
A Mass Casualty Incident refers to an event that results in a large number of injured individuals requiring medical attention, while there is a shortage of medical personnel to provide the necessary services.
Imagine a bus accident on the Kampala-Jinja highway. Normally, a hospital emergency department might see 5 patients in one hour. But after this bus accident, 50 injured people arrive at once. The hospital has only 3 doctors and 5 nurses on duty. The number of patients is much greater than the hospital's ability to treat them all immediately. This is a Mass Casualty Incident.
| Feature | Explanation |
|---|---|
| Many casualties | Large number of injured or sick people at once |
| Limited resources | Not enough doctors, nurses, beds, or equipment |
| Overwhelms normal capacity | The hospital cannot function in its usual way |
| Requires special organization | Normal routines must change |
Mass Casualty Management involves providing on-the-spot medical care to a significant number of injured victims when there are limited medical resources available.
It is the organized way of handling many injured people with the few resources you have. Instead of treating one patient until they are fully stable (as in normal times), you must treat many patients just enough to keep them alive until more help arrives.
Casualty Management involves providing immediate care to victims during a disaster, including:
- Rescue operations
- Emergency medical care
- Evacuation of trapped individuals
Important Note: Triage plays a crucial role in determining the needs of injured victims during casualty management.
| Normal Emergency | Mass Casualty Incident |
|---|---|
| Number of patients matches hospital capacity | Number of patients exceeds hospital capacity |
| Standard treatment for each patient | Modified treatment: "Do the most for the most" |
| One doctor per patient | One doctor for many patients |
| All patients receive full care immediately | Some patients must wait; priority goes to those who can survive |
| Normal hospital routines continue | Normal routines are suspended |
| Example: One boda-boda accident victim | Example: Bus crash with 40 injured people |
| Cause | Example |
|---|---|
| Road traffic accidents | Bus or taxi crash on highways (Kampala-Jinja, Kampala-Masaka) |
| Boda-boda accidents | Multiple riders colliding at an intersection |
| Building collapse | School or market building falling down |
| Fires | Market fire, school dormitory fire |
| Terrorist attacks | Bombings (e.g., 2010 Kampala World Cup bombings) |
| Landslides | Multiple people injured in Bududa |
| Disease outbreaks | Many people sick at once (cholera, Ebola) |
| Industrial accidents | Factory explosion or chemical spill |
| Stampedes | Crowd crush at religious or political events |
Triage is the process of sorting or categorizing victims during a disaster to maximize the number of survivors by prioritizing treatment for those who are most likely to benefit.
Triage means "sorting" or "choosing who to treat first." In normal times, the sickest person gets treated first. In a mass casualty, the person who is most likely to survive with immediate help gets treated first. The goal is to save the maximum number of lives, not to save one person while ten others die waiting.
"Triage" comes from the French word "trier" meaning "to sort" or "to select." It was first used in wartime medicine.
The goal of triage is to:
- Identify which patients require immediate treatment
- Prioritize their care based on survival chances and resource availability
Sorting is done at:
| Location | When |
|---|---|
| The site of the disaster | If a medical team is already present (e.g., ambulance crew, community health workers) |
| Reception center | Upon arrival at a designated collection point |
| Hospital entrance/emergency department | When patients arrive at the hospital |
| At every stage of transport | Re-triage happens when patients move from scene to ambulance to hospital to ward |
🔑 Key Point: Triage is not a one-time event. It happens at every step of the journey from the disaster scene to the hospital.
In a mass casualty incident:
- Approximately 60% of casualties require medical intervention (surgery, advanced treatment, hospitalization)
- Approximately 40% may only need first aid and follow-up care (minor wounds, reassurance, observation)
Knowing this helps nurses prepare:
- If 100 patients arrive, expect about 60 who need serious care and 40 who need minor care
- The 40% who need first aid only can sometimes help care for the more serious 60%
Triage uses colors to quickly identify priority. Every nurse must know these colors by heart.
| Icon | Triage Color Codes |
|---|---|
| 🔴 | RED = Most Urgent / Immediate |
| 🟡 | YELLOW = Urgent / Delayed |
| 🟢 | GREEN = Minor / Walking Wounded |
| ⚫ | BLACK = Dying or Dead / Expectant |
These patients have life-threatening injuries but can survive IF they receive immediate treatment. They need care within minutes to hours.
- Injuries are serious but treatable
- Patient has a good chance of survival with rapid intervention
- Without treatment, they will die quickly
| Injury | Why It is RED |
|---|---|
| Airway obstruction | Cannot breathe; death in minutes |
| Severe bleeding (hemorrhage) | Losing blood fast; shock and death |
| Shock | Blood pressure dropping; organs failing |
| Chest wounds (sucking chest wound) | Lung collapsed; cannot breathe |
| Severe head injuries with altered consciousness | Brain swelling; needs immediate surgery |
| Burns 20-60% of body surface | Massive fluid loss; risk of shock |
| Severe abdominal injuries | Internal bleeding; needs surgery |
| Open fractures with severe bleeding | Blood loss plus risk of infection |
| Amputations with bleeding | Life-threatening blood loss |
- Immediate airway management: Open airway, suction, intubate if possible
- Control bleeding: Direct pressure, tourniquet if needed
- Start IV fluids: Two large-bore cannulas if possible
- Oxygen: High-flow oxygen
- Rapid transport to resuscitation area or operating theater
- Do NOT let them wait
These patients have serious injuries but are stable enough to wait for a short time. They need treatment within 2-4 hours.
- Injuries are serious but not immediately life-threatening
- Patient is stable for now
- Can wait while RED patients are treated
- Will become RED if left too long
| Injury | Why It is YELLOW |
|---|---|
| Multiple fractures (closed, not bleeding heavily) | Painful and disabling but not immediately fatal |
| Open fractures (without severe bleeding) | Risk of infection; needs surgery but can wait briefly |
| Spine injuries (stable patient) | Risk of paralysis; needs careful handling |
| Major burns less than 20% | Painful; needs dressing but not immediately life-threatening |
| Deep wounds (not bleeding heavily) | Needs cleaning and stitching |
| Eye injuries | Vision at risk; needs specialist care soon |
| Chest injuries (stable breathing) | Rib fractures, minor lung contusions |
| Abdominal injuries (stable vital signs) | Possible internal injury; needs investigation |
- Immobilize fractures: Splint, cervical collar, backboard if spinal injury suspected
- Dress wounds: Clean and cover to prevent infection
- Pain management: Give analgesics if available
- Monitor vital signs: Watch for deterioration to RED
- Keep comfortable: Blankets, reassurance
- Re-triage regularly: Check if condition worsens
These patients have non-life-threatening injuries. They can wait more than two hours for treatment. They are often called the "walking wounded" because they can walk and talk.
- Injuries are minor
- Patient is conscious and stable
- Can care for themselves or help others
- Lowest priority for immediate medical care
| Injury | Why It is GREEN |
|---|---|
| Simple fractures (finger, toe, minor arm) | Painful but not dangerous |
| Minor burns (small area, superficial) | First aid sufficient |
| Sprains and strains | Painful but not life-threatening |
| Small cuts and abrasions | Minor first aid |
| Minor head injuries (alert, no vomiting) | Observation needed but not urgent |
| Emotional distress (no physical injury) | Psychological support |
| Walking wounded: can move and communicate | They can wait and even help |
- First aid: Clean wounds, apply bandages
- Register: Keep records for follow-up
- Observation area: Place in designated waiting area
- Self-care instructions: Teach home care if appropriate
- Use as helpers: They can assist with moving patients, comforting children, or translating
- Re-triage: Check periodically in case hidden injuries appear
In a disaster, triage must prioritize the chances of survival. Victims in this category are beyond help with the available resources. They are either already dead or so severely injured that they will die despite treatment.
Important Ethical Note: This is the hardest category for nurses. It feels wrong to "give up" on a patient. But in a mass casualty, treating one person who will die anyway might mean letting three others (who could survive) die without care. The goal is to save the maximum number of lives.
| Condition | Why It is BLACK |
|---|---|
| No pulse, no breathing, no response (dead) | Resuscitation would waste resources |
| Severe head injury with no brain function | Not survivable in mass casualty setting |
| Severe burns over 80-90% of body | Survival extremely unlikely |
| Massive crush injuries with no vital signs | Too severe to treat with limited resources |
| Multiple traumatic amputations with shock | Unsurvivable without massive resources |
| Penetrating injury to heart with no signs of life | Immediate death |
- Make comfortable: Pain relief if possible (morphine if available)
- Do not abandon: Stay with them; hold their hand; speak gently
- Do not use scarce resources: No IV fluids, no CPR, no surgery
- Protect dignity: Cover with blanket; shield from public view
- Document: Record identity if possible; note time of death
- Support family: When family arrives, give them quiet space and compassion
- Psychological support: For yourself and other staff; this is emotionally difficult
In a real disaster, patients are marked with colored:
- Tags: Plastic or cardboard cards attached to wrist or neck
- Ribbons: Colored tape or cloth tied to patient
- Tape: Colored medical tape on forehead or limb
- Chalk: In very low-resource settings, colored chalk marks on forehead
A good triage tag should show:
- Color category (Red, Yellow, Green, Black)
- Patient name (if known)
- Age and sex
- Time of triage
- Injuries found
- Treatment given
- Vital signs
- Name of triage officer
| Principle | Explanation |
|---|---|
| Rapid | Each patient should be assessed in 30-60 seconds |
| Simple | Use basic observations (breathing, pulse, consciousness, bleeding) |
| Repeatable | Re-triage frequently; conditions change |
| Transparent | Document why each color was chosen |
| Dynamic | Categories can change: a Yellow can become Red |
| Resource-based | The same injury might be Red in a small clinic but Yellow in a major hospital |
Various personnel are involved in triage operations:
| Personnel | Role |
|---|---|
| Nurses | Often the primary triage officers at hospital entrance |
| Midwives | Triage in maternity and reproductive health emergencies |
| Allied health workers (Clinical officers, paramedics, EMTs) | Triage at scene and during transport |
| Physicians | Provide emergency care to critically injured; may supervise triage |
| Community health workers | Initial sorting in remote areas before transport |
🔑 Key Point: In a major disaster, nurses often assume roles normally done by doctors because there are not enough doctors. A nurse may need to start IV fluids, give emergency medications, or intubate if trained.
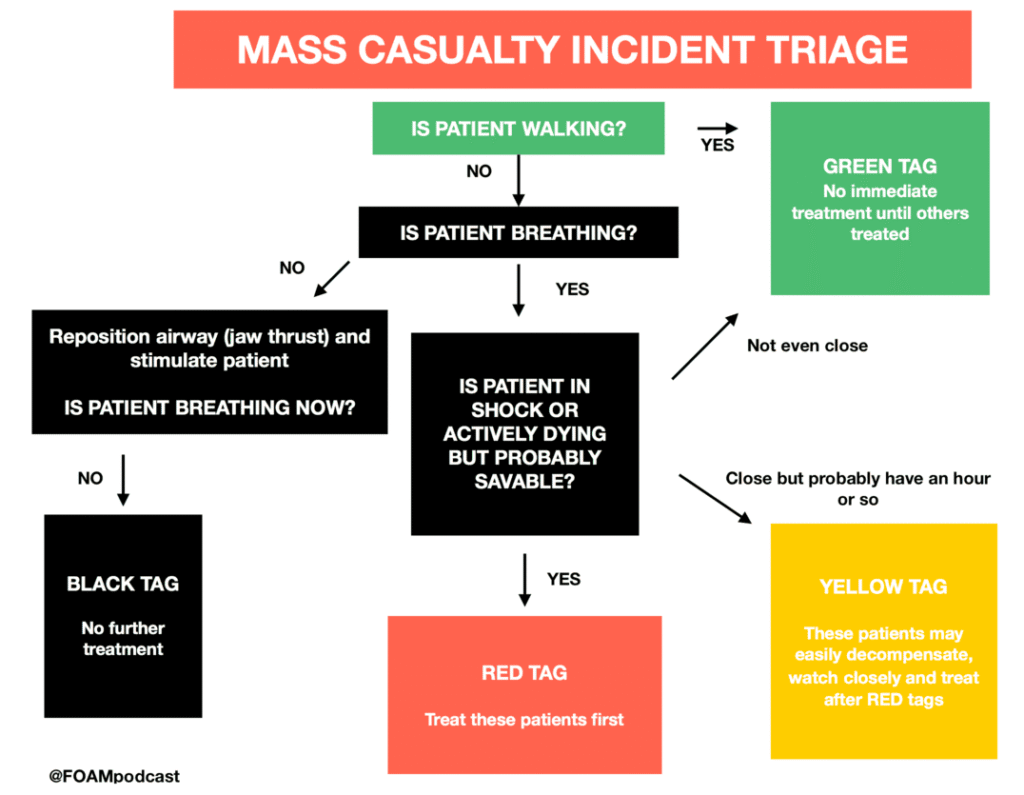
- Step 1: Call Out: Ask all patients who can walk to come to one area (GREEN collection point)
- Step 2: Assess the Remaining: For patients who cannot walk, quickly assess each one:
- Can they breathe? If no, open airway. If still no, BLACK
- Is breathing present? If yes, check rate. If very fast or very slow, RED
- Is there severe bleeding? If yes, RED
- Are they conscious? If no response, check pulse. If no pulse, BLACK
- Can they follow commands? If yes, check for major injuries
- Assign color based on findings
- Step 3: Tag and Move: Tag the patient with the appropriate color and move to the corresponding area:
- RED → Resuscitation area
- YELLOW → Treatment/waiting area
- GREEN → Minor injuries area
- BLACK → Morgue or quiet separate area
- Step 4: Re-triage: Reassess every 15-30 minutes. A patient's condition can improve or worsen.
- Children compensate well initially then crash suddenly
- A child who looks okay but is very quiet may be sicker than a crying child
- Use pediatric triage tape (measures height to estimate weight and vital signs)
- Always consider TWO patients (mother and baby)
- Pregnant women have extra blood volume: they may not show shock until very late
- Priority may need to be higher than the injury alone suggests
- May have silent heart attacks or strokes triggered by trauma
- Medications (blood thinners) can make bleeding worse
- Frailty means slower recovery
Every hospital should have a Mass Casualty Management Committee to ensure the hospital is ready before disaster strikes. This committee prepares the hospital's plan so that when 50 patients arrive at once, the hospital does not panic.
The committee should include members from:
| Department/Area | Why They Are Needed |
|---|---|
| Medical administration | Doctors who make clinical decisions and coordinate care |
| Hospital administration | Managers who allocate resources, space, and staff |
| Maintenance/Engineering | Ensure electricity, water, generators, and equipment work |
| Emergency department | Frontline responders who receive the first wave of patients |
| Surgical department | Surgeons who will operate on the most serious cases |
| Nursing services | Nurses who provide the majority of patient care |
- Pharmacy: Drug supply and management
- Laboratory: Blood tests and cross-matching
- Radiology: X-rays and imaging
- Security: Crowd control and safety
- Mortuary: Body handling
- Public relations/Media liaison: Information to families and press
- Chaplaincy/Social work: Psychological and spiritual support
| Function | Details |
|---|---|
| Preparing the hospital's contingency plan | Writing the disaster response plan specific to that hospital |
| Coordinating with other hospitals | Knowing which hospital can take overflow patients |
| Coordinating with relevant institutions | Police, fire brigade, ambulance services, Red Cross |
| Disseminating information | Sharing the plan with all staff; updating regularly |
| Conducting staff training | Regular drills and education sessions |
| Resource inventory | Knowing what supplies are available and where |
| Evaluating after events: After-action review | Learning lessons from every drill and real event |
The hospital receives warning that a mass casualty incident may occur or has occurred. Examples:
- Police radio that a bus has crashed with many injured
- Weather warning of an impending cyclone
- Notification of a bombing in the city
| Action | Who Does It |
|---|---|
| Activate the disaster plan | Hospital administrator or senior doctor on duty |
| Call in off-duty staff | Nursing supervisor contacts all available nurses |
| Clear emergency department | Move current non-critical patients to wards or home |
| Prepare supplies | Pharmacy opens emergency stock; theater prepares |
| Set up triage area | Designate space outside emergency department |
| Notify all departments | Call surgery, ICU, blood bank, laboratory, radiology |
| Prepare mortuary | Notify mortuary staff; prepare space |
| Set up communication center | Designate one person to receive and give information |
Patients begin arriving. All portions of the plan are implemented. The hospital shifts from normal operations to disaster mode.
| Action | Details |
|---|---|
| Triage at entrance | Sort patients before they enter the building |
| Direct to appropriate areas | Red to resuscitation, Yellow to treatment, Green to minor injuries, Black to separate area |
| Activate all teams | Surgery, anesthesia, nursing, support staff all working |
| Communicate continuously | Update on number of patients, resources needed |
| Request external help | Call other hospitals, NGOs, Ministry of Health if overwhelmed |
Signposts are clear signs posted at strategic locations in the hospital indicating:
- Evacuation routes: How to get out safely if the hospital itself is threatened
- Triage areas: Where patients should be directed
- Emergency exits: Alternative ways out
- Assembly points: Where staff and patients gather after evacuation
- In a disaster, people panic and forget directions
- New staff or volunteers may not know the hospital layout
- Patients and families need clear guidance
- In case of fire or structural damage, evacuation must be fast
The Incoming Patient Area is typically the casualty/emergency department of the hospital. However, during a mass casualty incident, this area may be extended to accommodate a larger number of patients.
- Tents outside the emergency department
- Nearby wards converted to emergency receiving areas
- Parking lot used for triage (in extreme cases)
- Schools or community halls nearby used as overflow (if hospital is full)
During a mass casualty, the emergency department is divided into specific functional areas:
- Location: At the entrance or just outside the emergency department
- Purpose: First point of contact; patients are sorted by color
- Staff: Triage nurse, triage officer
- Equipment: Tags, colored tape, stretchers, megaphone, clipboard
- Location: Inside emergency department or adjacent rooms
- Purpose: For RED tag patients — unstable, life-threatening conditions
- Features: Multiple beds or mats close together, Oxygen supply, Suction machines, IV fluid stocks, Emergency drugs, Monitoring equipment
- Staff: Senior doctors, anesthetists, senior nurses
- Location: Quiet, separate area away from main activity
- Purpose: For BLACK tag patients who are dying
- Features: Privacy, Dim lighting if possible, Pain relief medications available, Not visible to other patients or families initially
- Staff: Nurse assigned to comfort care; chaplain if available
- Location: Near mortuary or separate room
- Purpose: For patients who are already dead on arrival
- Features: Body bags or clean sheets, Identification tags, Security to prevent unauthorized entry, Refrigeration if available
- Staff: Mortuary attendant, police for identification
- Location: Large hall or waiting area
- Purpose: For GREEN tag patients
- Features: Chairs or mats, First aid supplies, Registration desk, Water and basic comfort items
- Staff: Junior nurses, medical students, volunteers
- Location: Nearby wards, clinic buildings, or tents
- Purpose: Overflow when emergency department is full
- Features: Basic monitoring capability, Beds or mattresses on floor, IV poles, oxygen if possible
- Staff: Nurses reassigned from less critical wards
- Location: Recovery area or ICU overflow
- Purpose: For patients who have had emergency surgery
- Features: Monitoring equipment, Oxygen, Pain management, Nursing observation
- Staff: Recovery nurses, anesthetists
During a mass casualty incident, normal standards of care must be modified. This is difficult for nurses because we are trained to give perfect care to every patient. But in an MCI, the goal changes.
"Do the greatest good for the greatest number"
Instead of perfect care for one patient, we give adequate care to many patients.
- Nurses may assume physician roles
- A nurse may need to intubate a patient (if trained)
- A nurse may need to declare death
- A nurse may need to make triage decisions normally made by doctors
- Physicians may work outside their specialty
- A gynecologist may need to treat trauma
- A pediatrician may need to treat adults
- Everyone does what they can
- Credentialing means officially approving someone to do a certain job
- In a disaster, providers may be granted credentials on an emergency or temporary basis
- A nurse may be authorized to give medications normally restricted to doctors
- A clinical officer may be authorized to perform minor surgery
- Disposable supplies may be reused due to resource limitations
- Gloves may be washed and reused (if no other option)
- Syringes may be sterilized and reused (extreme shortage only)
- Dressings may be washed and re-sterilized
⚠️ Note: This is not ideal and increases infection risk, but in a major disaster with no supplies, it may be necessary.
- Laboratory and radiology resources may be exhausted or overwhelmed
- Providers must make treatment decisions based on clinical judgment instead of tests
- A doctor may operate based on physical examination alone because X-ray machines are broken or too busy
- A nurse may give blood based on clinical signs of shock instead of waiting for lab results
| Challenge | Explanation |
|---|---|
| Withholding care from the dying | Black tag patients are not treated: this feels wrong but saves others |
| Rationing supplies | Deciding who gets the last bag of blood or the last oxygen tank |
| Breaking normal rules | Reusing disposables, practicing outside scope: necessary but uncomfortable |
| Telling families their loved one is not a priority | Explaining why a severely injured relative is not receiving surgery |
| Staff safety vs. patient need | Nurses working without adequate PPE because patients need help |
- Remember the goal: save the most lives possible
- Debrief after the event: talk about difficult decisions
- Seek psychological support
- Know that modified standards are temporary and necessary
Nurses must immediately know:
- How many medical-surgical beds are available
- How many ICU beds are available
- How many isolation beds are available (for infectious disease MCIs)
If 20 RED tag patients need admission but only 5 ICU beds exist, the nurse must know this immediately. Decisions about who gets a bed must be made quickly, and overflow areas must be prepared.
- Review all current in-patients
- Identify patients who can safely go home early to free up beds
- Examples:
- A patient recovering from malaria who is stable
- A mother who delivered yesterday and is doing well
- A patient on oral medications who can continue at home
- Work with doctors to review charts quickly
- Explain to patients and families why they must leave
- Give clear discharge instructions and medications
- Arrange follow-up
- Call in off-duty nurses: have a phone tree ready
- Recall retired nurses if needed
- Use student nurses and nursing assistants for non-critical tasks
- Assign specific roles: do not let everyone crowd around one patient
- Open emergency stockpiles
- Request supplies from: Pharmacy, Central medical stores, Other hospitals, NGOs (Red Cross, UNICEF)
- Prioritize scarce items: IV fluids, Blood, Oxygen, Sutures and dressings, Pain medications
- First person patients meet
- Rapid assessment (30-60 seconds per patient)
- Assigns color tag
- Directs patient to correct area
- Works in RED area
- Manages airways
- Starts IV lines
- Controls bleeding
- Prepares patients for surgery
- Monitors vital signs continuously
- Works in YELLOW area
- Dresses wounds
- Immobilizes fractures
- Administers medications
- Monitors for deterioration to RED
- Works in GREEN area
- Provides first aid
- Registers patients
- Gives self-care instructions
- Organizes helpers
- Works with BLACK tag patients
- Provides pain relief
- Offers emotional support
- Protects dignity
- Supports families
- Moves between areas
- Brings supplies
- Transports patients
- Communicates messages
- Relieves other nurses for breaks
- Records all patient information
- Maintains triage tags
- Tracks admissions and discharges
- Records deaths
- Essential for legal and follow-up purposes
- Ensures hand hygiene despite rush
- Manages waste disposal
- Oversees cleaning of areas
- Protects staff and patients from disease
- Without communication, chaos happens
- Families need to know where their relatives are
- Other hospitals need to know if they should accept transfers
- The media needs accurate information to prevent panic
- Report to nursing supervisor every 15-30 minutes on patient numbers and needs
- Use clear, simple language: avoid medical jargon when talking to non-medical staff
- Write clearly on triage tags and charts
- Update family members when possible (designate one area for family inquiries)
- Do not spread rumors: Only share verified information
- Legal protection for the hospital and staff
- Identification of patients
- Tracking of treatments given
- Epidemiological data (how many injured, types of injuries)
- Billing and resource accounting (for NGO and government reimbursement)
- Family notification
- Patient identification (name, age, sex, address if known)
- Triage category and time
- Injuries found
- Vital signs
- Treatment given (medications, fluids, procedures)
- Name of care provider
- Outcome (admitted, discharged, transferred, died)
- Triage tags with checkboxes
- Tally sheets: Count of Red, Yellow, Green, Black
- Whiteboards: Visible tracking of bed availability
- Pre-printed forms: Fill-in-the-blank to save time
Nurses in an MCI are under extreme stress. They may feel:
- Overwhelmed
- Guilty (about patients they could not save)
- Angry (at the disaster, at lack of resources)
- Numb or detached
- Exhausted
| Strategy | How to Do It |
|---|---|
| Take short breaks | Even 5 minutes to drink water and breathe |
| Eat and hydrate | You cannot help others if you collapse |
| Buddy system | Pair with another nurse; check on each other |
| Accept help | Let volunteers and less critical staff assist |
| Focus on what you CAN do | Do not dwell on what you cannot |
| Debrief after | Talk about the experience with colleagues |
- Red: Rescue immediately
- Yellow: Yes, treat soon
- Green: Go wait / Good to help
- Black: Beyond help / Breathing stopped
- Simple
- Triage
- And
- Rapid
- Treatment
(This is an internationally recognized triage system: Simple Triage And Rapid Treatment)
- Respiration: Are they breathing?
- Perfusion: Do they have a pulse? Are they perfusing?
- Mental status: Are they conscious? Can they follow commands?
- Count beds
- Alert staff
- Review in-patients for discharge
- Ensure supplies
- Set up areas
- 60% need medical intervention
- 40% need first aid only
- "Sixty need surgery, Forty need first aid"
Q1: Define a Mass Casualty Incident.
Answer: An event that results in a large number of injured individuals requiring medical attention while there is a shortage of medical personnel to provide the necessary services.
Q2: What is the goal of triage in a mass casualty incident?
Answer: To identify which patients require immediate treatment and prioritize their care in order to maximize the number of survivors.
Q3: List the four triage categories with their colors and give one example of injuries in each.
Answer:
- Red (Immediate): Airway obstruction, severe bleeding, shock, chest wounds, burns 20-60%
- Yellow (Delayed): Multiple fractures, open fractures without severe bleeding, spine injuries, major burns <20%
- Green (Minor): Simple fractures, minor burns, sprains, small cuts, walking wounded
- Black (Expectant/Dead): No pulse or breathing, severe burns >80%, unsurvivable injuries
Q4: Where is triage conducted?
Answer: At the disaster site, at reception centers, upon arrival at the hospital, and at every stage of victim transport.
Q5: What is the 60/40 rule in mass casualty incidents?
Answer: Approximately 60% of casualties require medical intervention, while 40% may only need first aid and follow-up care.
Q6: List the members of a Mass Casualty Management Committee.
Answer: Medical administration, hospital administration, maintenance, emergency department, surgical department, and nursing services.
Q7: Describe the two phases of emergency management in MCI.
Answer: Phase I is the alert phase (warning received, plan activated, staff called, supplies prepared). Phase II is the actual occurrence (patients arrive, triage implemented, all plan portions activated).
Q8: List five areas that should be set up in the emergency department during a mass casualty.
Answer: Triage area, resuscitation area, area for patients beyond salvage, area for brought-in dead, area for walking wounded, alternate area for overcrowding, post-operative receiving area. (Any five)
Q9: How does patient care in casualty change during a mass casualty incident?
Answer: Nurses may assume physician roles; physicians may work outside specialty; disposable supplies may be reused; treatment decisions may be based on clinical judgment rather than laboratory or radiology results.
Q10: What are three nursing responsibilities when a mass casualty incident is declared?
Answer: Conduct an accurate bed count; coordinate with in-patient services to discharge non-critical patients; ensure availability of required staff and supplies.
A truck loses control at a busy intersection. Fifteen boda-boda riders and passengers are injured. They are brought to your health centre IV, which has 2 nurses, 1 clinical officer, and 10 beds.
- Is this an MCI for your facility? (Yes: 15 patients exceeds your capacity)
- How do you set up triage? (Use the entrance area; assign one nurse to triage while the other prepares supplies)
- What colors do you expect? (Multiple fractures = Yellow; head injuries = Red or Black; minor abrasions = Green)
- What is your first action? (Call for help: alert district hospital, call off-duty staff, activate contingency plan)
A dormitory at a boarding school catches fire at night. Thirty students are brought to the regional referral hospital with burns and smoke inhalation.
- What areas must the emergency department set up? (Triage at entrance, resuscitation for smoke inhalation and severe burns, minor burns area, expectant area for severe cases)
- Which patients get RED tags? (Airway compromise from smoke, burns 20-60%, shock)
- What supplies will run out first? (IV fluids, oxygen, burn dressings, pain medication)
- What is the nursing role in documentation? (Track all 30 students, note injuries, treatments, and which students have been reunited with parents)
An explosion at a busy market brings 50 casualties to Mulago Hospital. You are the triage nurse at the entrance.
- What is your triage system? (RPM: Respiration, Perfusion, Mental status; assign colors in 30 seconds per patient)
- How do you handle the walking wounded? (Direct them to the Green area; they can help with translation, comforting others, or moving supplies)
- What do you do with a patient who has no pulse and no breathing? (Tag BLACK; do not start CPR in an MCI with limited staff; cover and protect dignity)
- How do you prevent staff psychological trauma? (Rotate staff, ensure breaks, debrief after the event, provide counseling)
- An MCI occurs when patient numbers exceed available resources
- Triage is the key to saving the maximum number of lives
- The four colors are Red, Yellow, Green, and Black
- Triage happens at every stage: scene, transport, hospital entrance, treatment areas
- The 60/40 rule helps predict resource needs
- Every hospital needs a Mass Casualty Management Committee
- There are two phases: Alert and Actual Occurrence
- The emergency department must be divided into specific functional areas
- During MCI, normal care standards are modified: this is necessary and ethical
- Nurses have expanded roles and may perform tasks normally done by doctors
- Documentation remains essential even in chaos
- Nurses must care for themselves to continue caring for others
- World Health Organization (WHO). Mass casualty management systems: strategies and guidelines for building health sector capacity.
- Advanced Trauma Life Support (ATLS). American College of Surgeons. Guidelines on disaster management and triage.
- Ministry of Health, Uganda. National Guidelines for Disaster Risk Management in the Health Sector.
- Bledsoe, B. E., Porter, R. S., & Cherry, R. A. Paramedic Care: Principles & Practice. (Relevant chapters on MCI and Triage).
Quick Quiz
Mass Causality Incident Quiz
Disaster Management - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Mass Causality Incident Quiz
Disaster Management
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.