

Table of Contents
TogglePerform Gastronomy Feeding
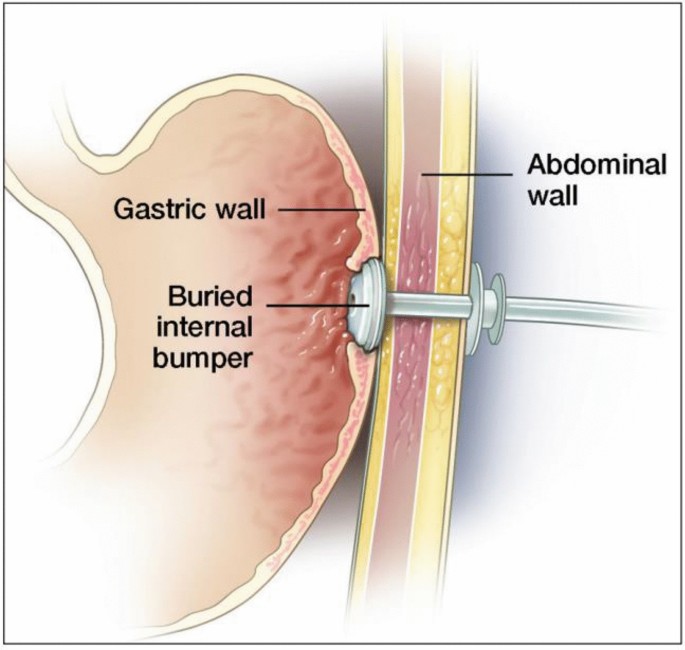
Gastronomy Feeding is feeding of a patient by means of an opening directly into the stomach through the abdominal wall.
They are commonly surgically inserted endoscopically through the abdominal wall, and held in place by an internal balloon or bumper and external fixator. Gastrostomy feeding is a successful method of enteral feeding providing daily nutritional requirements in specialist liquid form directly into a patient’s stomach via a flexible tube.
Indications of Gastrostomy feeding
Inability to Swallow Safely:
- Dysphagia: Difficulty swallowing due to neurological disorders, muscular diseases, or structural abnormalities.
- Aspiration risk: High risk of food or liquids entering the airway, leading to pneumonia.
- Esophageal obstruction: Blockage of the esophagus due to tumors or strictures.
- Carcinoma of the esophagus: Cancer of the esophagus.
- Strictures of the esophagus: Narrowing of the esophagus, often due to inflammation or scar tissue.
- Birth defects of the mouth: Congenital abnormalities affecting the mouth and swallowing ability.
- Esophageal atresia: Congenital absence or closure of part of the esophagus.
- Problems with sucking or swallowing: Difficulties in patients with debilitated diseases like stroke and dementia.
Prolonged Malnutrition:
- Chronic illness: Conditions such as cancer, Crohn’s disease, or cystic fibrosis leading to long-term nutritional deficiencies.
- Anorexia nervosa: Eating disorder characterized by extreme food restriction.
- Severe weight loss: Inability to maintain adequate weight and nutritional intake.
Impaired Digestion & Absorption:
- Short bowel syndrome: Significant reduction in the length of the small intestine, hindering nutrient absorption.
- Malabsorption disorders: Conditions affecting the ability to absorb nutrients, such as celiac disease.
Delayed Gastric Emptying:
- Gastroparesis: Delayed stomach emptying due to neurological or muscular dysfunction.
- Delayed gastric emptying due to medication: Certain medications can slow down gastric emptying.
Coma or Altered Consciousness:
- Severe brain injury: Loss of consciousness or inability to swallow safely.
- Chronic vegetative state: Persistent unconsciousness without awareness or purposeful movement.
Chronic Vomiting or Reflux:
- Severe gastroesophageal reflux disease (GERD): Persistent vomiting and acid reflux leading to malnutrition.
- Intractable vomiting: Persistent vomiting despite medical treatment.
Premature Infants:
- Premature birth: Infants born before 37 weeks of gestation may have underdeveloped digestive systems and require supplemental feeding.
- Failure to thrive: Infants who fail to gain weight or grow adequately.
Operations of the upper gut: Procedures involving the alimentary canal, mouth, nose, and esophagus may necessitate gastrostomy feeding to allow for healing and recovery.
Methods of feeding via a gastrostomy
- Bolus feeding: A volume of liquid feed given usually via a gravity set over a short duration, e.g. 15–20 minutes. The feed is usually delivered via a gravity set, relying on the force of gravity to push the feed into the stomach.
- Continuous feed: This is a feed given via an electronic feeding pump, which allows clinicians and home caregivers to deliver set amounts of enteral formula in a consistent manner, over a desired duration of time. The pump regulates the rate of feed delivery, ensuring a consistent and continuous flow into the stomach.

Types of Feeding Tubes
Feeding tubes are classified based on their length and retention mechanism:
A. Long Tubes:
- Percutaneous Endoscopic Gastrostomy (PEG): A long, flexible tube inserted through the abdominal wall and into the stomach. Placed endoscopically, meaning a thin, flexible tube with a camera is used to visualize the stomach and guide the tube placement. Offers a more minimally invasive approach compared to surgical placement.
- Long Balloon-Retention Tube: A longer tube with a balloon at the end that is inflated within the stomach, securing the tube in place. Commonly used for individuals requiring longer-term feeding.
- Malecot Tubes: A type of long tube that may be used for short-term feeding and is often used for drainage.
B. Skin-Level Tubes:
- Firm Silicone Mushroom Retention: These tubes have a mushroom-shaped end that rests against the stomach lining, preventing accidental tube removal. Examples include Bard feeding tubes.
- Balloon Retention: These tubes have a balloon near the end that is inflated inside the stomach, securing the tube in place. Examples include AMT MINI and MICKEY feeding tubes.
Procedure for administration of Gastrostomy feeding.
REQUIREMENTS
A tray containing;
- A bowel containing funnel/feeding syringe, rubber tubbing, glass or plastic connection.
- Feed at a suitable temperature [37°-38°] 240 to 300mls of strained nourishing fluid in a bowel of warm water.
- Towel and mackintosh cape.
- Warm water in a glass measure container.
- Spigot in a sterile receiver.
At the bedside:
- Hand washing facility.
- Screen.
PROCEDURE
Steps | Action | Rationale |
1. | Observe the general rules of nursing procedure. | |
2. | Expose the gastrostomy catheter. | To aid easy working. |
3. | Protect the bed linen with a mackintosh and towel. | This prevents soiling of the bed. |
4. | Wash hands and check temperature of the feed. | To prevent the spread of infection. |
5. | Aspirate and measure the stomach content before giving the feed. | To ensure feeds are absorbed. |
6. | Pinch proximal end of the gastronomy tube and connect funnel after removing the spigot. | To avoid air entry into the stomach. |
7. | Pour 10mls of water into the funnel, let it run through the tube slowly and followed by a prescribed amount of feed. Rinse the tube with 10m Is of warm boiled water. | To ensure patent tube throughout the procedure. |
8. | Pinch and disconnect the funnel when feeding is over and replace the spigot. | To prevent air entry into the stomach and backflow. |
9. | When the wound has not yet healed carry out gastrostomy toilet i.e. clean skin around the tube with normal saline and apply a protective cream e.g. Zinc Oxide and cover with dry dressing. | To promote healing and prevent infection. |
10 | Record the type, food amount given, and time. | Monitor input and output. |
11. | Provide oral hygiene, clean equipment and leave the patient comfortable. | To prevent infection to the patient. |
12. | Clear the trolley and wash hands. | To prevent cross infection. |
Complications of Gastrostomy Feeding
1. Tube-Related Complications:
- Tube Obstruction: Blockage of the tube due to thickened feed, medications, or debris.
- Primary Malposition: Incorrect initial placement of the tube.
- Perforation of the Intestinal Tract: A hole in the intestinal wall caused by the tube.
- Secondary Displacement of the Feeding Tube: The tube coming out of the stomach or moving out of position.
- Knotting of the Tube: The tube becoming tangled within itself.
- Accidental Tube Removal: The tube being pulled out of the stomach.
- Breakage and Leakage of the Tube: The tube becoming damaged and leaking.
- Leakage and Bleeding from Insertion Site: Fluid or blood leaking from the opening where the tube enters the skin.
2. Site-Related Complications:
- Erosion, Ulceration and Necrosis of Skin and Mucosa: Damage to the skin and lining around the gastrostomy site.
3. Gastrointestinal Complications:
- Intestinal Obstruction (Ileus): A blockage in the intestines.
- Hemorrhage: Bleeding from the stomach or intestines.
4. Systemic Complications:
- Inadvertent IV Infusion of Enteral Diet: Accidental injection of the feeding formula into a vein.
- Infection at the Tube Insertion Site: An infection at the point where the tube enters the body.
- Aspiration Pneumonia: Inhaling food or liquid into the lungs.
- Nasopharyngeal and Ear Infection: Infection of the nose, throat, and ear.
- Peritonitis: Inflammation of the lining of the abdominal cavity.
- Infective Diarrhea: Diarrhea caused by infection.
5. Metabolic Complications:
- Electrolyte Disturbances: Imbalances in the levels of electrolytes, such as sodium, potassium, and chloride.
- Hyper- and Hypoglycemia: High or low blood sugar levels.
- Vitamin and Trace Element Deficiency: Lack of essential vitamins and minerals.
Quick Quiz
Gastrostomy Quiz
FON - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Gastrostomy Quiz
FON
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.

We appreciate though complications of gastrostomy where repeated twice
But we appreciate
Thanks for the knowledge
I only suggest that at least every complication should be given with a rasionale
This is in reference with “chest infections”, “Intestinal obstruction “
i appreciate.
I would request that you add nursing diagnosis label for gastrostomy feeding as well it’s nursing interventions
Otherwise I appreciate your navigation
Thank you Team for the work well organized.
I also say, thank you for the organized work
Well done, organis notes
If I want to be part of you online, what to I do?
Send a whatsapp message on 0726113908
Thanks this is easy to read
Is it gastronomy or gastrostomy
Gastronomy is the art and science of good eating. It involves the study of food, its preparation and its cultural significance.
Gastrostomy is a surgical procedure that creates an opening in the stomach through the abdominal wall. It is used to provide a way for food and liquids to enter the stomach when someone cannot swallow or cannot swallow safely.
Thanks,some notes on identification of instruments with there names
it’s very good system that can enhance self learning