

Pain assessment is the systematic process of gathering information about a patient's pain. It is the first and most important step in pain management. If we do not assess pain properly, we cannot treat it properly.
Good assessment is the key to effective pain management. Without assessment, we are only guessing — and guessing causes suffering.
We covered Pain already, incase you want to view Pain Introduction, Click Here.- Nurses spend the most time with patients.
- Nurses are often the first to notice when a patient is in pain.
- Nurses give the pain medicines and must know if they are working.
- In Uganda, where doctors may not be present in every ward or clinic, nurses are frequently the main health workers responsible for pain assessment.
- You cannot treat what you do not understand.
"Pain is whatever the patient says it is, existing whenever they say it does."
- Believe the patient. If they say they have pain, they have pain.
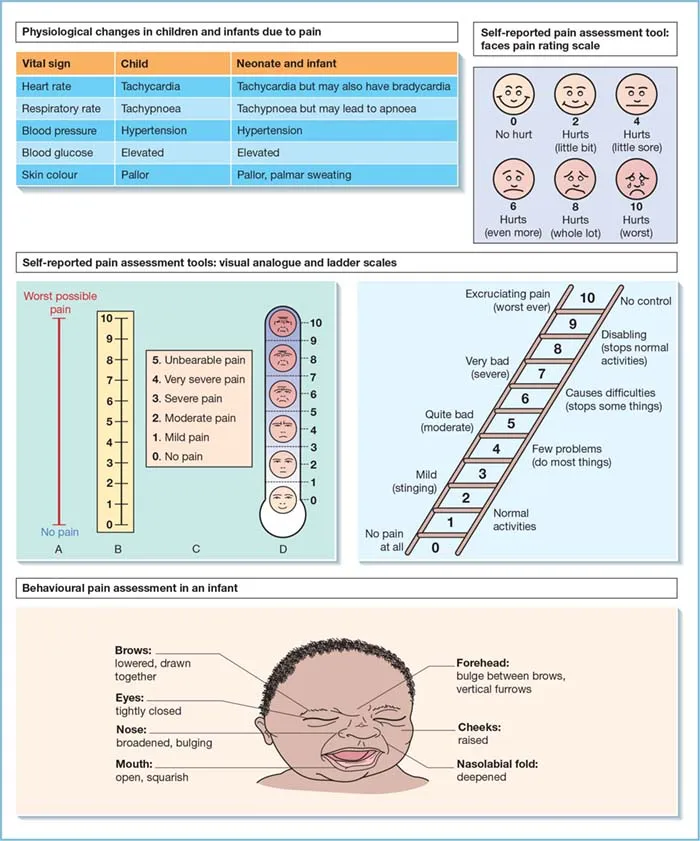
- Do not rely only on vital signs (heart rate, blood pressure) to decide if someone is in pain. In chronic pain, these signs may be normal even when pain is severe.
Pain is not just a physical sensation. It has physical, psychological, social, spiritual, and cultural dimensions. A thorough assessment looks at all of these.
- Pain must be assessed at every patient contact.
- After giving pain medicine, reassess to see if it worked.
- Measure pain at regular intervals: every 6 hours, every 4 hours, or every 2 hours in severe cases.
- Use simple tools and simple language.
- Complex questionnaires may be too demanding for very sick palliative care patients.
- Use tools that match the patient's literacy level, language, and culture.
A thorough pain assessment goes far beyond asking "Where does it hurt?" We must assess the whole person.
Use these questions to build a clear picture of the physical pain:
| Question | What to Ask | Why It Matters |
|---|---|---|
| Onset | "When did the pain start?" | Tells us if the pain is new, worsening, or chronic. |
| Nature | "What does the pain feel like?" (burning, stabbing, throbbing, aching, stinging) | Helps identify the type of pain. Words like "shooting," "burning," or "electric" suggest neuropathic pain, which needs different medicines. |
| Site & Radiation | "Where is the pain? Does it spread to other areas?" | Helps locate the source. Referred pain may indicate specific organ or nerve involvement. |
| Type | "What type of pain is it?" | Is it somatic, visceral, neuropathic, or bone pain? |
| Duration & Changes | "How long has the pain been there? Has it changed?" | Tells us if the disease is progressing or if treatment is failing. |
| Precipitating / Aggravating Factors | "What makes it worse?" (movement, eating, coughing, lying down, bowel movement) | Helps us plan care. For example, if movement worsens pain, we give medicine before turning the patient. |
| Relieving Factors | "What makes it better?" (rest, heat, cold, prayer, sitting up, medicines, herbs) | Helps us choose treatments and understand what the patient has already tried. |
| Impact on Function | "Does it stop you from walking, sleeping, eating, or working?" | Shows how much the pain is destroying quality of life. |
| Impact on Mood & Sleep | "Does the pain make you sad, angry, or unable to sleep?" | Links physical pain to psychological suffering. |
| Previous Medications | "What have you taken before? Did it help? Any side effects?" | Guides future prescribing. If paracetamol failed, we move up the WHO ladder. |
| Meaning of Pain | "What do you think this pain means?" | The patient may think "This pain means I am dying." This fear makes pain feel worse. |
- Inspect: Look at the body for swelling, redness, wounds, pressure sores, or visible tumors.
- Palpate: Gently touch the painful area to check for tenderness, masses, or temperature changes.
- Auscultate: Listen to bowel sounds, breathing, and heart sounds if relevant.
- Check movement: Can the patient move? Are they guarding a limb? Is there stiffness?
- Document findings: Record everything in writing and mark pain locations on a body chart.
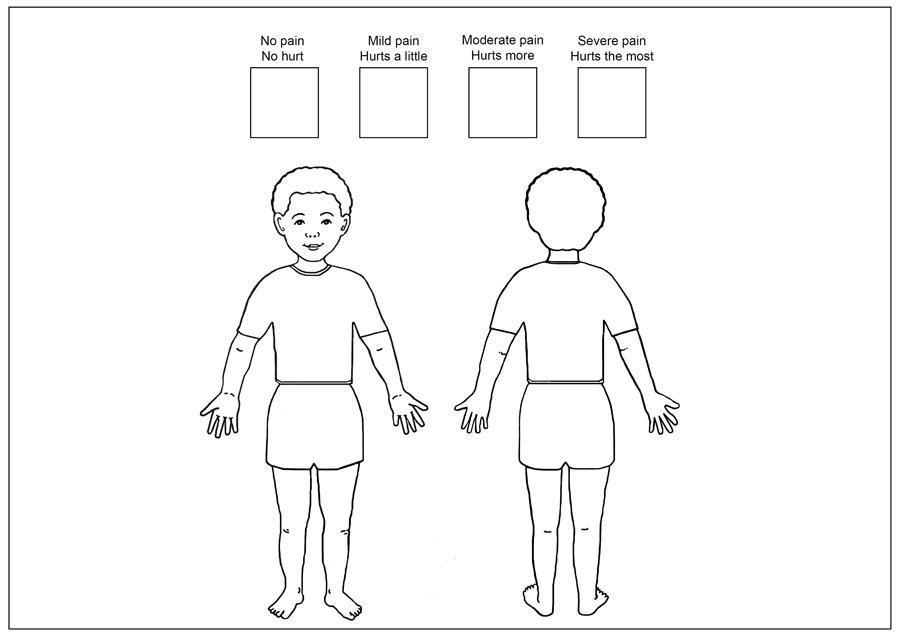
A body chart is a simple drawing of a human body. The patient marks where they feel pain. This is especially useful when:
- The patient has pain in more than one place.
- The patient has difficulty describing locations with words.
- The nurse needs to compare pain locations over time.
How to use it: Give the patient a pen and ask them to mark an X where it hurts the most. Use different marks (circles, shading) for different types or intensities of pain.
In palliative care, we do not order endless tests. We limit investigations to those that will significantly impact treatment decisions.
- Example: Ordering an X-ray to see if a bone is broken may change how we position the patient.
- Example: Ordering a CT scan just to "confirm what we already know" may be unnecessary and cause the patient distress and expense.
Understand how far the disease has progressed. This helps us know if the pain is from: The disease itself (tumor pressing on a nerve), A complication (infection, fracture), or Treatment side effects.
Pain is deeply affected by the mind. A patient who is terrified or depressed feels more pain. Ask about:
| Area | Questions to Ask |
|---|---|
| History of illness & understanding | "What do you understand about your illness?" "What have the doctors told you?" |
| Emotional & psychological response | "How are you feeling inside?" "Are you sad, scared, or angry?" |
| Role impact | "How is the illness affecting your role as a parent, mother, father, lover, or breadwinner?" |
| Hopes & fears | "What are you hoping for?" "What are you most afraid of?" |
| Future plans | "Do you have plans for the future?" (This reveals hope or hopelessness). |
| Losses & disappointments | "What have you already lost because of this illness?" (job, independence, body image). |
| Unfinished business | "Is there anything you still want to do or say?" |
| Things to accomplish | "What is most important to you now?" |
Why this matters in Uganda: Many patients fear that pain means death is coming. This fear makes the pain feel worse. Addressing the fear is part of treating the pain.
Pain does not exist in a vacuum. A patient who is worried about school fees or eviction feels more pain. Ask about:
| Area | Questions to Ask |
|---|---|
| Role impact | "How is the illness affecting your ability to work and care for your family?" |
| Family history | "Who is around you? Where are they? How important are they? How supportive are they?" |
| Life stresses | "What is happening with money, jobs, housing, children, and sources of support?" |
| Genogram (Family Tree) | Draw a family tree. This helps the patient open up, shows family patterns, reveals conflicts, and acts as a therapeutic tool to discuss death and vulnerabilities. |
Nursing action: If a patient is in pain AND worried about rent, relieving the pain is only half the battle. Link them with social support.
Spiritual pain can feel like physical pain. Patients may say "My heart hurts" when they mean they are spiritually broken. Assess:
| Time Frame | What to Explore |
|---|---|
| Past | Regrets, guilt, shame. "Is there anything in your past that troubles you?" |
| Present | Anger, grief for the loss of their own life, lost sense of purpose. "Do you feel life still has meaning?" |
| Future | Hopes and fears of dying and death. "Are you afraid of what comes after death?" |
In Uganda: Many patients are deeply religious. Spiritual pain may be expressed as "Why has God allowed this?" or "I am being punished." Recognizing this helps us provide spiritual care alongside pain medicine.
Culture shapes how pain is expressed, treated, and understood. In Uganda, with over 50 ethnic groups, cultural assessment is essential.
| Area | What to Assess |
|---|---|
| Symptom description | How does the patient describe pain? Some cultures use words like "heat," "heaviness," or "wind" rather than "pain." |
| Language | Does the patient speak English? Do they need an interpreter? |
| Family role | Who makes decisions? The patient, the elder, the husband, or the eldest son? |
| Autonomy & confidentiality | Can the patient keep their diagnosis private, or does the family demand to know everything? |
| Attitudes toward ill-health | Is illness seen as a curse, punishment, or natural event? |
| Food & diet | Are there cultural foods or restrictions that affect medicine-taking? |
| Western medicine vs. other therapies | Has the patient used herbs, traditional healers, or prayers? Do they trust modern medicine? |
| Attitudes toward death | Is death discussed openly or taboo? |
| Rituals surrounding death | Are there specific rituals the patient wishes to observe? |
Nursing action: Respect cultural beliefs. Do not dismiss traditional medicine — ask about it, and work with it when safe.
The PQRST tool is a simple, structured way to remember all the important questions to ask about pain. It is one of the most important tools for nursing exams and clinical practice.
- "Where is the pain?" "Can you point to where the pain is?" "Does the pain spread?" "Put an X where it hurts the most."
- "Does anything worsen the pain, such as eating, bowel movements, or movement in general?"
- "Does anything alleviate or improve the pain?"
- "Does the pain get better when staying still?"
- "Does it improve after having a bowel movement?"
- "Does it improve after wound discharge?"
- "Does using hot or cold compresses help?"
- "Does praying or being with friends provide relief?"
- "Have you tried any medications, painkillers, or herbs? Do they help?"
- "Did any treatment reduce or eliminate the pain?"
"What does the pain feel like to you?" "How would you describe your pain?"
| Words the Patient Uses | What It May Mean | Type of Pain |
|---|---|---|
| "Aching," "throbbing," "gnawing" | Somatic or bone pain | Nociceptive |
| "Cramping," "squeezing," "pressure" | Visceral (organ) pain | Nociceptive |
| "Burning," "shooting," "stabbing," "electric," "pins and needles" | Nerve damage | Neuropathic |
| "Dull," "constant," "heavy" | Deep tissue or organ involvement | Mixed |
Why this matters: Neuropathic pain (nerve pain) does not respond well to standard painkillers like morphine alone. It needs adjuvant medicines (amitriptyline, gabapentin). If you hear words like "burning" or "shooting," you must tell the doctor.
"Where does the pain start?" "Does the pain radiate to any other areas?"
- Examples of radiation: Back pain that radiates down the leg = sciatica (nerve compression). Shoulder pain from liver cancer = referred pain from the diaphragm. Chest pain radiating to the arm = heart pain (angina).
- Site: "Where is your pain?" (Use a body chart). Mark the exact location.
- Severity: "On a scale of 0 to 5, how severe is the pain?" (Or 0 to 10, but 0-5 is easier in Uganda). "How does the pain affect your daily life?" "Does it prevent you from engaging in normal activities, sleeping, moving, sitting, or eating?"
- "How long have you had the pain?"
- "Is the pain constant or does it come and go?"
- "Does the pain worsen at a specific time of day or night?"
- "Have you received any previous pain treatments?"
- "Are you on any pain treatment now? Does it help?"
This is sometimes added to PQRST as a sixth element. It is critical in palliative care.
- "What are your fears about the pain?" "What do you think is causing the pain?" "What does the pain mean to you?"
- Common answers in Uganda: "I'm being punished." "I'm going to die." "There is no hope." "I have to suffer; it is my destiny." "I'm being eaten away."
- Nursing action: When you know what the pain means to the patient, you can address the fear AND the physical sensation. If a patient believes pain means death, reassurance that pain can be controlled gives them hope.
Case: A patient with advanced cervical cancer complains of pain. When you ask her to describe it (The "Q" in PQRST), she says, "It feels like an electric shock shooting down my right leg."
Question: What type of pain is this, and why is this distinction crucial for your treatment plan?
Answer: This is classic Neuropathic Pain (nerve pain). It is crucial because standard WHO ladder painkillers (like Paracetamol or even Morphine alone) are often ineffective. You must alert the doctor to prescribe an adjuvant medication like Gabapentin or Amitriptyline.
Pain assessment tools help us measure pain so we can track it over time and see if treatment is working. They turn a subjective experience into a number or picture we can record.
- Establish a baseline score at the first assessment.
- Reassess regularly and plot scores on a graph to see trends.
- Choose a tool that matches the patient's understanding and literacy level.
- Remember: Most tools do not measure anxiety. Anxiety and pain have similar behavioral signs (restlessness, grimacing). It is possible to measure anxiety instead of pain. Always ask about both.

Ask the patient to rate their pain intensity on a numerical scale (0 = No pain, 10 = Worst pain imaginable). In Uganda, it is easier to use a 0 to 5 scale:
| Score | Meaning | Nursing Action |
|---|---|---|
| 0 | No pain | Continue monitoring. |
| 1 | Little pain | Mild — may need non-drug methods or paracetamol. |
| 2 | A bit more pain | Mild to moderate — monitor closely. |
| 3 | Quite some pain | Moderate — may need weak opioid (codeine). |
| 4 | Quite a lot of pain | Severe — needs strong opioid (morphine). |
| 5 | Overwhelming pain — worst imaginable | Severe — needs morphine urgently. |
- Verbal-Descriptor Variation: Instead of numbers, use words: "No pain", "Mild pain", "Mild-to-moderate pain", "Moderate pain", "Severe pain", "Very severe pain".
- How to use with patients who struggle with numbers: Use fingers: "Show me with your fingers how bad the pain is. Zero fingers = no pain. Five fingers = worst pain."

Uses a hand gesture to represent pain level:
- Clenched fist (0 fingers) = No hurt / No pain at all.
- 1 finger extended = A little pain.
- 2 fingers extended = A bit more pain.
- 3 fingers extended = Quite some pain.
- 4 fingers extended = Quite a lot of pain.
- 5 fingers extended (open hand) = Hurts worst / Worst possible pain.
- Important cultural warning: In some cultures, a closed fist might be interpreted as the worst possible pain (anger, fighting). You must explain the scale clearly to the patient.
- Example explanation for a Ugandan patient: "I would like to find out the level of pain that you have. Can you tell me on a scale of 0 to 5, where 0 is no pain at all, 1 is a little pain, 2 is a bit more, 3 is quite some pain, 4 is quite a lot of pain, and 5 is overwhelming pain — the worst pain imaginable. Where would you put your pain on that scale?"
- Note on African use: Experiences in Africa have shown that many people prefer the Hand Scale over the Faces Scale because it feels more natural and less like a child's tool.
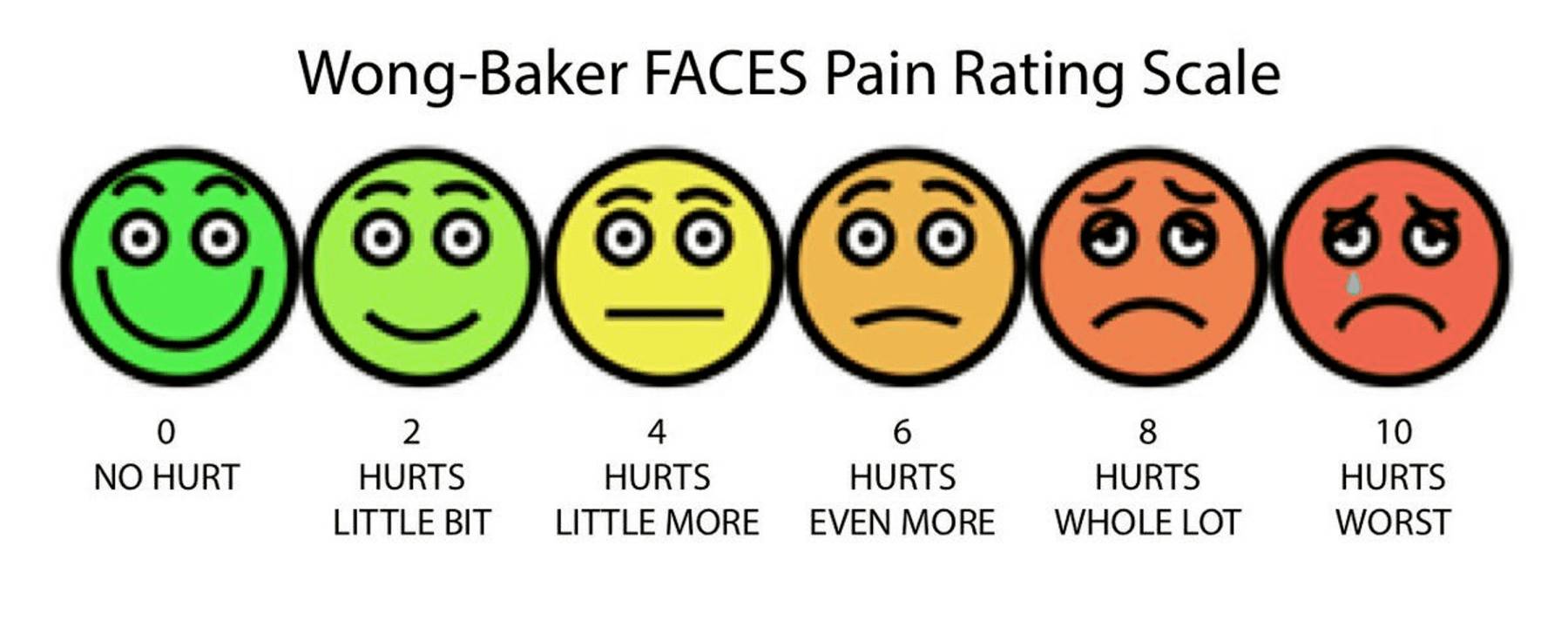
- Shows six cartoon faces with expressions ranging from a broad smile (no hurt) to a very sad, crying face (hurts worst). Numbered 0, 2, 4, 6, 8, 10 (or simplified 0-5).
- Important instructions for the nurse: Train the patient: Explain that they are rating their pain level, not their emotions.
- Bad use: A patient points to a sad face because they feel sad about their diagnosis, not because they are in pain.
- Good use: "Point to the face that shows how much the pain hurts your body, not how sad you feel in your heart."
- When to use it: Best for children, elderly patients with dementia, or adults with low literacy. Be aware that in some African settings, adults may feel this scale is too childish.
- Body Chart: A drawing of the front and back of a human body. Useful for identifying multiple pain sites, referred pain, or radiation.
- Eland Body Scale: Helps assess multiple sites and differing intensities in children. Ask the child to assign colors (e.g., Green = No pain, Yellow = Little, Orange = Moderate, Red = Severe) and color in a body outline. Children may not have the words to describe pain, but they can use colors and drawings.
Pain management in children is complex. Although there are similarities with adults, children have specific needs and challenges.
| Myth | Fact |
|---|---|
| Newborns do not feel pain. | Newborns do have the ability to perceive pain. Their nervous system is developed enough to feel pain. |
| Young children cannot process or remember pain. | Children of all ages can experience and remember pain. Painful experiences in childhood can cause long-term fear of medical settings. |
| Children become accustomed to repeated painful procedures. | Repeated painful procedures still cause distress and pain every time. They do not "get used to it." |
| Children are unable to tell where it hurts. | Children can indicate the location of their pain, especially with tools like the Eland Body Scale or by pointing. |
| Opioids should be avoided due to addiction risk. | Psychological addiction to opioids is rare in children who are using them for real pain. |
| Incomplete myelination means children don't feel pain. | Proper pain perception (nociception) is possible without complete myelination. |
| Younger children have higher pain sensitivity. | Pain tolerance generally increases with age. Younger children may actually feel pain more intensely. |
| Children always communicate when they have pain. | Children may not express pain due to fear of doctors, fear of injections, or wanting to be brave. |
| Children are not aware they have chronic pain. | Children may not recognize or understand chronic pain, but they still feel it. It may show as irritability, refusal to play, or sleep problems. |
| Barrier | Explanation |
|---|---|
| Limited tools | Few age-appropriate, validated pain tools available in our settings. |
| Lack of knowledge | Health workers do not know which tools to use for different ages. |
| Insufficient training | Nurses are not trained in how to use pain scales for children. |
| Difficulty interpreting scores | A child's pain score may not match their behavior. |
| Anxiety vs. psychological pain | Hard to tell if the child is anxious, scared, or actually in physical pain. |
| Factors inhibiting children reporting | Fear of doctors/nurses, fear of illness, reluctance to bother caregivers, avoidance of injections, eagerness to leave the hospital. |
| Letter | Step | What to Do |
|---|---|---|
| Q | Question the child | If the child can respond, ask them directly. If not, question the parent/caregiver. |
| U | Use pain rating scales | Use appropriate scales (Eland Body Scale, Faces Scale, Hand Scale) to quantify pain. |
| E | Evaluate behavior and physiological changes | Watch for crying, facial grimacing, guarding, refusal to move, changes in sleep or eating, increased heart rate, or sweating. |
| S | Secure the caregiver's involvement | Listen to mothers, fathers, and caregivers. Include them in decision-making. They know subtle changes in their child's behavior. Ask them about comforting strategies that work. |
| T | Take the cause of pain into account | Consider the underlying disease or problem. Is the pain from the illness, a procedure, or a side effect? |
| T | Take action and evaluate results | Develop a treatment plan. Reassess using the same pain scale. Adjust treatment. Use pain diaries for chronic pain. |
| Category | Score 0 | Score 1 | Score 2 |
|---|---|---|---|
| Face | No particular expression or smile. | Occasional grimace or frown, withdrawn, disinterested. | Frequent to constant quivering chin, clenched jaw. |
| Legs | Normal position or relaxed. | Uneasy, restless, tense. | Kicking, or legs drawn up. |
| Activity | Lying quietly, normal position, moves easily. | Squirming, shifting back and forth, hesitant to move. | Arched, rigid or jerking. |
| Cry | No cry (awake or asleep). | Moans or whimpers; occasional complaint. | Crying steadily, screams or sobs, frequent complaints. |
| Consolability | Content, relaxed. | Reassured by occasional touching, hugging or being talked to, distractible. | Difficult to console or comfort. |
- 0: Relaxed and comfortable
- 1-3: Mild discomfort
- 4-6: Moderate pain
- 7-10: Severe discomfort or pain or both
- Pain assessment is not a one-time event. It is a continuous cycle.
- After starting treatment: Reassess within 2-3 days of initiating analgesia to see if the medicine is working.
- After each dose: Check pain relief after giving oral medicine (30-60 minutes) or injectable medicine (15-30 minutes).
- Regularly: Every 4-6 hours for stable patients; every 2 hours for severe pain.
- Before and after procedures: Always assess pain before moving a patient, changing a dressing, or inserting a catheter.
| Date | Time | Pain Score (0-5) | Medicine Given | Relief? | Side Effects | Nurse's Notes |
|---|---|---|---|---|---|---|
| 7/7 | 08:00 | 4 | Morphine 10mg | Some relief after 1 hour | None | Patient able to eat breakfast |
| 7/7 | 12:00 | 3 | Morphine 10mg | Good relief | None | Patient slept 2 hours |
| 7/7 | 16:00 | 2 | Morphine 10mg | Good relief | None | Patient sat up and talked to family |
Important warning: Most pain measurement tools do not consider the presence of anxiety. Anxiety and pain have similar behavioral indicators: restlessness, grimacing, fast breathing, crying.
It is possible to measure anxiety and think it is pain. Always ask: "Are you worried or frightened?" as well as "Are you in pain?" If anxiety is high, treat it AND assess whether physical pain is still present.
| Patient Type | Recommended Tool | Why |
|---|---|---|
| Adult, literate, speaks your language | Numerical Rating Scale (0-5 or 0-10) | Quick, easy to track over time. |
| Adult, low literacy, or prefers non-verbal | Hand Scale | Culturally preferred in many African settings. Easy to understand. |
| Child over 3 years | Faces Scale or Hand Scale | Visual and intuitive. |
| Child with multiple pain sites | Eland Body Scale | Shows location and intensity simultaneously. |
| Child under 3 or non-verbal | QUESTT tool + behavioral observation + FLACC | They cannot self-report; rely on behavior and caregivers. |
| Patient with language barrier | Body chart + Hand Scale + interpreter + FLACC | Visual tools transcend language. |
Not asking (assuming patient will tell you), Not believing ("They are exaggerating"), Using vital signs only, Using the wrong tool, Forgetting anxiety.
Fear of addiction (hiding pain to avoid morphine), Fear of injections, Cultural stoicism (enduring pain silently to be strong), Cognitive impairment, Language barrier.
No pain assessment tools available, No time, No training, No documentation forms.
- Assess pain at every contact — Do not wait for the patient to complain.
- Use the right tool — Match the tool to the patient's age, literacy, and culture.
- Believe the patient — Accept their report as truth.
- Assess holistically — Ask about physical, psychological, social, spiritual, and cultural factors.
- Document everything — Record scores, locations, qualities, and impacts.
- Establish a baseline — Get the first score before treatment starts.
- Reassess regularly — Check after medicines and at set intervals.
- Communicate findings — Tell the doctor if pain is severe or not responding to treatment.
- Advocate — If pain is undertreated, speak up for the patient.
- Know the PQRST tool inside out — be able to list every question for each letter.
- Know the difference between the NRS, Hand Scale, and Faces Scale — when to use each, and their advantages in Uganda.
- Be able to explain why the Hand Scale is often preferred in Africa — cultural appropriateness, simplicity.
- Know the myths about pain in children — examiners love to test this.
- Be able to describe the QUESTT tool — all six steps.
- Understand the importance of baseline measurement — you cannot know if treatment worked without a starting point.
- Know the barriers to pain assessment — especially anxiety vs. pain confusion.
- Be able to describe the holistic dimensions — physical, psychological, social, spiritual, cultural.
- Know the reassessment timeline — 2-3 days after starting treatment, every 4-6 hours routinely.
- World Health Organization (WHO) Guidelines on the Pharmacological Treatment of Persisting Pain in Children with Medical Illnesses.
- African Palliative Care Association (APCA) Guidelines for Pain Assessment in African Settings.
- Uganda Ministry of Health - Clinical Guidelines for Pain Management and Palliative Care.
I need to know how I can explain the WHO analgesics ladder
Thanks 😊
They are easy to read and understand
provide us with questions thanks
I appreciate for that organization of the notes, would like to get some knowledge also about the FLACC Scale, thanks 🙏🙏