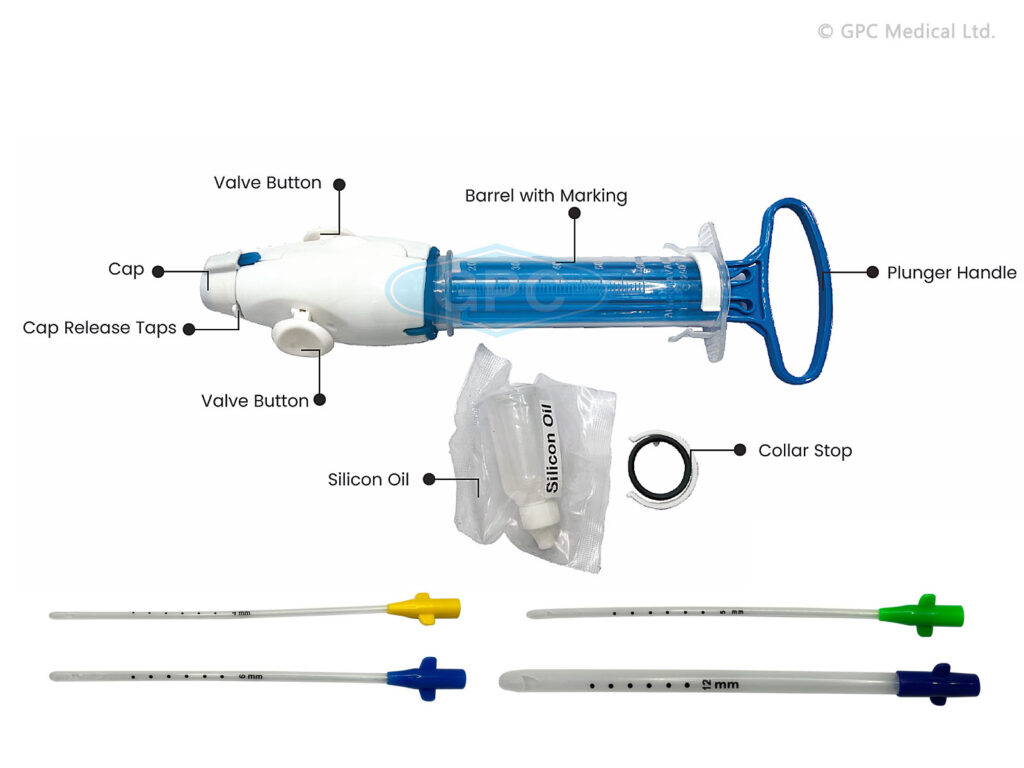
Manual Vacuum Aspiration (MVA):
Manual Vacuum Aspiration (MVA) is a method of termination of pregnancy where a healthcare provider uses a handheld device (an aspirator) to remove the contents from the uterus using suction undertaken with the patient awake. A narrow tube attached to a syringe is used to empty the womb using aspiration (gentle suction). Local anaesthetic is injected into the cervix (neck of the womb) to minimize discomfort.
Manual Vacuum Aspiration (MVA) is a preferred, appropriate, and cost-effective procedure for managing abortion in low-resource settings. It is particularly effective up to 12 weeks of pregnancy and has been proven highly efficacious in several randomized controlled trials. MVA has largely replaced dilation and curettage (D&C) in many industrialized and other countries.
Preparation:
- Prepare the patient, the room, equipment, supplies, and ensure the presence of an assistant.
- Select the appropriate size of the cannula based on the gestational age and uterine size.
Requirements for MVA Procedure:
Trolley (Top Shelf): | Trolley (Bottom Shelf): | Bedside Setup: |
Sterile MVA set Casco speculum Vulsellum uterine sound Receiver Bowl of cotton swabs Sponge holding forceps Cannula | Lidocaine or bupivacaine Syringe and needle KY jelly Antiseptic lotion Gumboots | Buckets Screens Apron
|
Procedure for Manual Vacuum Aspiration:
1. Review Indications:
- Inevitable abortion before 16 weeks
- Incomplete abortion
- Molar pregnancy
- Delayed postpartum hemorrhage due to retained placental fragments
2. Provide Emotional Support and Encouragement: Ensure the woman feels supported and reassured throughout the procedure.
3. Offer Pain Relief: Administer paracetamol 30 minutes before the procedure or perform a para-cervical block.
4. Prepare the MVA Syringe:
- Assemble the syringe, close the pinch valve, and pull back on the plunger until the plunger arms lock.
- For molar pregnancy, have three syringes ready. For very early pregnancy, insert the cannula without prior cervical dilation.
5. Administer Oxytocin or Ergometrine: Give oxytocin 10 units IM or ergometrine 0.2 mg IM to firm the myometrium and reduce perforation risk.
6. Perform a Bimanual Pelvic Examination: Re-assess the size and position of the uterus and the conditions of the fornices.
7. Insert Sterile Speculum and Visualize the Cervix: Apply antiseptic solution to the vagina and cervix, especially around the os.
8. Check the Cervix for Tears or Protruding POC: Remove any products of conception (POC) with ring (or sponge) forceps.
9. Gently Grasp the Anterior Lip of the Cervix: Use ring forceps or a single-toothed tenaculum. If using a tenaculum, first inject 1 mL of 0.5% lignocaine solution into the cervix.
10. Dilate the Cervix if Needed: For missed abortion or prolonged retention of POC, use mechanical or osmotic dilators, or cervical priming with mifepristone or prostaglandin.
11. Insert the Cannula: While applying gentle traction to the cervix, insert the cannula through the cervix into the uterine cavity just past the internal os.
12. Attach the Prepared MVA Syringe: Hold the ring forceps or tenaculum and the end of the cannula in one hand and the syringe in the other. Release the pinch valve(s) to transfer the vacuum to the uterine cavity.
13. Evacuate Remaining Contents: Gently rotate the syringe from side to side and move the cannula back and forth within the uterine cavity without losing vacuum.
14. Check for Signs of Completion: Look for red or pink foam without tissue, a grating sensation, and the uterus contracting around the cannula.
15. Withdraw the Cannula: Detach the syringe, place the cannula in decontamination solution, and empty the syringe contents into a strainer.
16. Perform a Bimanual Examination: Check the size and firmness of the uterus post-procedure.
17. Inspect the Tissue Removed: Ensure complete evacuation, assess for molar pregnancy, and if necessary, strain and rinse the tissue for examination.
18. Address Absence of POC: If no POC are seen, consider complete abortion, breakthrough bleeding, or possible ectopic pregnancy.
19. Reinsert Speculum and Examine for Bleeding: If persistent bleeding or soft uterus, repeat evacuation.
Post-Procedure Care: Administer paracetamol 500 mg as needed, consider antibiotics, encourage the woman to eat, drink, and walk, and offer other health services.
Discharge Uncomplicated Cases: Discharge within 1-2 hours, advising on symptoms that require immediate attention.
Precautions for Performing MVA:
- Delay the procedure if conditions like shock, severe vaginal bleeding, or intra-abdominal injury are present, and stabilize the patient first.
- Stabilization involves oxygen, IV fluids, antibiotics for sepsis, and blood transfusion if needed.
Shock Management:
- Rapid, weak pulse, low blood pressure, pallor, sweatiness, rapid breathing, anxiousness, confusion, or unconsciousness.
- Treat with oxygen, IV fluids, antibiotics, and blood transfusion if necessary.
Severe Vaginal Bleeding:
- Heavy bright red bleeding, pallor, and blood-soaked materials.
- Assess all bleeding sources, stabilize, and evacuate POC.
Intra-Abdominal Injury:
- Distended abdomen, decreased bowel sounds, rigid abdomen, rebound tenderness, nausea, vomiting, pain, fever, or cramping.
- Immediate management with IV fluids, antibiotics, and potential surgery. Perform MVA after stabilization.


Brief and summarised notes easy to understand the explanations
I love it
Thanks
you have really simplified these notes. it has greatly been revised from the time I came to learn of the nurse’s revision website. an uploud Sir
good and simple work
be blessed 🙏
May the Almighty God bless you abundantly
wow thanks so much
simple and easy to understand