive reinforcement, consistent consequences, token economies, establishing routines) to manage challenging behaviors and promote desired ones.
- Organizational and Study Skills: Counseling older children, adolescents, and adults on strategies for time management, planning, organization, note-taking, and reducing distractions.
- Lifestyle Modifications: Educating on the importance of healthy diet, regular exercise, adequate sleep, and stress management in mitigating ADHD symptoms.
- Coping Strategies: Helping individuals develop effective coping mechanisms for frustration, emotional dysregulation, and low self-esteem often associated with ADHD.
- Administration Education: Instructing patients/families on the correct dosage, timing, and method of administration for prescribed medications (e.g., stimulants, non-stimulants).
- Side Effect Monitoring: Assessing for and educating about common and serious side effects of ADHD medications (e.g., appetite suppression, sleep disturbances, cardiovascular changes for stimulants; GI upset for atomoxetine; sedation for alpha-agonists).
- Therapeutic Response Evaluation: Monitoring the effectiveness of medication in reducing target symptoms and improving functioning, often using rating scales and patient/family reports.
- Growth Monitoring: For children on stimulant medication, regularly monitoring height and weight to track growth.
- Cardiovascular Monitoring: Taking baseline and regular blood pressure and heart rate measurements, especially for individuals on stimulant or alpha-agonist medications.
- Adherence Promotion: Addressing barriers to medication adherence and promoting consistent medication use as prescribed.
- Collaboration with Multidisciplinary Team: Working closely with physicians, psychiatrists, psychologists, social workers, teachers, and other specialists to ensure integrated and comprehensive care.
- School Liaison: Communicating with school personnel (teachers, counselors, special education staff) to facilitate academic accommodations (IEPs, 504 plans), behavioral interventions in the classroom, and exchange of information.
- Referrals: Facilitating referrals to specialists (e.g., occupational therapy for sensory issues, tutoring for learning disabilities, therapy for mental health comorbidities).
- Advocacy: Advocating for the individual's needs within healthcare systems, educational settings, and the community. Empowering patients and families to advocate for themselves.
- Resource Navigation: Connecting families to support groups, community resources, and reliable information sources.
- Children and Adolescents: Focus on psychoeducation for parents, behavior management strategies, school collaboration, medication monitoring, and supporting social skill development.
- Adults: Emphasis on medication adherence, organizational skills, stress management, coping with comorbidities (anxiety, depression), workplace accommodations, and managing the impact of ADHD on relationships and daily responsibilities.
- Geriatric Population: While less common for initial diagnosis, nurses might encounter older adults managing lifelong ADHD, focusing on medication interactions, cognitive changes, and maintaining functional independence.
Satisfied
thanks for the notes they are good to understand