
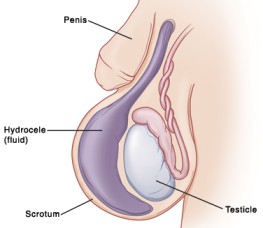

CLASSIFICATIONS OF HYDROCELES
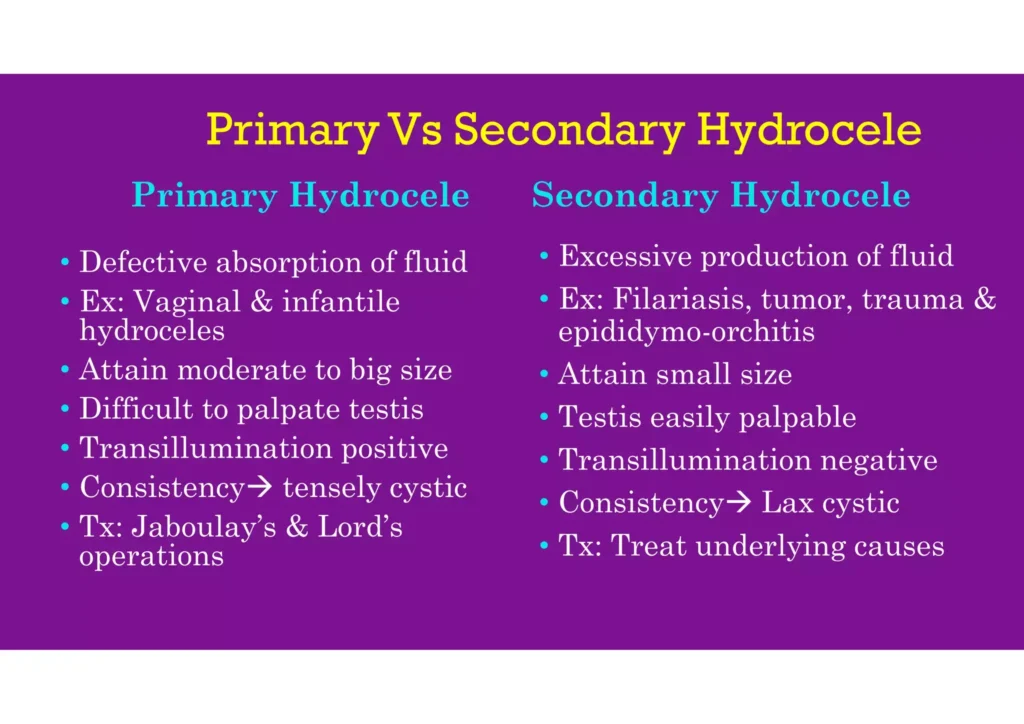
Primary hydrocele: A primary hydrocele is characterized by a soft, painless swelling that is usually large in size and makes it difficult to feel the testis. Transillumination can demonstrate the presence of fluid. Although these hydroceles are often asymptomatic, their large size can cause inconvenience and, if left untreated, may lead to atrophy of the testis due to compression or obstruction of blood supply. Early diagnosis during a complete physical examination may reveal small hydroceles in which the testis can be easily palpated within a lax hydrocele. However, in cases where the hydrocele sac is dense, ultrasound imaging is necessary to visualize the testis and reveal any underlying abnormalities. Primary hydroceles are usually painless, similar to testicular tumors.
A common method of diagnosing a primary hydrocele is through transillumination, where shining a strong light through the enlarged scrotum will pass light in the case of a primary hydrocele, while a tumor will not, except in the case of a malignancy with reactive hydrocele.
Its subdivided into four types.
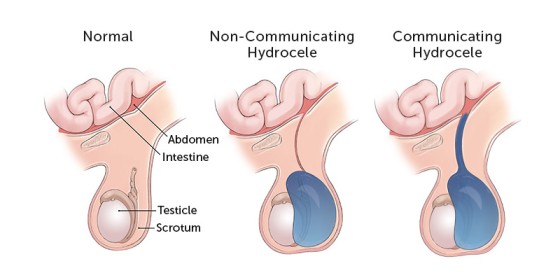
Congenital Hydrocele:
- Occurs when the processus vaginalis, a tube-like structure connecting the abdomen to the scrotum, remains open and communicates with the peritoneal cavity.
- This allows peritoneal fluid to move, but the opening is usually too small to allow intra-abdominal contents to herniate through.
- When pressure is applied to the hydrocele, it usually does not empty, but the fluid may drain into the peritoneal cavity when the individual is lying down.
- The swelling cannot be felt above the inguinal ring, resembling a hernia.
Infantile Hydrocele:
- Occurs when the processus vaginalis becomes closed at the level of the deep inguinal ring, but the portion beyond it remains open, allowing fluid to accumulate.
- This condition is not exclusive to infants and can also occur in adults.
- The swelling cannot be felt above the inguinal ring.
Encysted Hydrocele of the Cord:
- In this type, both the proximal and distal portions of the processus vaginalis become closed off, while the central portion remains open, leading to the accumulation of fluid within it.
- This results in a smooth oval swelling near the spermatic cord, which can be mistaken for an inguinal hernia.
- When the testis is gently pulled downwards, the swelling moves downwards and becomes less mobile.
Vaginal Hydrocele (in females):
- In females, a related condition known as a “hydrocele of the canal of Nuck” can occur.
- This occurs when the canal of Nuck, the equivalent structure to the processus vaginalis in males, fails to close properly, leading to the development of a hydrocele.
- This condition may present as a swelling in the groin or labia majora.
Secondary hydrocele: A secondary hydrocele arises from an underlying condition, such as infections (e.g., filariasis, tuberculosis of the epididymis, syphilis), trauma or injury (e.g., post herniorrhaphy hydrocele or malignancy).
- Secondary hydroceles are generally smaller, with the exception of those caused by filariasis, which can lead to very large hydroceles.
- Testicular infarction, microlithiasis of the testicle, and lithiasis of tunica vaginalis can also contribute to the development of secondary hydroceles.
- Testicular diseases, including cancer, trauma (e.g., hernia), and orchitis (inflammation of the testis), can result in secondary hydroceles. They may also occur in infants undergoing peritoneal dialysis. It is important to note that a hydrocele is not a cancerous condition, but clinical evaluation is needed if a testicular tumor is suspected, as there are no documented cases associating hydroceles with testicular cancer in the world literature.
Secondary hydroceles are most commonly linked with acute or chronic epididymo-orchitis and are also observed with testicular torsion and certain testicular tumors. Commonly, a secondary hydrocele is soft and moderately sized, and the underlying testis can be felt. The secondary hydrocele usually resolves when the primary condition is treated.
Other predisposing factors for secondary hydroceles include acute/chronic epididymo-orchitis, testicular torsion, testicular tumors, hematocele, filarial hydrocele, post herniorrhaphy, and hydrocele of a herniated sac.

Thank you so much for this great help of questions, notes and everything.
Understandable
Am greatful
Thank you very much this topic is very enjoyable
thanks bro
for the great work done