MANAGEMENT OF MENINGITIS.
Meningitis is a potentially life-threatening condition with a high mortality rate if left untreated. Prompt treatment is crucial, and a delay has been linked to a poorer outcome. The initial treatment involves promptly administering antibiotics and sometimes antiviral drugs. Corticosteroids may also be used to prevent complications from excessive inflammation.
Treatment with broad-spectrum antibiotics should not be delayed while confirmatory tests are being conducted. In cases where meningococcal disease is suspected, benzylpenicillin is recommended before transfer to a hospital. Intravenous fluids are administered if there is hypotension or shock, and admission to an intensive care unit may be necessary.
Aims of Management
- To minimize further complication.
- To relieve pain.
- To preserve life.
- To promote comfort
Immediate Intervention:
- The patient and relatives are received and admitted to the male medical ward in an isolation room with dim light, on a comfortable bed, and positioned for comfort.
- Quick assessment of the patient’s condition, including level of consciousness (using the Glasgow Coma Scale), and baseline observations (TPR/BP) are recorded.
- Relatives and the patient are reassured to alleviate anxiety.
- The doctor is informed about the patient’s condition.
Meanwhile;
In case of unconsciousness, oxygen administration is instituted.
An Intravenous (IV) line is established for fluid and drug administration, and a blood sample is taken for hematology.
The doctor may request for the following investigations;
- Cerebral Spinal Fluid analysis for quality, quantity, and nature.
- Chest x-ray and ultrasound to identify a possible primary site.
Continuous care
- Catheter insertion for monitoring urine output and fluid balance charting after 24 hours.
- Nasogastric tube insertion for nutritional support.
- Tepid sponging is performed to reduce fever and enhance patient comfort.
- Continuous monitoring of CSF for quality, quantity, and appearance.
- Collection, disinfection, and safe disposal of all patient discharges to prevent cross-infection.
Following Doctor’s Review and Prescription:
For Streptococcus pneumonia (10-14 day course; up to 21 days in severe cases):
- Benzyl penicillin 3-4 MU IV or IM every 4 hours
- Or Ceftriaxone 2 g IV or IM every 12 hours
For Haemophilus influenza (10-day course):
- Ceftriaxone 2 g IV or IM every 12 hours.
For Neisseria meningitides (up to 14-day course):
- Benzyl penicillin IV 5-6 MU every 6 hours
- Or Ceftriaxone 2 g IV or IM every 12 hours
- Or Chloramphenicol 1 g IV every 6 hours (IM if IV not possible)
For adults above 50 years:
- Cefotaxime 2g IV every 6 hours
- Or Ceftriaxone 2 g IV every 12 hours
- Or Co-trimoxazole 50mg/kg IV daily in 2 divided doses, plus Ampicillin 2g IV every 4 hours
- Or Co-trimoxazole 50mg/kg IV daily in 2 divided doses.
Meningitis is potentially life-threatening and has a high mortality rate if untreated; delay in treatment has been associated with a poorer outcome. The first treatment in acute meningitis consists of promptly giving antibiotics and sometimes antiviral drugs. Corticosteroids can also be used to prevent complications from excessive inflammation.
Thus, treatment with wide-spectrum antibiotics should not be delayed while confirmatory tests are being conducted. If meningococcal disease is suspected in primary care, guidelines recommend that benzylpenicillin be administered before transfer to hospital.
Continuous Nursing Care:
- Reassurance of the patient and relatives.
- Position change every 2 hours to prevent pressure sores and aspiration.
- Infusion site cleaning, bed baths, and regular oral care.
- Proper bed-making and changing of soiled linen.
- Ensuring a balanced diet.
- Encouraging patient exercises for healing.
- Providing a bedpan for bowel opening.
- Health education about meningitis, its causes, features, and prevention.
Specific Interventions:
Mechanical Ventilation: Required if the level of consciousness is very low or if respiratory failure is evident.
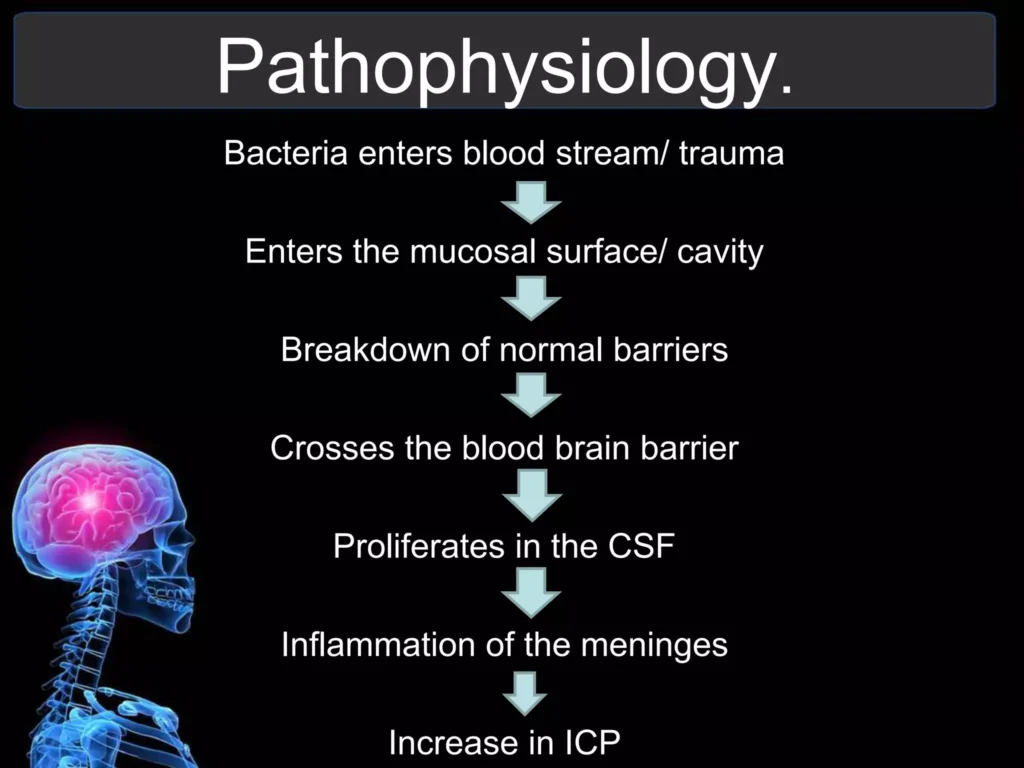
Raised Intracranial Pressure (ICP):
- Monitoring measures are taken to optimize cerebral perfusion pressure.
- Various treatments, including medication (e.g., mannitol), are used to decrease intracranial pressure.
Seizures: Treated with anticonvulsants.
- Hydrocephalus: May require the insertion of temporary or long-term drainage devices, such as a cerebral shunt.
Bacterial Meningitis:
- Antibiotics Used: Cefotaxime, vancomycin, chloramphenicol, and ampicillin can be used, sometimes in combination.
- Empirical Therapy: Based on age, history of head injury, recent neurosurgery, and the presence of a cerebral shunt. Ampicillin is recommended for young children, those over 50, and immunocompromised individuals to cover Listeria monocytogenes.
- Tuberculous Meningitis: Requires prolonged treatment with antibiotics (typically a year or longer).
Steroids:
- Additional treatment with corticosteroids (usually dexamethasone) shows benefits such as a reduction in hearing loss and better short-term neurological outcomes. Their role differs in children and adults.
Viral Meningitis:
- Usually requires supportive therapy.
- Antiviral drugs (e.g., aciclovir) may be used for herpes simplex virus and varicella-zoster virus.
- Mild cases can be treated at home with conservative measures.
Fungal Meningitis:
- Treated with long courses of high-dose antifungals (amphotericin B and flucytosine).
- Frequent lumbar punctures or lumbar drains may be needed to relieve raised intracranial pressure.
Note:
- Untreated bacterial meningitis is almost always fatal.
- Viral meningitis tends to resolve spontaneously and is rarely fatal.
- With treatment, mortality from bacterial meningitis depends on age and the underlying cause. Mortality rates are highest in newborns (20–30%) and adults (19–37%).




Thanks
Thank you!
thank you alot
Thanks
Detailed indeed
thank you so much
NICE
Short, pricise, full of knowledge and enjoyable to read!
nice one…thank you so much