

Pain is an unpleasant experience that involves both physical sensations and emotions. It is often connected to actual or possible harm to body tissues. Pain is something we feel when our body is hurt, sick, or under threat.
"Pain is what the patient says hurts."
This means pain is subjective. Each person shapes their own understanding of pain based on their personal experiences, culture, fears, and beliefs. If a patient says they are in pain, they are in pain. As nurses, we must believe them.
"Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage."
What this means in simple words:
- Pain is not just a physical feeling. It is also an emotional experience.
- Pain can happen even when there is no visible injury (potential damage).
- The patient describes the pain in their own words, and we must accept that description.
"Pain is whatever the experiencing person says it is, existing whenever he says it does."
What this means for nurses:
- The patient is the expert on their own pain.
- We cannot measure pain with a thermometer or a blood test.
- We must ask the patient, listen to them, and believe them.
- Pain is the symptom that patients fear the most when they are nearing the end of life. It affects quality of life more than almost any other problem.
- Pain affects around 98% of cancer and HIV/AIDS patients in advanced stages.
- Cancer pain is typically constant and worsens as the disease progresses.
- In developing countries like Uganda, where less than 5% of cancer patients have access to chemotherapy or radiotherapy, pain tends to worsen gradually until death because the disease cannot be stopped by curative treatment.
A study conducted in Africa involving patients with Stage IV AIDS (the most advanced stage) identified the most common pains reported:
| Type of Pain | Percentage of Patients | Cause / Notes |
|---|---|---|
| Lower limb pain | 66% | Often caused by peripheral neuropathy (nerve damage), common in HIV/AIDS. |
| Mouth pain | 50.5% | Often from oral thrush, ulcers, or infections. |
| Headache | 42.3% | From infections like meningitis, or raised pressure in the skull. |
| Throat pain | 39.8% | From infections, difficulty swallowing, or esophageal thrush. |
| Chest pain | 17.5% | From lung infections, TB, or other chest problems. |
💡 Nursing Implication
In Uganda, where HIV/AIDS is a major cause of illness, nurses must be prepared to assess and manage these specific types of pain every day. Note that HIV-induced lower limb pain is heavily linked to viral damage of nerves and the toxic effects of older Anti-Retroviral (ARV) drugs like Stavudine (d4T).
Acute pain serves as a useful mechanism that alerts the body to the presence of harmful or potentially harmful stimuli in the environment, such as:
- Extreme heat (burning)
- Extreme cold (frostbite)
- Sharp objects (cuts)
- Disease or injury
Think of acute pain like a fire alarm. It warns us that something is wrong and needs attention.
In palliative care, pain is often chronic (long-lasting). It no longer serves as a useful warning. Instead, it becomes a problem itself that causes suffering and needs to be relieved.
Understanding how pain happens helps nurses understand why different medicines work in different ways.
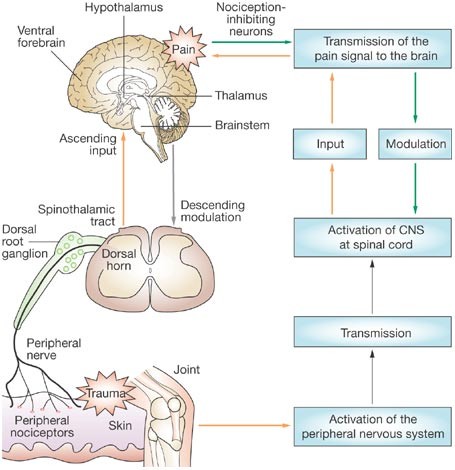
Pain travels through the body like a message passing through several stations:
- Pain begins when free nerve endings called nociceptors (pain sensors) are stimulated.
- These nociceptors are found in the skin, connective tissues, muscles, bones, and internal organs.
- They can be activated by:
- Physical stimuli: Pressure, heat, cold, cutting.
- Chemical stimuli: Chemicals released when tissues are injured or inflamed.
When tissues are injured, the body releases chemicals that activate the pain sensors. These include:
- Prostaglandins (cause inflammation and swelling)
- Bradykinin (dilates blood vessels and causes pain)
- Serotonin (affects mood and pain signaling)
- Histamine (causes itching and swelling)
- Potassium ions and Hydrogen ions (acidic environment around injury)
Pharmacology Expansion: This is why anti-inflammatory drugs like ibuprofen and diclofenac (NSAIDs) work — they directly inhibit the COX enzyme, stopping the production of prostaglandins right at the site of injury!
- The pain signal travels along peripheral nerves (nerves outside the brain and spinal cord) to the dorsal horn of the spinal cord.
- In the spinal cord, the signal crosses over to cells of the spinothalamic tract.
- These cells carry the impulses up the spinal cord, through the brain stem, to the thalamus (a relay station in the brain).
Pharmacology Expansion: Local anesthetics (like lidocaine) work by blocking the sodium channels along these peripheral nerves, stopping the "Transmission" phase entirely. Opioids (morphine) work primarily at the dorsal horn to stop the signal from ascending to the brain.
- From the thalamus, impulses are delivered to various areas of the cerebral cortex (the thinking and feeling part of the brain).
- The brain interprets the signal as pain and creates a reaction (pulling away, crying, guarding the area).
| Type | Location | What They Detect |
|---|---|---|
| Somatic nociceptors | Skin, muscles, bones, connective tissues | Pain from the surface and structure of the body. (Usually sharp, aching, easy to locate). |
| Visceral nociceptors | Internal organs (liver, stomach, intestines, etc.) | Pain from inside the body. (Usually dull, cramping, hard to locate). |
The concept of Total Pain was developed by Dame Cicely Saunders in the 1960s. She is the founder of the modern hospice movement.
Cicely Saunders taught that pain is not just a physical phenomenon. In palliative care, pain has four dimensions that are all connected and must all be addressed.
This is the actual bodily sensation of pain. It includes:
- The disease itself (tumor pressing on organs, bones, or nerves).
- Undesirable effects of treatment (surgery wounds, chemotherapy side effects, radiation burns).
- Insomnia (pain that stops sleep).
- Chronic fatigue (tiredness that never goes away).
- Other physical symptoms like nausea, constipation, or shortness of breath that make pain feel worse.
This is the emotional suffering that comes with illness. It includes:
- Anger at delays in diagnosis ("Why did the doctors not find this earlier?").
- Anger at treatment failure ("The medicine is not working!").
- Disfigurement (feeling ugly or ashamed because of weight loss, wounds, or surgery scars).
- Fear of pain ("Will it get worse?").
- Fear of death ("What will happen when I die?").
- Feelings of helplessness ("I cannot do anything for myself anymore").
- Anger at friends who do not visit ("Where is everyone now that I am sick?").
This is the suffering caused by changes in the patient's place in society and family. It includes:
- Worry about family ("Who will take care of my children?").
- Worry about finance ("We have no money for school fees or food").
- Loss of job (cannot work anymore).
- Loss of income (the family has no money because the breadwinner is sick).
- Loss of social position (people used to respect me, now they pity me or avoid me).
This is the suffering of the soul and spirit. It includes:
- "Why has this happened to me?" (searching for a reason).
- "Why does God allow me to suffer like this?" (feeling abandoned by God).
- "Is there any meaning or purpose in life?" (feeling that life has become meaningless).
- Guilt about past actions.
- Fear of what happens after death.
- Giving morphine alone will not relieve total pain.
- We must also provide emotional support, social help, family counseling, and spiritual care.
- The four dimensions are interrelated (connected). For example:
- Worry about money (social) makes pain feel worse (physical).
- Fear of death (spiritual) causes anxiety (psychological) that increases pain.
- Lack of sleep (physical) causes anger (psychological).
Case: A 45-year-old mother with advanced breast cancer cries all night, complaining of severe pain in her chest wall. You give her Morphine, but an hour later she is still crying, saying the pain is a 10/10. When you sit and talk to her, she reveals she is terrified about who will pay her children's school fees if she dies.
Question: Which dimension of Total Pain is primarily preventing the morphine from working, and what is your nursing intervention?
Answer: She is experiencing severe Social and Psychological pain (worry over finances and fear of death/abandonment of children). The intervention requires more than just increasing her morphine dose—you must sit with her, provide counseling, and involve a social worker to discuss her children's future. Until her mind is put at ease, her physical perception of pain will remain amplified.
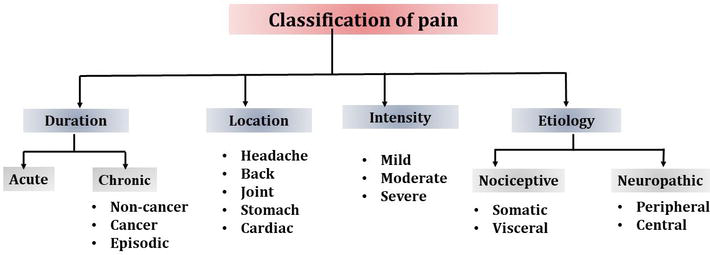
To assess and treat pain effectively, the nurse must understand what type of pain the patient has. Pain can be classified in several ways.
| Feature | Description |
|---|---|
| Onset | Sudden, definite onset. |
| Duration | Limited and predictable (hours to days). |
| Cause | Definite injury or illness (fracture, surgery, infection). |
| Behavior | Help-seeking behavior: crying, moving about, calling for help. |
| Signs | Sympathetic overactivity: fast heartbeat (tachycardia), pale skin (pallor), high blood pressure (hypertension), sweating, grimacing, crying, anxious, dilated pupils (papillary dilatation). |
In cancer: Acute pain may be caused by direct effects of the disease (tumors pressing on nerves/organs) or treatment-related effects (radiotherapy, surgery, and chemotherapy harming tissues).
| Feature | Description |
|---|---|
| Onset | Gradual or ill-defined (unclear when it started). |
| Duration | Continues unabated (does not stop), may become progressively more severe. |
| Cause | Results from a chronic pathological process (cancer, HIV neuropathy, arthritis). |
| Behavior | Patient may appear depressed and withdrawn. They do NOT show obvious distress like acute pain patients. |
| Signs | No signs of sympathetic overactivity. The heart rate, blood pressure, and sweating may be normal! |
💡 Crucial Nursing Note on Chronic Pain
Because chronic pain patients do not look like they are in pain (no crying, no sweating, normal BP), nurses and families often mistakenly think they are exaggerating, faking it, or "getting used to it." This is wrong. Chronic pain is very real, the body has just adapted its vital signs. You MUST believe the patient's report!
This means the nerve pathways are intact (normal). The feeling of pain is a normal response to a harmful stimulus (like a cut, burn, or tumor). It is divided into two groups:
| Feature | Description |
|---|---|
| Location | Skin, muscles, bones, connective tissues. |
| Description | Well localized (patient can point exactly to where it hurts). Described as aching, throbbing, or gnawing. (Gnawing means deep, persistent, boring ache like a rat chewing). |
| Examples | Bone infiltration by cancer, soft tissue infiltration, ulceration, infection, toothache, burns. |
| Treatment | Usually controlled with common analgesics: paracetamol, NSAIDs (ibuprofen, diclofenac) for mild pain, opioids (morphine) for severe pain. Radiotherapy may help for bone pain. |
| Feature | Description |
|---|---|
| Location | Internal organs (liver, stomach, intestines, bladder). |
| Description | Not well localized (patient cannot point to one spot). Described as a feeling of pressure, cramping, or squeezing. |
| Examples | Tumor in an organ, bowel obstruction (blockage), stretching of the liver capsule from tumor growth. |
| Treatment | Paracetamol, NSAIDs, opioids. Steroids can reduce inflammation. Antispasmodics help reduce spasms. |
This means there is damage to the nerve pathways themselves. The nerves send abnormal signals to the brain, even when there is no harmful stimulus.
| Feature | Description |
|---|---|
| Mechanism | Abnormal response to a normal or noxious stimulus. |
| Causes | Nerve infiltration by cancer, infection from HIV or herpes zoster (shingles), peripheral neuropathy from drugs (like some ARVs or TB treatment), CNS injury, pain following surgery. |
| Description | Burning, pricking, stinging, pins and needles, insects crawling under the skin, numbness, hypersensitivity (pain from light touch), shooting pain, electric shocks. |
| Treatment | Adjuvant drugs tend to work better than standard analgesics. Antidepressants (amitriptyline) are most commonly used. Anticonvulsants (carbamazepine, gabapentin) for shooting pain. Neuropathic pain may be partly or totally resistant to opiates like morphine! |
💡 Nursing Implication
If a patient says their pain is "burning" or "like electricity," standard painkillers (paracetamol, diclofenac) alone will not work. Tell the doctor that adjuvant medicines (like Amitriptyline or Gabapentin) are needed.
| Type | What It Means | Examples | Treatment |
|---|---|---|---|
| Peripheral pain | Damage to peripheral nerves (nerves outside the brain and spinal cord). | Nerve compression by tumor, chemotherapy-induced nerve damage. | Targeted nerve pain medications (gabapentin, amitriptyline). |
| Central pain | Damage to the central nervous system (brain or spinal cord). | Stroke, spinal cord injury, tumor pressing on the spinal cord. | Neuropathic pain medications. |
| Type | Description | Example | Management |
|---|---|---|---|
| Breakthrough pain | A sudden, transitory (temporary) increase in pain that "breaks through" regular pain control. | A patient who is comfortable on morphine suddenly has severe pain. | Adjust the pain management plan. Give extra ("rescue") doses of short-acting medicine. |
| Incident pain | Pain that occurs only in specific circumstances, usually related to movement or activity. | Pain when the patient turns in bed, walks, coughs, or is moved by the nurse. | Address the specific trigger. Give medicine before the activity if possible. |
| Procedural pain | Pain caused by medical procedures. | Pain during wound dressing, catheter insertion, injection, blood draw. | Give appropriate pain management before the procedure. |
Important in children: Incident pain and procedural pain are particularly significant in children. Children may become terrified of nurses and doctors if procedures hurt. Always give pain relief before painful procedures.
| Concept | Description | Analogy | Influencing Factors |
|---|---|---|---|
| Pain Threshold | The minimum intensity at which a stimulus is perceived as painful. It is the physiological point where "sensation" becomes "pain." | Like a smoke detector setting; the point where the amount of smoke triggers the alarm to sound. | Genetics, neurological health, and the sensitivity of pain receptors (nociceptors). |
| Factors Lowering Threshold | Conditions that make a person more sensitive to pain, meaning less stimulation is required to feel hurt. | Like a hair-trigger on a doorbell that rings even if a light breeze hits it. | Lack of sleep, anxiety, depression, fatigue, and chronic inflammation. |
| Factors Raising Threshold | Conditions that increase resilience to pain, meaning a stronger stimulus is needed before it is felt. | Like wearing thick gloves that prevent you from feeling the prick of a needle. | Distraction, strong emotions (like adrenaline), certain medications, and relaxation techniques. |
Pain is not just about the injury or disease. Many factors make pain feel worse or better.
| Factor | Why It Increases Pain |
|---|---|
| Discomfort | Being uncomfortable (hot, cold, lying on a hard bed, dirty sheets) focuses attention on pain. |
| Insomnia | Tired brains cannot cope with pain. Pain feels worse at night. |
| Fatigue | Physical exhaustion lowers the body's ability to tolerate pain. |
| Anxiety | Worry and fear make the body tense and amplify pain signals. |
| Fear | Fear of death, fear of more pain, fear of being alone — all increase suffering. |
| Anger | Anger releases stress hormones that increase inflammation and pain perception. |
| Sadness | Depression and sadness lower the brain's natural pain-blocking chemicals. |
| Depression | Depressed patients feel pain more intensely and respond less to treatment. |
| Boredom | When the mind has nothing else to focus on, pain becomes the center of attention. |
🧠 Mnemonic: Factors That Increase Pain
Remember: "DAFIA BED"
Discomfort
Anger
Fatigue
Insomnia
Anxiety
Boredom
Exhaustion
Depression
| Factor | Why It Decreases Pain |
|---|---|
| Relief of other symptoms | When nausea, constipation, or shortness of breath are treated, pain feels less severe. |
| Understanding | When the patient understands what is happening and what to expect, fear decreases and pain decreases. |
| Companionship | Having someone sit with you, hold your hand, or talk to you distracts from pain and releases calming hormones. |
| Creative activity | Music, drawing, storytelling, or prayer distract the brain from pain. |
| Relaxation | Relaxed muscles and slow breathing reduce tension and pain. |
| Reduction in anxiety | When anxiety is treated (through counseling or medicine), pain decreases. |
| Elevation in mood | Happiness and hope release natural painkillers (endorphins) in the brain. |
| Analgesics | Directly block pain signals. |
| Anxiolytics | Anti-anxiety medicines reduce anxiety that amplifies pain. |
| Antidepressants | Treat depression and can also directly reduce nerve pain. |
- The patient's mood: A happy patient tolerates pain better than a sad patient.
- The patient's morale: Hope and determination reduce pain. Hopelessness increases it.
- The meaning of the pain: If a patient thinks "This pain means I am dying," the pain feels worse. If they think "This pain is being treated and I will be comfortable," it feels better.
- Psychological and spiritual factors: Beliefs, prayers, and mental strength affect pain.
- Social circumstances: A patient with family support feels less pain than an isolated patient.
- Emotional component: Patients may describe pain as "agonizing," "cruel," or "terrible" — these words show the emotional weight of pain.
- Gender differences: Men and women may experience pain differently due to biological, psychological, and social factors. Women may report pain more openly; men may hide it due to cultural expectations of toughness.
- Integrated multi-disciplinary teams: Managing chronic pain requires doctors, nurses, counselors, social workers, and spiritual leaders working together.
- Holistic support: Addressing feelings of helplessness, building resilience, and caring for the whole person improves pain control.
Severe pain in advanced illness has negative effects on every part of the patient's life.
- Pain causes stress hormones (like cortisol and adrenaline) to flood the body, which can:
- Increase heart rate and blood pressure.
- Suppress the immune system (making the patient more vulnerable to infections).
- Interfere with digestion and sleep.
- Psychologically, pain causes anxiety, depression, anger, and hopelessness.
Pain does not exist alone. It interacts with and worsens other symptoms:
- Nausea: Pain makes nausea worse.
- Constipation: Pain and opioids both cause constipation. (Physiological note: Pain causes sympathetic nervous system firing, which halts GI peristalsis).
- Shortness of breath: Pain makes breathing shallow and fast.
- Depression: Pain causes depression; depression causes more pain.
- Anxiety: Fear of pain causes anxiety.
- Insomnia: Pain prevents sleep; lack of sleep increases pain.
The patient's ability to move, work, eat, bathe, and care for themselves is further impaired. A patient who could walk with mild pain may become completely bedridden with severe pain.
- Autonomy (the ability to make one's own choices and control one's own life) is challenged. The patient cannot do what they want. They must depend on others for everything.
- Dignity is challenged. The patient may feel humiliated by needing help with toileting, bathing, or feeding. Uncontrolled pain makes a person feel helpless and stripped of their humanity.
The patient and family may interpret severe pain as a sign that death is coming very soon. This causes panic, grief, and spiritual crisis.
💡 Nursing Role: Reassurance
Reassure the patient that pain can be controlled. Pain does not always mean death is hours away. Good pain control can allow weeks or months of meaningful life.
Despite knowing how to treat pain, many patients in Uganda and other countries suffer unnecessarily because of these barriers:
- Nurses and doctors do not ask about pain regularly.
- They do not use pain assessment tools.
- They rely on vital signs (heart rate, blood pressure) instead of asking the patient. Remember: In chronic pain, vital signs may be normal even when pain is severe.
- Health workers do not know about the WHO analgesic ladder.
- They do not know how to use morphine safely.
- They do not know the difference between nociceptive and neuropathic pain.
- Fear of constipation, drowsiness, or addiction prevents health workers from prescribing strong painkillers. (This irrational fear of prescribing opioids is called "Opiophobia").
- Families refuse morphine because they fear the patient will die sooner or become a "drug addict."
- Myths about pain:
- "Pain is normal and must be endured."
- "Strong pain medicine is only for dying people."
- "If I take morphine now, it won't work later."
- "Pain means the cancer is spreading — there is no point treating it."
- Myths about opioids:
- "Morphine is addictive." (Truth: Addiction is extremely rare when opioids are used properly for severe cancer pain).
- "Morphine causes death."
- "Morphine is illegal."
- In Uganda, morphine may not be available in all health facilities.
- Patients live far from hospitals and cannot afford transport.
- Palliative care services are concentrated in cities, leaving rural areas underserved.
💡 Nursing Role: Advocacy
As nurses, we must educate patients and families, advocate for better access to medicines, and treat pain aggressively wherever we work. You are the bridge between the suffering patient and the life-changing medication!
Different types and causes of pain look and feel different. Recognizing the clinical presentation helps nurses identify the type of pain and suggest the right treatment.
| Type of Pain | Clinical Presentation & Description | Common Examples |
|---|---|---|
| Visceral Pain | Not well localized. Constant, aching sensation. Often described as deep, squeezing, or cramping. | Pain from a liver tumor or bowel obstruction. |
| Bone Pain | Well localized with local tenderness. Resembles a nagging toothache (persistent, deep, throbbing). Worsens with movement and weight bearing. (Physiology: Tumors release prostaglandins which stimulate osteoclasts to destroy bone). | Cancer that has spread (metastasized) to the spine, hip, or leg bones. |
| Colic (Colicky Pain) | Gripping pain associated with spasms (sudden muscle contractions). Comes in waves — intense pain, then relief, then intense pain again. | Bowel obstruction, kidney stones, bladder spasms. |
| Raised Intracranial Pressure (ICP) | Generalized headache. Worsens in the mornings and when lying down (because lying flat prevents venous drainage from the head, increasing pooling). Accompanied by nausea, projectile vomiting, and blurred vision. | Brain tumor, brain infection (toxoplasmosis or cryptococcal meningitis in HIV patients). |
| Neuropathic Pain | Burning, sharp, stabbing, shooting, or a nagging ache. Associated with numbness, tingling, or hypersensitivity. May follow a dermatomal distribution (a specific nerve path/band on the skin). | Shingles (herpes zoster) pain on chest/face; HIV peripheral neuropathy causing burning feet. |
| Spiritual Pain | Emotional form of suffering. Expressed through nightmares. Feeling abandoned by God, worthless, or meaningless. | "God has forgotten me" or terrifying dreams about death. |
Sometimes pain shows through behavior rather than words:
- Refusal to take medication: The patient may be too sore to swallow, or the medicine may cause pain.
- Self-harming behaviors: The patient may hit themselves, pull at wounds, or become aggressive. This can be a sign of severe, uncontrolled pain or confusion.
- In Uganda and many African countries, pain is undertreated.
- Many patients with cancer and HIV/AIDS suffer until death because they cannot access strong pain medicines.
- Less than 5% of cancer patients have access to chemotherapy or radiotherapy, so pain control becomes the most important treatment.
- HIV-related neuropathy: Burning pain in the feet and legs, often caused by the virus or by anti-retroviral drugs (ARVs) like stavudine (d4T).
- Kaposi's sarcoma pain: Painful skin lesions and swelling, especially in the legs.
- Cancer pain: Cervical cancer, breast cancer, prostate cancer, and lymphoma are common and often present late with severe pain.
- Tuberculosis (TB) pain: Chest pain, bone pain from TB of the spine (Pott's disease).
- Malaria and other infections: Headaches, muscle pain, joint pain.
- Some patients believe pain is a punishment from God or ancestors.
- Some believe they must endure pain silently to show strength.
- Some fear that taking strong medicine means they are giving up hope.
- Nursing response: Educate gently. Explain that pain relief is part of God's care and that strong medicine allows the patient to pray, be with family, and live with dignity.
Nurses are often the only health workers available in rural areas. Nurses must be able to assess pain, give pain medicines, teach families, and advocate for better access to morphine. Every nurse in Uganda must know the WHO analgesic ladder and how to use oral morphine.
- Pain is whatever the patient says it is. Believe them.
- Pain has four dimensions: Physical, psychological, social, spiritual. Treat all four.
- Acute pain has signs (fast heart rate, sweating, crying). Chronic pain often does not. Do not rely on vital signs alone.
- Nociceptive pain responds to standard painkillers. Neuropathic pain needs adjuvant medicines.
- Morphine is safe and essential for severe pain. It does not kill patients when used correctly.
- Constipation is the only side effect of morphine that never goes away. Always give laxatives.
- Pain in children is real and often undertreated. Use age-appropriate tools.
- In Uganda, pain is a major public health issue. Nurses are the frontline warriors against it.
Case: A 70-year-old male with advanced prostate cancer is lying perfectly still in bed. His HR is 72, BP is 120/80, and he is not sweating. However, when you ask him, he says his pain is a 9/10. The nursing student next to you whispers, "He must be lying, his vitals are normal and he isn't crying."
Question: How do you correct the student using the principles of palliative care pain?
Answer: You explain that this patient has Chronic Pain. In chronic pain, the body's sympathetic nervous system adapts, meaning the heart rate, BP, and sweating return to normal. Furthermore, patients with chronic pain often lie still or appear withdrawn rather than crying out. The golden rule is: "Pain is what the patient says hurts."
Memorize these formulas to easily recall complex lists during your nursing exams!
🧠 "Please Stop Playing, Start Living"
- Physical
- Social
- Psychological
- Spiritual
- Living (Reminder that total pain affects the whole life)
- Nociceptive = Normal nerves, Normal response
- Neuropathic = Nervous nerves, Nasty signals
🧠 "SHOCK & PAIN"
- Sweating
- Hypertension (high BP)
- Obvious distress (crying, moving)
- Crying
- Keep watching (tachycardia)
- Pallor (pale skin)
- Anxiety
- Increased heart rate (tachycardia)
- Non-stop complaints
🧠 "The DARK Side"
- Depressed
- Apathy (lack of interest)
- Restless or withdrawn
- Kept inside (hidden suffering, normal vitals)
🧠 "DAFIA BED"
- Discomfort
- Anger
- Fatigue
- Insomnia
- Anxiety
- Boredom
- Exhaustion
- Depression
🧠 "BAD MAP"
- Beliefs and myths (patient/doctor attitudes)
- Access problems (services unavailable)
- Don't know (inadequate knowledge)
- Missing assessment (inadequate pain assessment)
- Afraid of side effects (Opiophobia)
- Poor services (poorly accessible)
📝 Make sure you can do the following before entering the exam room:
- Know both definitions of pain (IASP and McCaffery) word for word.
- Be able to draw and explain the pain pathway: nociceptors ➔ peripheral nerves ➔ dorsal horn ➔ spinothalamic tract ➔ thalamus ➔ cerebral cortex.
- Name the chemical mediators of pain: prostaglandins, bradykinin, serotonin, histamine, potassium, hydrogen ions.
- Explain Total Pain with all four dimensions and give examples for each.
- Compare acute and chronic pain in a table (onset, duration, signs, behavior, sympathetic activity).
- Compare somatic and visceral pain (location, description, examples, treatment).
- Describe neuropathic pain and why it needs adjuvant drugs, not just morphine.
- Know the African HIV pain study percentages (lower limb 66%, mouth 50.5%, headache 42.3%, throat 39.8%, chest 17.5%).
- List the factors that increase and decrease pain.
- Describe the clinical presentation of bone pain, visceral pain, raised intracranial pressure, and neuropathic pain.
- List the barriers to pain management and how nurses can overcome them.
- State the principles of pain management (comprehensive approach, multiple causes, WHO ladder, subjectivity, pediatric considerations).
- International Association for the Study of Pain (IASP). (2007). IASP Taxonomy.
- McCaffery, M. (1968). Nursing practice theories related to cognition, bodily pain, and man-environment interactions.
- Saunders, C. (1964). The symptomatic treatment of incurable malignant disease.
- World Health Organization (WHO). Cancer pain relief and palliative care.
Thank you for saving us.
I’m glad
My request is that you should find a way for me to get a soft copy of these notes to keep in my phone gallery
Please 🥺🥺
Thanks for the information …..though am wondering where we can incorporate the WHO analgesic ladder in this whole thing about pain assessment and management
check in pain management
Thanks for the information bro