

Adenoid hypertrophy is a condition characterized by enlarged adenoids, a collection of lymphatic tissue located at the back of the nasal cavity. This enlargement can lead to nasal obstruction, impacting breathing, sleep, and overall well-being.
- The adenoids, also known as the pharyngeal tonsils, are part of the body’s secondary immune system, acting as a first line of defense against infections.
- The anatomical position of the adenoids allows them to help fight infection by preventing germs from entering the body through the mouth or nose. They are involved in the production of mostly secretory IgA, which is transported to the surface providing local immune protection.
- Along with the tonsils, the adenoids form part of the lymphatic system, which works to defend the body against microbes, absorb nutrients, maintain proper fluid levels, and eliminate certain waste products.
- They are usually larger in children, playing a role in protecting them from respiratory infections. Lymphoid tissue of Waldeyer's ring is most immunologically active between 4 and 10 yr of age, with a decrease after puberty.
- By the age of five, adenoids usually begin to shrink, becoming less prominent in the immune system’s function.
- The lymphoid tissue of the nasopharynx and oropharynx is composed of the adenoids (pharyngeal tonsil), the tubal tonsils, the lateral bands, the palatine tonsils, and the lingual tonsils.
- These structures form an interrupted circle of protective lymphoid tissue at the upper ends of the respiratory and alimentary tracts named Waldeyer’s ring after the German anatomist who described them.
- The adenoids are small masses of lymphatic tissue located in the upper airway, between the nose and the back of the throat (upper midline in nasopharynx).
- The adenoid is a single mass of pyramidal tissue with its base on the posterior nasopharyngeal wall and its apex pointed toward the nasal septum.
- The surface is invaginated in a series of folds. The epithelium is pseudostratified ciliated epithelium and is infiltrated by the lymphoid follicle.
- The formation of the adenoids begins in the 3rd month of fetal development.
- In the 5th month: the pharyngeal crypts will develop. The surface is covered with pseudostratified ciliated epithelium.
- By the 7th month of development the adenoids are fully formed.
Adenoid enlargement can be attributed to various factors, peaking between 2 – 8 years. Common diseases of the tonsils and adenoids include acute adenoiditis/tonsillitis, recurrent/chronic adenoiditis/tonsillitis, obstructive hyperplasia, and malignancy.
- Infections: Viral infections, such as Epstein-Barr virus, and bacterial infections, like group A Streptococcus, can trigger inflammation and swelling of the adenoids. Most episodes of acute pharyngotonsillitis are caused by viruses.
- Chronic Inflammation: Repeated acute infections or persistent infections can lead to chronic adenoid inflammation, resulting in hypertrophy. The tonsils and adenoids can be chronically infected by multiple microbes.
- Allergy: Allergens or irritants, when exposed to the adenoid tissue, can trigger an inflammatory response, causing enlargement.
- Recurrent RTI: Recurrent respiratory tract infections.
- Genetics.
- Gastroesophageal Reflux (GERD): Stomach acid refluxing into the esophagus can irritate the adenoid tissue, leading to inflammation and hypertrophy.
Several aerobic and anaerobic bacterial species have been implicated in adenoid hypertrophy. Group A β-hemolytic streptococcus (GABHS) is the most common cause of bacterial infection in the pharynx. In chronic infections, there is a high incidence of β-lactamase–producing organisms.
- Alpha-, beta-, and gamma-hemolytic Streptococcus species
- Hemophilus influenzae
- Moraxella catarrhalis
- Staphylococcus aureus
- Neisseria gonorrhoeae
- Corynebacterium diphtheriae
- Chlamydophila pneumoniae
- Mycoplasma pneumoniae
- Anaerobic species, such as Peptostreptococcus predominate in chronic infections alongside aerobes.
| Grade | Description |
|---|---|
| Grade 1 | No contact between adenoid tissue and vomer, soft palate, or torus tubaris. |
| Grade 2 | Adenoid tissue contacts the torus tubaris. |
| Grade 3 | Adenoid tissue contacts the torus tubaris and vomer. |
| Grade 4 | Adenoid tissue contacts the torus tubaris, vomer, and soft palate in resting position. |

| Grade | Description |
|---|---|
| Grade 1 | Adenoid occupies less than 25% of the choanal area. |
| Grade 2 | Adenoid occupies 25-50% of the choanal area. |
| Grade 3 | Adenoid occupies 50-75% of the choanal area. |
| Grade 4 | Adenoid occupies 75-100% of the choanal area. |
Always think about details history of nasal obstruction, snoring, and nasal discharge.
- Grade 0: never seen
- Grade 1: seen during URTI
- Grade 2: frequently seen
- Grade 3: always occurs
The adenoids enlargement may cause acute adenoiditis, recurrent acute adenoiditis, chronic adenoiditis, and obstructive sleep apnea. The symptoms can vary depending on the severity of the condition.
- Nasal Obstruction: Difficulty breathing through the nose, leading to mouth breathing. Both the tonsils and adenoids are a major cause of upper airway obstruction in children.
- Mouth Breathing: Dry lips and bad breath due to continuous breathing through the mouth.
- Nasal Congestion: Feeling like the nose is pinched or stuffed.
- Frequent Sinus Symptoms: Recurrent sinus infections, headaches, and facial pain.
- Snoring: Loud snoring, especially during sleep.
- Acute Adenoiditis: Symptoms include purulent rhinorrhea, nasal obstruction, fever, and sometimes otitis media due to their proximity to the Eustachian tubes. The patient may also present with swallowing difficulties, speech anomalies (hyponasal speech), and sleep-disordered breathing. This can be difficult to differentiate from an acute upper respiratory infection but tends to have a longer and more severe course.
- Recurrent Acute Adenoiditis: 4 or more episodes of acute adenoiditis in a 6-month period with intervening periods of wellness.
- Chronic Adenoiditis / Obstructive Adenoid Hyperplasia: Symptoms include persistent rhinorrhea, chronic nasal obstruction, postnasal drip, malodorous breath, mouth breathing, hyponasal voice, and associated otitis media or extra esophageal reflux lasting at least 3 months.
- Obstructive Sleep Apnea (OSA): Airway obstruction in children is typically manifested in sleep-disordered breathing (including OSA, obstructive sleep hypopnea, and upper airway resistance syndrome which may cause growth failure). Clinically marked by loud snoring, apneic episodes while sleeping, daytime somnolence, behavioral problems, and enuresis.
- Tonsillar Neoplasm: Rapid enlargement of one tonsil is highly suggestive of a tonsillar malignancy, typically lymphoma in children.
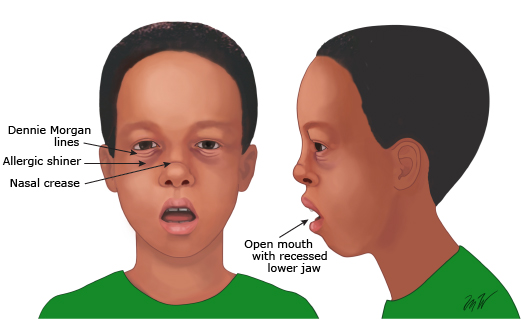
It is the long, open-mouthed, face of children with adenoid hypertrophy. The mouth is always open because upper airway congestion has made patients obligatory mouth breathers.
- Underdeveloped thin nostrils
- Short upper lip
- Prominent upper teeth
- Crowded teeth
- High-arched palate
- Hypoplastic maxilla
- Eustachian blockage causing glue ear-deafness
- The deafness and inattentiveness interferes with the learning
- Child grows with lowered intelligence and understanding
- Clinical / Physical Examination: History & clinical examination. Examine the nose and throat for signs of adenoid enlargement.
- Palpation: Gently feeling the adenoids through the roof of the mouth.
- Endoscopy / Rhinoscopy: A thin, flexible tube with a camera is inserted into the nose to visualize the adenoids. Transnasal Endoscopy is performed by an otolaryngologist for a definitive diagnosis.
- Radiological Examination (PNS) / Lateral Neck Radiograph: The main imaging study to evaluate the adenoid is a lateral neck radiograph. An X-ray of the neck can help visualize the size, shape, and airway narrowing caused by the adenoids.
- CT scan.
Adenoid tissue enlargement was graded according to the Adenoidal-nasopharyngeal ratios (ANR). The ANR was obtained by dividing the measurement for adenoid tissue density by the value for nasopharyngeal space in millimeters as described by Fujioka. It was rated regarding airway space as:
- Grade 1: > 6 mm
- Grade 2: 4-6 mm
- Grade 3: < 3 mm
Treatment for adenoid hypertrophy depends on the severity of the symptoms. Management options include waiting until they involute, non-surgical management (intranasal corticosteroids), or surgical removal (adenoidectomy).
- Wait until they involute: No treatment may be needed as adenoids naturally shrink over time.
- Chronic adenoiditis: No good evidence supports any curative medical therapy for chronic infection of the adenoids.
- Systemic antibiotics: Have been used long-term (ie, 6 weeks) for lymphoid tissue infection, but eradication of the bacteria failed. In fact, with the current trend of resistant bacteria, the use of prophylactic or long-term antibiotics has been decreased to prevent the formation of resistant bacteria. If the condition is an acute bacterial infection, short courses of antibiotics may be prescribed.
- Topical Nasal Steroids: Saline or steroid nasal sprays can help reduce swelling and improve breathing. Some studies indicate a benefit with using topical nasal steroids in children with adenoid hypertrophy.
- Studies indicate that while using the medication, the adenoid may shrink slightly, which may help relieve some nasal obstruction.
- However, once the topical nasal steroid is discontinued, the adenoid can again hypertrophy and continue to cause symptoms.
- In a child with nasal obstructive symptoms with or without presumed allergic rhinitis, a trial of topical nasal steroid spray and saline spray may be considered for effective control of symptoms.
- Mometasone furoate: intranasal spray 50 mcg – 100 mcg /day for 6 to 8 weeks for children more than 2 years.
- Fluticasone propionate: nasal spray of 400 microg/day for 8 weeks for children more than 4 years.
- Beclomethasone: intranasal spray 50 mcg /day for 8 weeks for children more than 3 years.
Evidences: Using nasal steroids to treat nasal obstruction caused by adenoid hypertrophy suggests significant improvement (up to 77.7% in some data sources). The improvement appears to be associated with a reduction of adenoid size. Maintenance therapy is often needed if symptom-relief is to persist.
Adenoidectomy: Surgical removal of the adenoids may be recommended if conservative measures are ineffective.
- Four or more episodes of recurrent purulent rhinorrhea in prior 12 months in a child <12 (documented by intranasal examination or diagnostic imaging).
- Persisting symptoms of chronic adenoiditis after 2 courses of antibiotic therapy.
- Sleep disturbance with nasal airway obstruction persisting for at least 3 months.
- Otitis media with effusion >3 months or second set of tubes (persistent Otitis media with effusion over age 4).
- Dental malocclusion or orofacial growth disturbance documented by orthodontist.
- Nasal speech.
- Cardiopulmonary complications including cor pulmonale, pulmonary hypertension, right ventricular hypertrophy associated with upper airway obstruction.
If adenoid hypertrophy is left untreated, it may cause many serious problems such as:
- Obstructive Sleep Apnea (OSA): Enlarged adenoids can block the airway during sleep, leading to frequent awakenings, daytime sleepiness, and other health issues.
- Chronic Otitis Media: The hypertrophied adenoids can block the Eustachian tube, leading to recurrent ear infections and fluid buildup in the middle ear.
- Recurrent Sinus Infections: Obstruction of the nasal passages can lead to frequent sinus infections.
- Mouth Breathing and Dental Issues: Continuous mouth breathing can cause dry mouth, bad breath, and dental malocclusions over time.
- Speech and Swallowing Problems: Enlarged adenoids can interfere with speech and swallowing, potentially causing nasal speech and difficulty swallowing.
- Failure to Thrive / Developmental Delay: In severe cases, the obstruction can lead to poor weight gain and growth in children.
- Cognitive and behavioral disorders.
- Systemic and pulmonary hypertension.
- Enuresis.
| No. | Nursing Diagnosis | Interventions & Rationale |
|---|---|---|
| 1 | Ineffective Airway Clearance related to adenoid hypertrophy, mechanical obstruction, and excessive secretions. |
|
| 2 | Risk for Bleeding (Post-Operative) related to surgical removal of highly vascular adenoid tissue. |
|
| 3 | Acute Pain related to surgical incision, inflammation, and throat irritation. |
|
| 4 | Impaired Swallowing / Risk for Deficient Fluid Volume related to throat pain post-surgery. |
|
- Explanation and Consent: Explain the surgery to the child (in age-appropriate terms) and the parents. Ensure written informed consent is obtained from the parents/guardians.
- Baseline Assessment & Labs: Record baseline vital signs. It is critical to review bleeding and coagulation profiles (PT, PTT, INR, platelet count) because the adenoid bed is highly vascular.
- Physical Examination: Check for any active upper respiratory infections (which may delay surgery) and assess for loose teeth (to prevent dislodgment and aspiration during intubation).
- NPO Status (Nil Per Os): Ensure the patient strictly follows fasting guidelines (typically 6-8 hours for food, 2 hours for clear liquids) to prevent aspiration pneumonia under anesthesia.
- Counseling and Reassurance: Provide emotional support to reduce anxiety for both the child and the parents. Address any questions about post-operative pain or bleeding.
- Preparation: Have the child void before administering any pre-medication. Remove any jewelry or obstacles. Establish an IV line for fluid and medication administration.
After surgery to remove the adenoids, nurses play a vital role in providing comprehensive care:
- Immediate Airway Management & Positioning: Place the patient in a lateral (side-lying) or prone position with the head turned to the side until fully awake. This prevents the aspiration of blood and secretions.
- Monitoring for Complications (Bleeding): This is the highest priority. Observe for signs of bleeding such as frequent swallowing, vomiting bright red blood, restlessness, tachycardia, or pallor. Note: some dark, old blood in the vomitus is normal immediately post-op.
- Respiratory Distress: Observe for signs of respiratory distress, stridor, or excessive snoring indicating severe airway edema.
- Pain Management: Administering pain medication (typically Acetaminophen) and providing comfort measures (like an ice collar). Avoid aspirin or ibuprofen which increase bleeding risk.
- Hydration and Nutrition: Encouraging fluid intake once the gag reflex returns and nausea subsides. Offer cold, clear liquids first. Avoid red/brown fluids, citrus, or hot liquids. Gradually advance to soft, easy-to-swallow foods.
- Rest and Recovery: Advise on adequate rest and gradual return to normal activities. Maintain a calm environment to prevent crying or agitation, which can increase blood pressure and precipitate bleeding at the surgical site.
- Activity Restrictions: Instruct parents to restrict vigorous physical activity, heavy lifting, and rough play for 1 to 2 weeks to prevent delayed hemorrhage.
- Dietary Guidelines: Continue a soft, cool, or room-temperature diet for several days. Avoid hard, crunchy, spicy, or acidic foods.
- Normal Post-Op Symptoms: Educate parents that foul-smelling breath, a low-grade fever, nasal congestion, and mild earache (referred pain from the throat) are common and expected during the healing process.
- Warning Signs to Report: Seek immediate emergency medical attention if there is any bright red bleeding from the mouth or nose, continuous swallowing, persistent high fever, or inability to take in fluids (risk of dehydration).
- Follow-up: Ensure a follow-up appointment is scheduled to evaluate the healing of the adenoid bed and the resolution of preoperative symptoms (like OSA or recurrent infections).