


Oral Contraceptive Pills
There are two main types of hormonal oral contraceptive formulations:
- Combined hormonal contraceptive methods which contain both oestrogen and progestin thus, they are called combined oral contraceptives (COCs)
- One which contains only progesterone or one of its synthetic analogues (Progestins) thus, it is called progestogen-only pills (POPs) method.
(i) Combined Oral Contraceptive Pills (COC)
Combined oral contraceptives contain both oestrogen and progesterone. It achieves effects of both hormones. Oestrogen suppresses ovulation and progesterone creates unfavourable conditions for egg transport and thickening of the cervical mucus to impair sperm entrance into the canal.
Examples
- Lo-femenal
- Pill Plan (Duofen)
- Microgynon
Mechanism of Action:
Combined methods work by:
- Suppressing ovulation (estrogenic effect)
- Thickening cervical mucus, making it difficult for sperm to penetrate the uterus
- Making the endometrium unsuitable for implantation of a fertilized egg (thin and atrophic due to constant progestogenic action)
- Reducing sperm transport in the upper genital tract (fallopian tubes).
Effectiveness:
- 92 – 99.9% effective, depending on user compliance.
- In very young women, typical effectiveness can be as high as 95.3%.
- Failure rates decline with the duration of use and age of the user.
- Failures may be due to method failure, client error, incomplete information from service providers, drug interactions, severe vomiting/diarrhoea, or expired pills.
Advantages:
- Very effective if taken correctly.
- Effective immediately.
- Easily reversible.
- Few side effects.
- Convenient and easy to use.
- Does not interfere with intercourse.
- Causes regular and predictable periods.
- May improve anemia.
- Reduces dysmenorrhea and premenstrual tension.
- Protects against ovarian and endometrial cancer, and some causes of PID.
- Reduces the risk of ovarian cysts, benign breast disease, and ectopic pregnancy.
- Can be provided by trained non-medical staff.
Disadvantages:
- Effectiveness depends on daily pill intake, requiring strong motivation.
- Increases chances of promiscuity.
- Can cause Candida vulvitis and vaginitis.
- May lead to thromboembolism and benign/malignant liver tumors.
- Requires regular and dependable supply.
- Reduces breast milk, especially in the first 6 months after delivery.
- Not the most appropriate choice for lactating women unless no other method is available and there is a high risk of pregnancy.
Indications:
- Women requiring a highly effective method.
- Women wanting an easily reversible method.
- Non-breastfeeding women or breastfeeding women after 6 months.
- Women who are anaemic with heavy menstrual bleeding.
- Women with a history of ectopic pregnancy.
- Nulliparous women.
- Women with a history of benign, functional ovarian cysts.
- Women with a family history of ovarian cancer.
- Women with menstrual cycle symptoms or irregular menstrual cycles.
Contraindications:
- Absolute contraindications include cardiovascular diseases, liver disease, pregnancy, undiagnosed per vaginal bleeding, and oestrogen-dependent neoplasms.
- Relative contraindications include obesity, varicosities, epilepsy, asthma, mood disorders, nursing mothers in the first 6 months, smoking, and gallbladder disease.
Side Effects:
- Major side effects include hypertension, venous thromboembolism, and cholestatic jaundice.
- Minor side effects can be due to oestrogen, progestin, or both, including nausea, vomiting, headache, leg cramps, weight gain, chloasma & acne, breakthrough bleeding, hypomenorrhea, amenorrhea, leucorrhea, and decreased libido.
Danger Signs of COCs:
- Acute abnormal pain.
- Severe headaches with blurred vision.
- Pain in the chest with difficulty in breathing.
- Pain in the calf muscles.
Indications for Withdraw:
- Severe migraine.
- Visual disturbance.
- Sudden chest pain.
- Severe cramps.
- Excessive weight gain.
- Severe depression.
- Patient wanting pregnancy.
- Awaiting major surgery.
Drug Interaction:
- Decreases effectiveness of methyldopa, oral anticoagulants, and oral hypoglycemics.
- Increases effectiveness of B blockers, corticosteroids, diazepam, aminophylline, and alcohol.
- Other drugs that increase COC metabolism include phenobarbitone, antiepileptics (except sodium valproate and clozapine), rifampicin, griseofulvin, spironolactone, and ketoconazole.


Implants
Implants are small, flexible rods or capsules that are inserted under the skin of a woman’s upper arm.
These implants release a steady, low dose of hormones (usually a progestin hormone) into the bloodstream over an extended period. The most common types of contraceptive implants include Implanon, Jadelle, and Norplant.
Implants are considered a reversible form of contraception, and their effectiveness is not dependent on user compliance once inserted. They are suitable for women who want a reliable, long-term birth control option without the need for daily or frequent intervention.
Types:
- Implanon: A single rod capsule effective for 3 years.
- Jadelle: Two rods of levornogestrel each 75mg capsules providing protection for 5 years.
- Norplant: Consists of 6 rods each with 36mg levornogestrel capsules labelled for 5-7 years.
Modes of Action:
The hormonal release from these implants serves to prevent pregnancy by thickening the cervical mucus within 24 hours, hindering sperm entry into the uterus, inhibiting ovulation (the release of eggs from the ovaries), and altering the uterine lining to make it less receptive to a fertilized egg. Implants are highly effective and offer long-term contraception, ranging from three to seven years, depending on the specific type.
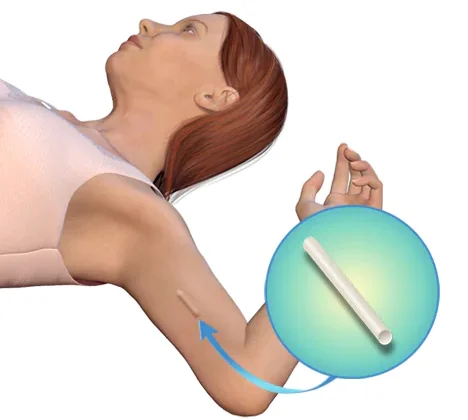
Insertion: Inner aspect of non dominant arm, 6 – 8 cm above elbow fold under local anesthesia. This is at day1, immediate after abortion or 3weeks postpartum.
Removal: Approximately 3 to 5 years
Advantages:
- Very effective within 24 hours after insertion.
- Easily reversible with no delay in returning to fertility after removal.
- Reduces frequency and intensity of sickle cell crises.
- Highly effective for long-term contraception.
- Shares benefits with Depo Provera.
Common Side Effects and Disadvantages:
- Changes in menstruation patterns.
- Spotting.
- Rare instances of heavy bleeding.
- Amenorrhea.
- Does not protect against STIs, including HIV/AIDS.
- Discomfort in the hand after insertion.
- Possible weight changes (overweight or weight loss).
- Minor surgical procedure required for both insertion and removal.
Indications:
- Breastfeeding post-partum mothers.
- Adolescents.
- Post-abortion contraception.
- Women with sickle cell disease.
- Women awaiting surgical contraception.
- Women on treatment, e.g., ARVs.
Contraindications:
- Serious problems with the heart or blood vessels.
- Breast cancer history.
- Liver diseases leading to jaundice.
- Pregnancy.
Signs and Problems Requiring Medical Attention:
- Soreness at the site of insertion.
- Capsules coming out.
- Severe headaches.
- Heavy bleeding, exceeding the usual amount and duration.
- Pregnancy.
- Missed period after several regular cycles.
Injectable Contraceptives
Examples
- Depo Provera (Depo Medroxyprogesterone acetate (DMPA), single dose of 150 mg I.M every 12 weeks. (Injecta Plan)
- Sayana Press 104mg, 0.65ml Subcutaneously
- Noristerat (Norethisterone) 200mg every 8 weeks for 24 weeks, then every 12 weeks.
- Norigynon/Mesigyna (50 mg norethindrone enanthate plus 5 mg estradiol valerate) ; Both given monthly.
These contraceptives contain a single type of hormone, progestin.

Depo Provera
Depo Provera is a hormone used for contraception. It is given by injection and its effects will last for three months at a time.
Mode of Action
- Inhibits ovulation.
- Thickens cervical mucus, hindering sperm entry.
- Thins the uterine lining, reducing chances of fertilized egg implantation.
Indications
- Breastfeeding mothers after 6 weeks or immediately if not breastfeeding.
- Women needing long-term contraception.
- Known/suspected HIV-positive women.
- Women with sickle cell disease.
- Women unable to use COC due to oestrogen content.
- Women awaiting surgical contraception.
Advantages
- Very effective.
- Does not suppress lactation.
- Easy to remember return dates.
- Private usage.
- No oestrogen-related side effects.
- Reduces sickle cell crisis frequency.
- Non-interference with sex.
Disadvantages
- Changes in menstrual bleeding.
- Spotting (common in the first 3 months).
- Amenorrhea (common after 1st injection and after 9-12 months).
- Prolonged heavy vaginal bleeding.
- Weight changes.
- Irreversible injection.
- Delayed return of fertility.
- Loss of libido.
- Does not protect against STIs/HIV/AIDS.
Management
- Depo Provera 150mg deep IM into deltoid or buttock muscle.
- No rubbing to avoid increased absorption.
- Advise abstinence or backup FP method for the first 7 days after injection.
- Return for the next dose 12 weeks after the injection.

Sayana Press
Sayana Press is a contraceptive injection that women can give to themselves to prevent pregnancy. It’s given under the skin, at the front upper thighs or abdomen. The injection releases medication that runs through your bloodstream over a period of 13 weeks.
- Sayana press ® is a single-dose container with 104 mg Medroxyprogesterone acetate (MPA) in 0.65ml suspension (104mg) formulated for subcutaneous.
- It is administered subcutaneously into the anterior thigh or abdomen or arm.
- The efficacy of Sayana press depends on adherence to the recommended dosage schedule of administration.
Composition
- Single-dose container with 104 mg Medroxyprogesterone acetate (MPA) in 0.65ml suspension.
Administration
- Subcutaneously into the anterior thigh, abdomen, or arm
Mechanism of Action
- Suppresses ovulation.
- Renders endometrium unsuitable for implantation.
- Increases cervical mucus viscosity, impeding sperm penetration.
Indications
Nearly all women can use it safely & effectively including women:-
- Women whose partners have undergone vasectomy until vasectomy is effective.
- Have or have not had children.
- Any age including adolescents & women over 40 years old.
- Have just had an abortion/miscarriage.
- Breastfeeding women 6 weeks postpartum.
- HIV infected whether or not on ART.
Advantages and Non contraceptive benefits.
- New formulation for S/C injection.
- 30% low side effects compared to Depo-Provera.
- Do not interfere with sex.
- Private & no one else can tell that a woman is using it.
- May help women gain weight.
- Do not require daily action.
- Prevents pregnancy.
- Protects against endometrial cancer, uterine fibroids.
- Reduces sickle cell crisis among women with sickle cell anaemia.
- Protects against symptomatic PID & iron deficiency anaemia.
Disadvantages
- Weight changes.
- No protection against STIs/HIV/AIDS.
- Delayed fertility return.
- Potential side effects like hypersensitivity reactions, decreased/increased appetite, loss of libido, dizziness, headache, and more.
Problems that may need medical attention
- Loss of bone mineral density.
- Menstrual irregularities.
- Thromboembolic disorders.
- Anaphylaxis & anaphylactoid reactions.
- Sudden partial or complete loss of vision.
Disadvantages & Side effects
- Weight gain or loss
- Does not protect against STI/HIV/AIDs
- Delayed fertility return
- Hypersensitivity reactions
- Decreased/increased appetite
- Loss of libido & irritability
- Dizziness, headache & migraine
- Thromboembolic disorders
- Nausea & vomiting
- Jaundice
- Alopecia & urticaria
- Loss of bone mineral density
- Back & leg pains
- Mood changes
- Abdominal bloating & discomfort
