Merkel Cell Polyomavirus (MCPyV)
Merkel Cell Polyomavirus (MCPyV) & Human Cancer
By the conclusion of this highly detailed master guide, you will be deeply conversant with:
- The virological characteristics and genomic structure of Merkel Cell Polyomavirus (MCPyV).
- The precise molecular mechanisms of the Large T-Antigen and Small T-Antigen in cellular transformation (the Rb and PP2A pathways).
- The clinical presentation, high-risk demographics, and exact diagnostic markers of Merkel Cell Carcinoma (MCC).
- The catastrophic molecular event of viral integration and T-Antigen truncation that traps the host cell in an infinite division cycle.
- The specific research aims utilized to establish MCPyV as a direct human tumor-causing virus.
I. Introduction & Definition
Merkel Cell Polyomavirus (MCPyV) is a recently discovered virus strongly implicated in human oncology. Discovered in 2008 by researchers Patrick Moore and Yuan Chang, it is firmly and universally associated with Merkel Cell Carcinoma (MCC), which is a highly aggressive, rapidly metastasizing, and deadly skin malignancy.
Viral Characteristics:
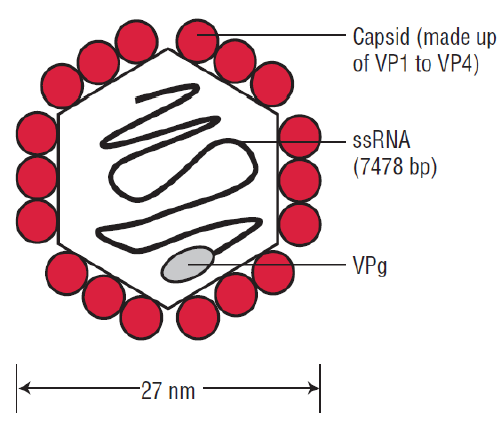
- Size: It is a very small virus (approximately 40–50 nm in diameter).
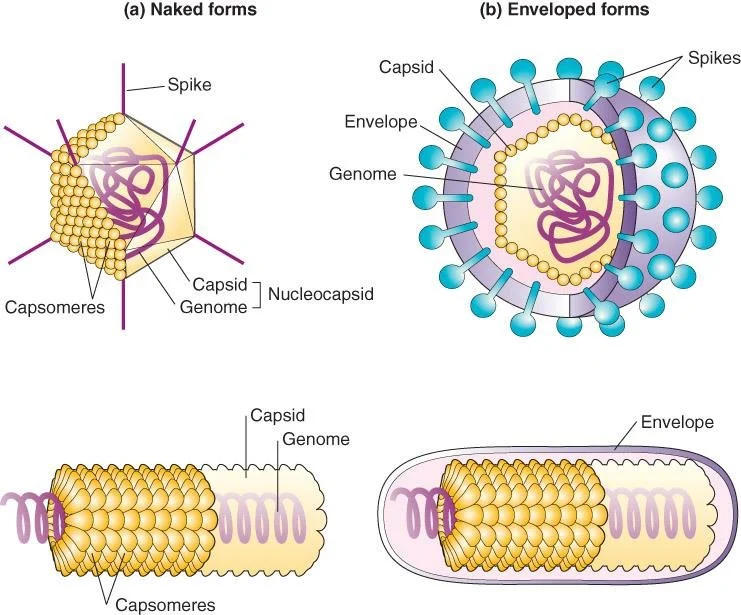
- Structure: It is non-enveloped (meaning it lacks a delicate outer lipid bilayer). Because it lacks this lipid envelope, the virus is highly resistant to environmental degradation, heat, drying, and routine alcohol-based hand sanitizers. It consists purely of a tough, icosahedral protein capsid protecting its DNA.
- Genome: It is a double-stranded DNA (dsDNA) virus.
- Oncogenic Potential: Like other viruses in the polyomavirus family, it is naturally capable of inducing tumorigenesis (cancer formation) under specific host conditions.
- Context: Polyomaviruses are known, well-documented pathogens of birds and mammals, including humans. The best-characterized and most heavily studied polyomavirus historically is SV40 (Simian Virus 40), which was discovered in monkeys and serves as the ultimate laboratory model for understanding how MCPyV behaves in humans.
II. Classification of the Virus & Clinical Anatomy
MCPyV belongs to a specific taxonomic lineage among the human polyomaviruses. Other members of this human-infecting family include the previously characterized BK virus (which causes nephropathy in transplant patients) and JC virus (which causes Progressive Multifocal Leukoencephalopathy [PML] in HIV/AIDS patients), as well as the novel WU and KI viruses.
- Family: Polyomaviridae
- Genus: Alphapolyomavirus
- Species: Alphapolyomavirus quintihominis
- Pathological Consequence: Causes Merkel cell carcinoma (MCC).
What is a Merkel Cell?
Merkel cells are specialized, oval-shaped receptor cells found deep in the stratum basale (the deepest layer of the epidermis) of the skin. They are densely innervated by somatosensory nerve endings and are uniquely responsible for high-resolution light touch sensation (e.g., feeling the fine texture of an object, reading Braille).
Because they share features with both epithelial cells (skin cells) and nerve cells (they contain neurosecretory granules filled with neurotransmitters), tumors arising from them exhibit highly specific neuroendocrine features. This makes MCC a cutaneous neuroendocrine carcinoma.
III. The Polyomavirus Genome & Life Cycle
Genomic Structure:
The viral genome is incredibly compact, highly organized, and circular. It contains approximately 5,000 base pairs. It is structurally divided into three distinct functional regions:
- The Regulatory Region: Contains the origin of replication (Ori) and bidirectional promoter/enhancer elements. This acts as the "control room" directing where and when transcription begins.
- The Early Unit: Transcribed immediately upon infection of the host cell. It encodes the non-structural, highly oncogenic proteins responsible for hijacking the cell: the Large T-antigen (LT) and the Small T-antigen (sT).
- The Late Unit: Transcribed later in the cycle, only after viral DNA replication has begun. It encodes the viral structural capsid proteins (VP1, VP2, and VP3) needed to physically build the new viruses.
The Viral Life Cycle (Lytic vs. Lysogenic):
The ultimate outcome of a polyomavirus infection depends entirely on whether the host cell is "permissive" (allows the virus to complete its lifecycle) or "nonpermissive."
The Lytic Phase
The virus successfully infects the cell, commandeers the cellular machinery, and forces the cell to undergo massive, rapid viral replication. This intense manufacturing process culminates in complete cell lysis (death) and the bursting release of thousands of infectious progeny virions to infect neighboring cells. (Note: Dead cells cannot form tumors).
The Lysogenic / Transformation Phase
The virus infects the cell but cannot complete its full replication cycle. There is a total loss of lytic potential. In a rare, catastrophic biological event, the viral DNA accidentally requires integration into the host cell's chromosomal genome. Because the host cell does not die, the integrated viral DNA continually produces Early Unit proteins (T-antigens), constantly pushing the cell to divide. This leads directly to cellular transformation, immortality, and tumor formation.
IV. Virulence Factors: The Tumor Antigens (TAg)
The true oncogenic (cancer-causing) power of MCPyV lies hidden in its Early Unit proteins, specifically the Large and Small T-Antigens. These are functional polyomavirus proteins designed to bind to and degrade or sequester the host cell's natural tumor suppressors, thereby actively promoting S-phase entry (forcing the cell into the DNA synthesis phase of the cell cycle).
1. Large T Antigen (LT Antigen):
This is the major virulence protein and the primary driver of transformation.
- Structure & Domains: The LT protein (approximately 817 amino acids long) contains several critical motifs (functional sections):
- DnaJ (Hsc70-binding motif): Interacts with cellular chaperones to alter host protein folding and stability.
- Rb-binding motif (LXCXE motif): The absolute critical domain for oncogenesis.
- Ori binding domain: Binds the viral replication origin and regulatory elements to initiate viral replication.
- Helicase domain: Unwinds DNA. Perpetuates the synthesis of a large number of progeny and induces cell lysis in permissive cells.
- p53-binding sites: Interacts with the p53 tumor suppressor (though its exact role in MCPyV differs from SV40).
- Mechanism of Action (The Rb Pathway): It heavily interferes with normal cell cycle regulation. It does this by aggressively binding and inactivating the ultimate tumor suppressor protein, Retinoblastoma (pRb).
Physiology Expansion: The pRb/E2F "Brakes"
Normally, pRb acts as the absolute "brakes" of the cell cycle. It holds tightly onto a transcription factor called E2F, preventing the cell from dividing. When the LT Antigen binds to pRb, it physically rips pRb away from E2F. The newly freed E2F travels straight to the nucleus and commands the cell to divide endlessly, pushing infected cells into uncontrolled, catastrophic divisions.
2. Small T Antigen (sT Antigen):
While originally thought to be secondary, sT is now considered a profoundly strong oncogenic virulence factor in its own right.
- Mechanism of Action: Enhances viral replication and cell transformation by activating cellular pathways involved in rampant cell growth and survival. Specifically, it aggressively inhibits protein phosphatase 2A (PP2A).
Physiology Expansion: The PP2A "Off Switch"
PP2A is a vital cellular enzyme that removes phosphate groups from signaling proteins. Removing phosphates normally acts to turn "off" powerful growth signals (like the MAP kinase and mTOR pathways). By physically inhibiting PP2A, the sT Antigen ensures that cellular growth pathways stay permanently switched "on," leading to abnormal signaling and massively increased, unrestrained cellular proliferation.
To easily remember exactly how the virus causes cancer on an exam, think: "Large Rb, Small PP"
- Large T-Antigen blocks pRb (Releasing the brakes on the cell cycle).
- Small T-Antigen blocks PP2A (Keeping the growth signals permanently turned on).
V. Infection Dynamics: Immune Evasion, Persistence & Latency
How does a virus that infects almost the entire human population only cause cancer in a very select few? The answer lies in the dynamic, lifelong interplay between the virus's stealth mechanisms and the host's immune system.
1. Immune Evasion:
The virus usually causes a completely asymptomatic infection in healthy individuals. It evades immune detection through three primary mechanisms:
- Reduced presentation of viral antigens to surveying T-cells.
- Direct molecular interference with host immune signaling pathways.
- Quiet persistence inside host skin cells as a circular episome without causing immediate damage (avoiding the triggering of inflammatory alarms).
2. Viral Integration into Host Genome:
In Merkel cell carcinoma, the viral DNA does not stay as a free-floating circle (episome). Instead, it undergoes clonal integration directly into the host cell's chromosomes. This accidental integration makes the infected cells continuously, permanently express oncogenic proteins (the T-antigens), which contributes directly to irreversible malignant transformation.
3. Persistence and Latency:
Most people in the general population are actually infected with MCPyV during early childhood (likely through skin-to-skin contact). The virus establishes long-term persistence (latency) in the skin and remains harmless (asymptomatic) for decades, as long as the host's robust immune system keeps it strictly in check.
The Trigger for Disease: MCC mainly develops when host cellular immunity is severely weakened, allowing the virus to reactivate and mutate. High-risk populations include:
- Elderly individuals (due to natural immunosenescence—the aging of the immune system).
- Immunocompromised patients (e.g., individuals living with uncontrolled HIV/AIDS).
- Organ transplant recipients (who are actively and permanently taking immunosuppressive drugs, like Tacrolimus or Cyclosporine, to prevent organ rejection).
❓ Applied Clinical Question: Viral Integration
Question: A 65-year-old kidney transplant patient develops a rapidly growing, painless, purple nodule on his neck. A biopsy reveals Merkel Cell Carcinoma. If the virus has been living harmlessly in his skin since childhood, why did the tumor only form now, and what specific molecular event had to occur to the viral DNA for this to happen?
Answer: The tumor formed now because his immune surveillance was artificially suppressed by the lifelong anti-rejection drugs required for his kidney transplant. However, immunosuppression alone doesn't instantly cause the cancer. The absolutely required molecular event is Viral DNA Integration into the host genome. The virus transitioned from a quiet, latent, free-floating state to being permanently stitched into the host DNA. This resulting architectural change triggered the continuous, unstoppable production of Large and Small T-Antigens that forced the cell into malignant transformation.
VI. Merkel Cell Carcinoma (MCC): Clinical Features
Before the discovery of MCPyV, Merkel Cell Carcinoma was known only as the deadliest form of skin cancer with a totally unknown origin/etiology. It is characterized by a rapidly increasing number of cases globally, frequent early metastases to regional lymph nodes, and a historical lack of effective treatments.
Clinical Presentation & Risk Factors:
- It presents as an aggressively fast-growing skin cancer.
- Usually appears as a painless nodule that may be red, purple, pink, or skin-colored, frequently possessing a shiny surface.
- Enlarged, firm lymph nodes are palpable if regional metastasis has already occurred (which is common at the time of initial diagnosis).
- High-Risk Demographics: It is highly prevalent in immunosuppressed patients (HIV, organ transplants, chronic lymphocytic leukemia patients) and is vastly more common in fair-skinned individuals.
- Location: Commonly occurs on severely, chronically sun-exposed areas such as the face, neck, and extensor surfaces of the arms. (UV radiation acts as a potent local immunosuppressant and a DNA-damaging mutagen).
The Clinical Features of MCC: "AEIOU"
Dermatologists use the "AEIOU" mnemonic to rapidly identify suspected Merkel Cell Carcinoma in a clinical setting:
- Asymptomatic (Painless nodule, lack of tenderness).
- Expanding rapidly (Doubling in size in weeks, not months).
- Immunosuppression (History of transplant, HIV, or chronic disease).
- Older than 50 (Peak incidence in the 70s).
- UV-exposed skin (Occurs predominantly on sun-damaged, fair skin).
VII. Diagnosis and Treatment of MCC
Diagnosis:
- Clinical Examination: Suspicious, rapidly growing skin lesions matching the AEIOU criteria are thoroughly examined.
- Skin Biopsy: Confirms the diagnosis histologically. Under the microscope, MCC presents classically as a "small round blue cell tumor" with high mitotic activity (many cells visibly dividing) and distinct neuroendocrine features.
- Immunohistochemistry (IHC): Essential to differentiate MCC from other small round blue cell tumors (like metastatic small cell lung cancer, melanoma, or lymphoma). Typical markers include:
- CK20 positive: Cytokeratin 20 shows a highly characteristic "dot-like" pattern (perinuclear accumulation of intermediate filaments). This is the hallmark diagnostic stain.
- Chromogranin: Positive (confirms neuroendocrine origin by highlighting neurosecretory granules).
- Synaptophysin: Positive (also confirms neuroendocrine origin).
- Note: MCC is typically Thyroid Transcription Factor-1 (TTF-1) negative, which helps differentiate it from small cell lung cancer (which is TTF-1 positive).
Treatment Modalities:
- Surgery: Wide local excision (WLE) with massive margins is the primary, main treatment for localized disease. Sentinel lymph node biopsy is universally performed to check for microscopic spread.
- Radiotherapy: Often used after surgery (adjuvant) to kill any remaining microscopic cancer cells in the tumor bed or draining lymph nodes, as MCC is remarkably radiosensitive.
- Immunotherapy: A massive, recent breakthrough for advanced, metastatic MCC. Important drugs include Pembrolizumab, Avelumab, and Nivolumab.
Physiology Expansion: Because MCC is fundamentally driven by a foreign virus, the tumor cells are highly immunogenic (they look foreign to the body). To survive, tumors express PD-L1 to put the immune system to sleep. These immunotherapy drugs are PD-1/PD-L1 inhibitors that "take the brakes off" the patient's immune system, allowing circulating T-cells to recognize and destroy the virally infected cancer cells. - Chemotherapy: Used as a salvage therapy in advanced/metastatic disease, but clinical responses are notoriously short-lived, and the cancer almost always recurs.
VIII. The MCPyV Hypothesis & Genomic Evidence
Researchers investigating MCC tumors discovered low copy number polyomavirus-like transcripts in 80% to 90% of all MCC tumors globally. Furthermore, they definitively found that the viral DNA had undergone clonal DNA integration into the human genome, meaning the virus was present before the tumor expanded.
The T-Antigen Truncation Mutation (Extremely High-Yield Concept)
Sequencing of the integrated viral genome in MCC tumors revealed highly specific point mutations in the TAg-encoding gene. These specific mutations are predicted to result in the synthesis of a truncated (shortened) protein due to premature stop codons.
Two distinct truncating mutations were identified (labeled MCV350 and MCV339). Only two MCPyV genomes were initially sequenced to find this profound pattern.
💡 Why MUST the T-Antigen be truncated to cause cancer?
This is the core, beautiful paradox of MCPyV oncogenesis!
The wild-type (WT) virus wants to replicate. Its Large T-Antigen has two main functional ends: a front end that binds pRb (forcing the cell to replicate its DNA to provide building blocks for the virus) and a back end with a Helicase domain (which utilizes those building blocks to replicate the viral genome and ultimately kills/lyses the cell to escape).
If the virus replicates and kills the cell, cancer cannot form (dead cells don't form tumors). Therefore, for a tumor to develop, the viral DNA integrates into the host chromosome and suffers a highly specific truncating mutation that literally chops off the Helicase domain. The resulting truncated T-Antigen still possesses the front end to block pRb (forcing the cell to divide forever), but it can no longer replicate the virus or lyse the cell. The cell is permanently trapped in an infinite division cycle without dying, resulting in a tumor!
The Working Hypothesis:
- Normal Pathway: Wild-type MCPyV infects permissive human cells, successfully replicates using intact helicase, and causes cellular lysis, which releases infectious progeny into the environment.
- Oncogenic Pathway: Mutated MCPyV infects a cell and accidentally integrates into its genome. This results in tumor transformation because the truncated TAg forces division without lysis. The transformed cell initiates tumors, which rapidly expand and lead to further aggressive metastases.
IX. Research Aim 1: The Transforming and Oncogenic Potentials of MCPyV
Scientists utilized specific molecular assays to definitively prove that MCPyV could cause cancer.
Question: Does MCPyV T-antigen immortalize human cells in vitro?
- Background: SV40 TAg immortalizes mammalian cells in vitro. Normally, primary laboratory cells divide a set number of times (the Hayflick limit) and senesce (die of old age). Transformed cells proliferate indefinitely. If MCPyV TAg causes cellular transformation, primary cells should become immortalized.
- Experiment: MCPyV and SV40 TAgs were artificially delivered to cultured cells using modified retroviruses.
- Result: MCPyV may cause cellular transformation, but NO, it does not immortalize cells exactly in the same robust manner as SV40. The p53-binding sites may be required (which MCPyV lacks or utilizes differently). Wild-Type (WT) TAg is continually used to further refine and answer this discrepancy.
Question: Can MCPyV cause tumors in laboratory animals?
- Background: Murine (mouse) PyV causes tumors in mice; SV40, JC, and BK viruses rapidly induce brain tumors when injected into hamsters and rats. Is MCPyV also a definitive tumor-causing agent in animals?
- Experiment: Inject newborn, immunologically naive hamsters with the virus and systematically examine their bodies for the development of tumors. Presence of a tumor strongly suggests in vivo oncogenic potential.
- Result: NO direct tumors formed in standard animal models using simply the virus. Complex mutations in VP (viral protein) genes or artificial SV40/JC/BK/MC recombinants are strictly needed to answer this question definitively in animal models.
X. Research Aim 2: Identification of WT MCPyV & Infectivity
- Question 1: Is Wild-Type (WT) MCPyV present in non-tumor tissues of MCC patients or the environment (air, dust, parasites)?
- Action: Researchers utilized targeted PCR (Polymerase Chain Reaction) to amplify the TAg and VP-coding genes from various environmental and tissue swabs, and sequenced the resulting viral DNA to find out the virus's natural reservoir.
- Question 2: Is WT MCPyV capable of lytic growth?
- Background: Polyomaviruses natively cause lytic death of permissive cells. The WT (whether a clinical isolate or laboratory recombinant) MCPyV is theoretically expected to be capable of lytic growth. Lytic growth results in a massive abundance of free virions and allows measuring infectivity via a standard plaque assay.
- Result: The truncated TAg found specifically in tumors is strictly and biologically incapable of driving the lytic phase. Recombinant WT viruses generated in the lab may contain additional, unknown mutations depriving such a virus from lytic potential in culture. Thus, while WT MCPyV easily infects humans globally, it ONLY causes tumors upon the catastrophic loss of lytic potential via mutation.
XI. Research Aim 3: Mechanism of MCPyV-Induced Transformation
This aim explores the exact, granular molecular biology of how the viral proteins hijack the human cell cycle.
- Protein Interactions: Do MCPyV proteins interact with cellular partners?
- Tested using: Co-immunoprecipitation (using antibodies against TAg, VP, and cellular proteins to pull them out of solution together), Yeast two-hybrid systems (to test for direct interactions between TAg and cellular tumor suppressors from a genetic expression library), and BiFC (Bimolecular Fluorescence Complementation).
- Result: Yes, MCPyV proteins interact intimately with specific cellular partners, directly leading to transformation.
- Stability & Expression: Is the stability of mRNA and expression of MCPyV proteins affected?
- Tested using: Proteins were analyzed via Western hybridization (blot). mRNA stability was tested via quantitative rtPCR (DTS).
- Result: MCV339 and MCV350 (the truncated, mutated tumor proteins) are highly stable and synthesized continuously without degradation.
Epistasis Analysis of TAg
Goal: Identify the exact mechanism of MCPyV TAg-mediated transformation. SV40 T-antigen is historically known to interact with both pRb and p53 to deregulate the cell cycle and simultaneously prevent apoptosis.
Experiment: Introduce TAg to cells or animal models that have already been genetically depleted (knocked out) of pRb and p53. This is called an epistasis analysis.
Logic: If removing pRb/p53 causes transformation on its own, and adding TAg causes the exact same transformation without adding any extra effects, they are scientifically operating in the exact same genetic pathway (Epistatic).
Results: Transformation occurs strictly via the disruption/transactivation of these pathways. TAg-dependent degradation of pRb is mathematically and biologically sufficient for full tumor transformation. Unknown tumor suppressors/oncogenes may also be involved but pRb is the primary key.
The Role of p53: Are p53-binding sites necessary for transformation?
Conclusion: NO. TAg-dependent degradation of pRb is entirely sufficient for tumor transformation in MCPyV, setting it apart from SV40 which heavily relies on p53 disruption.
Interestingly, researchers found that truncating mutations likely occurred after initial transformation. Translation re-initiation allows some minute synthesis of the C-terminus of the protein, aiding the tumor's survival.
XII. Summary, Significance, and Future Directions
Summary:
Merkel Cell Carcinoma (MCC) is a deadly, aggressive skin cancer with a previously completely unknown etiology and a severe lack of effective historical treatments. The compelling, molecular evidence of a novel polyomavirus capable of directly causing cancer allows for the development of highly targeted MCC treatments. MCPyV provides a direct, undeniable association between a human cancer and infectious polyomaviruses, shifting the paradigm of dermatological oncology.
Future Directions of Research:
- Test for the presence of MCPyV in other types of poorly understood human tumors.
- Explore the exact mechanism by which MCPyV natively spreads among humans (e.g., respiratory, fecal-oral, or direct dermal contact).
- Test whether TAg truncation is a universal, common feature of absolutely all MCPyV-induced tumors globally.
- Estimate true seropositivity (how many people have circulating antibodies against it) among the general, healthy human population.
- Develop effective, targeted antiviral drugs or preventative immunologic treatments (like vaccines similar to the HPV vaccine).
❓ Final Module Review Question
Question: Based on the epistasis analysis and molecular mechanics discussed, why is immunotherapy (specifically PD-1/PD-L1 inhibitors like Pembrolizumab) a logical and highly effective treatment for an advanced Merkel Cell Carcinoma, whereas it might completely fail in a standard, non-viral melanoma?
Answer: Because MCC is fundamentally an infection-driven tumor. The tumor cells are actively and continuously expressing viral antigens (the truncated Large and Small T-Antigens). Because these are inherently foreign viral proteins, the patient's immune system naturally recognizes them as non-self and desperately wants to attack them. However, the tumor survives by hiding, overexpressing PD-L1 checkpoint proteins to "turn off" the attacking T-cells. By administering Immunotherapy to chemically block those checkpoints, the immune system "wakes up," clearly recognizes the foreign viral proteins on the cancer cells, and aggressively destroys the tumor. Standard melanomas driven purely by UV damage may lack these highly visible foreign antigens, making them harder for the immune system to target.
XIII. References & Suggested Reading
- Feng, H., Shuda, M., Chang, Y., & Moore, P. S. (2008). Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science, 319(5866), 1096-1100. (The landmark paper discovering MCPyV).
- Shuda, M., et al. (2008). T antigen mutations are a human tumor-specific signature for Merkel cell polyomavirus. Proceedings of the National Academy of Sciences, 105(42), 16272-16277.
- Houben, R., et al. (2010). Merkel cell polyomavirus-infected Merkel cell carcinoma cells require expression of viral T antigens. Journal of Virology, 84(14), 7064-7072.
- Schrama, D., et al. (2012). The role of Merkel cell polyomavirus in Merkel cell carcinoma. Current Opinion in Oncology, 24(2), 141-149.
- Nghiem, P. T., et al. (2016). PD-1 Blockade with Pembrolizumab in Advanced Merkel-Cell Carcinoma. New England Journal of Medicine, 374(26), 2542-2552. (Landmark clinical trial for Immunotherapy in MCC).
Quick Quiz
Virology Intro Quiz
Microbiology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Virology Intro Quiz
Microbiology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.
Merkel Cell Polyomavirus (MCPyV) Read More »