
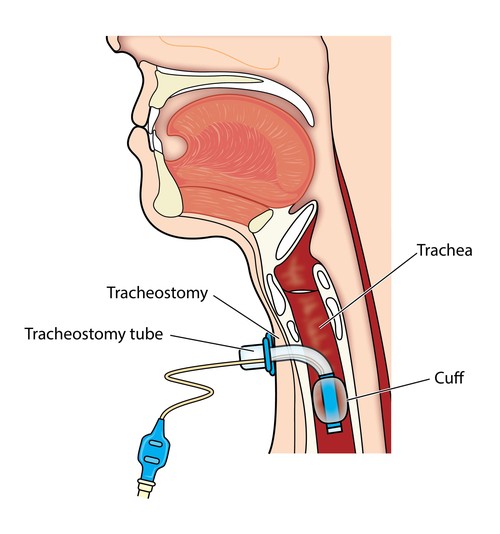
Tracheostomy Tubes
Tracheostomy tubes are essential for patients requiring a long-term airway management. These tubes come in various types and sizes, designed to meet individual needs and anatomical variations.
Types of Tracheostomy Tubes:
- Cuffed: These tubes have an inflatable cuff that seals the trachea, preventing air leaks and aspiration. They are used for mechanically ventilated patients or those at high risk of aspiration. Cuff pressure must be monitored closely to prevent tracheal damage.
- Uncuffed: These tubes lack a cuff, allowing air to flow around the tube. They are suitable for patients who can breathe independently and have a low risk of aspiration. Uncuffed tubes also facilitate speaking and coughing.
- Fenestrated: These tubes have openings on the outer cannula, allowing air to pass through the vocal cords when the inner cannula is removed. They are used for weaning from ventilation or speech therapy.
- Non-fenestrated: These tubes lack these holes, meaning air cannot pass through the vocal cords when the inner cannula is removed. These tubes are typically used for patients who require mechanical ventilation or have a high risk of aspiration.
- Double-Lumen: These tubes have two cannulas: a fixed outer cannula and a removable inner cannula. The inner cannula provides a clear passage for air and secretions, minimizing the risk of tube occlusion.
- Single-Lumen: Single lumen tubes consist of the outer cannula only (there is not an inner cannula). Most pediatric tracheostomy tubes are single lumen tubes, because their diameters are too small to accommodate an inner cannula. However, the entire tracheostomy tube would require to be changed if an obstruction occurred inside the single lumen tube
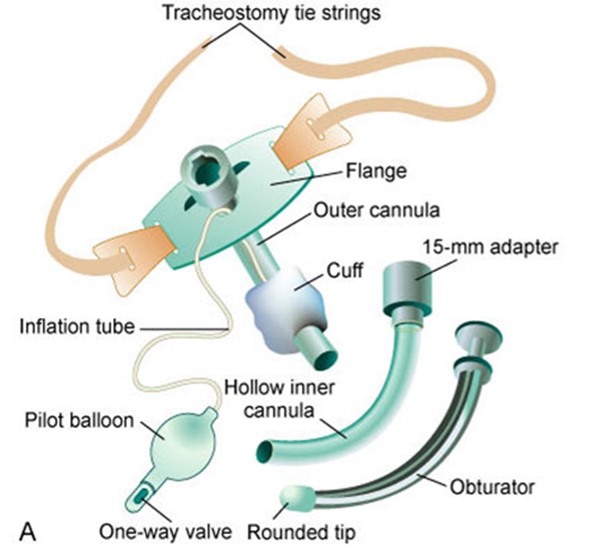
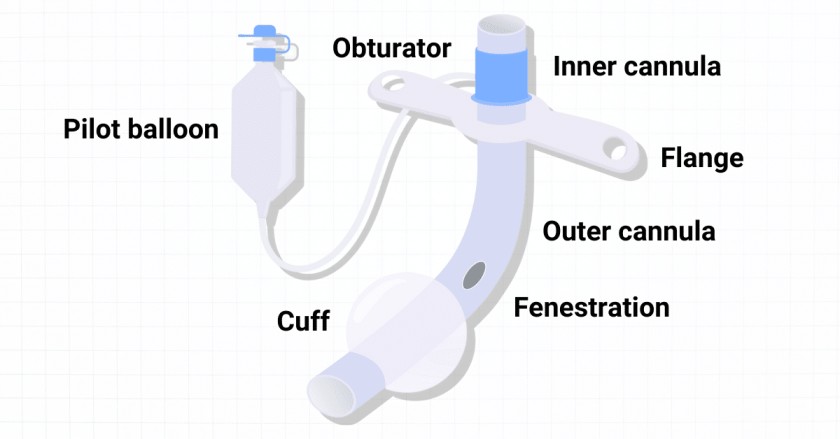
Components of a Tracheostomy Tube:
- Flange: This flat plate rests on the neck, holding the tube in place. It has holes for securing the tube with ties or straps.
- Obturator: A cone-shaped device inserted into the tube during insertion to guide it and prevent tracheal wall injury. It is removed once the tube is in place.
- Pilot Balloon: A small balloon connected to a valve, used to inflate or deflate the cuff and indicates its status.
- Suction Port: An opening on the tube that allows connection to a suction catheter for removing secretions.

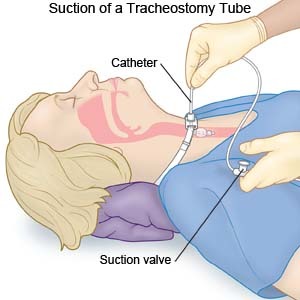
Suctioning
Suctioning of the tracheostomy tube is necessary to remove mucus, maintain a patent airway, and avoid tracheostomy tube blockages. The frequency of suctioning varies and is based on individual patient assessment.
Indications for suctioning.
- Audible or visible signs of secretions in the tube.
- Respiratory distress symptoms.
- Suspected blockage or partial blockage of the tube.
- Inability of the patient to clear secretions through coughing.
- Vomiting.
- Decreased oxygen saturation on pulse oximetry.
- Changes in ventilation pressures (for ventilated patients).
- Patient’s request for suctioning (older children).
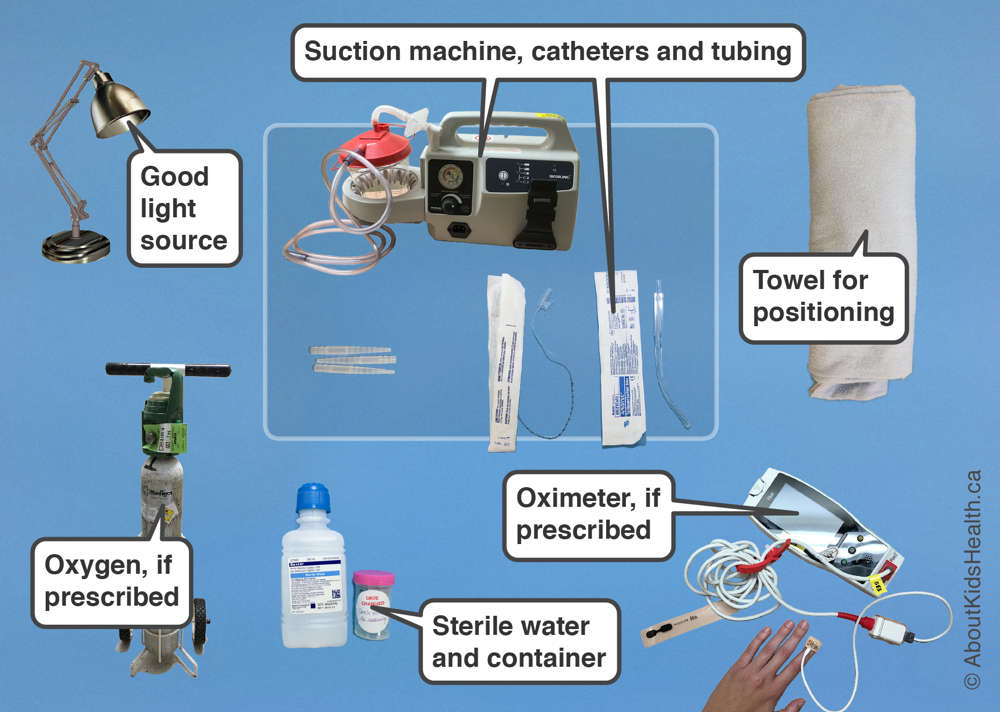
Procedure Preparation
- Ensure Tracheostomy Kit is present.
- Appropriate size suction catheters (with graduations if available).
- Tape measure with depth required for tracheostomy tube suctioning.
- Setting the suction pressure to the correct range: 80-120mmHg is the recommended suction pressure for tracheostomy tube suctioning, with a maximum pressure of 120mmHg when the tube is occluded. Note that the Medigas suction gauges in use may measure pressure in kPa, with the equivalent of 80-120mmHg being 10-16kPa.
Procedure
Detailed Procedure
- Explain to the patient and their family that you are going to suction the tracheostomy tube.
- Apply eye protection.
- Perform hand hygiene, apply non-sterile gloves.
- Remove the mask or breathing circuit.
- Peel open suction catheter end and attach to suction tubing, check and adjust suction pressure gauge to between 80 – 120 mmHg.
- Utilizing a non-touch technique gently introduce the suction catheter tip into the tracheostomy tube to the pre-measured depth.
- Apply finger to suction catheter hole and; gently rotate the catheter while withdrawing. Each suction should not be any longer than 5-10 seconds.
- Assess the patient’s respiratory rate, skin colour and/or oximetry reading to ensure the patient has not been compromised during the procedure.
- Repeat the suction as indicated by the patient’s individual condition.
- Look at the secretions in the suction tubing – they should normally be clear or white and move easily through the tubing. Document changes from normal color and consistency and notify the treating team if the secretions are abnormal color or consistency.
- Rinse the suction catheter with sterile water decanted into a container (not directly from the bottle).
- Replace suction catheter into the packaging.
- Dispose of waste, remove gloves and perform hand hygiene
Note:
- Suction catheters are to be routinely replaced every 24 hours or at any time if contaminated or blocked by secretions.
- Suction water/and the container to be replaced every 24 hours.
- Routine use of 0.9% sodium chloride is not recommended as there is little clinical evidence to support this. However, in situations where this may be of benefit e.g., thick secretions and/or to stimulate a cough 0.5ml of 0.9% sodium chloride can be instilled into the tracheostomy tube immediately prior to the suction procedure.
Special safety considerations:
- Some patients may require assisted ventilation before and after suctioning. If required, this will be requested by the parent medical team. If the correct size suction catheter does not pass easily into the tracheostomy tube, suspect a blocked or partially blocked tube and prepare for immediate tracheostomy tube change.
Pingback: Common tumors of ear nose and throat (ENT) - Nurses Revision
It’s good for revision
Ok thanks so much
Think indications of are the same as when do we do such a procedure
It’s hard for me, l need someone to help me