
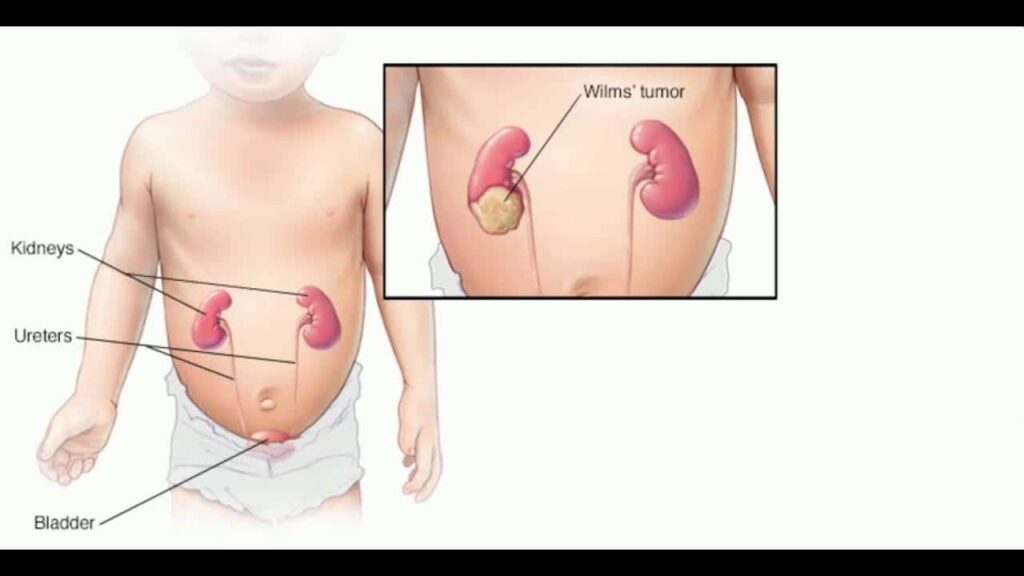
Wilms tumor is a highly malignant embryonic cancer of the kidney that primarily occurs in young children (usually peaking between ages 3 to 4 years). It is the most common primary renal tumor in childhood.
- Laterality: It usually affects only one kidney (unilateral) but can affect both kidneys (bilateral) in 5-10% of cases.
- Embryological Pathophysiology (Expansion): It develops from abnormally persistent, immature embryonic kidney cells called the metanephric blastema. Instead of maturing into normal nephrons (glomeruli and tubules), these blastemal cells multiply out of control, forming a solid, highly vascular tumor.
- Histology (Expansion): The prognosis heavily depends on the microscopic appearance.
- Favorable Histology (FH): Well-differentiated cells (accounts for 90% of cases, highly curable).
- Unfavorable / Anaplastic Histology (UH): Poorly differentiated cells with huge, distorted nuclei (often associated with TP53 gene mutations). Highly resistant to standard chemotherapy.
While most cases are sporadic (random), about 10% are associated with specific genetic mutations, birth defects, and overgrowth syndromes. These usually involve mutations on Chromosome 11 (WT1 and WT2 genes).
- WAGR Syndrome: Caused by a deletion on Chromosome 11p13.
- Wilms tumor (about 30-50% chance of developing it)
- Aniridia (absence of the iris in the eye, causing severe light sensitivity/blindness)
- Genitourinary anomalies (e.g., cryptorchidism, hypospadias)
- Retardation (Intellectual/Mental disability)
- Denys-Drash Syndrome: Caused by a point mutation in the WT1 gene.
- Wilms tumor (very high risk, ~90%)
- Pseudohermaphroditism (male pseudohermaphroditism / ambiguous genitalia)
- Early-onset kidney disease (nephropathy leading to rapid renal failure)
- Beckwith-Wiedemann Syndrome (BWS): An overgrowth syndrome linked to the WT2 gene (Chromosome 11p15).
- Large birth weight (Macrosomia)
- Macroglossia (abnormally large tongue)
- Organomegaly (enlarged internal organs)
- Omphalocele or umbilical hernia
- Increased risk for embryonic tumors (Wilms tumor, hepatoblastoma).
- Hemihypertrophy: An asymmetrical overgrowth condition where one side of the body (or a single limb) is noticeably larger than the other. Strongly associated with Wilms tumor.
Remember: "Wilms has a BAD WAGR"
- Beckwith-Wiedemann Syndrome (Overgrowth, macroglossia)
- Aniridia (Part of WAGR)
- Denys-Drash Syndrome (Kidney disease, ambiguous genitalia)
- WAGR (Wilms, Aniridia, GU anomalies, Retardation)
- Painless abdominal mass: Usually discovered incidentally by a parent while bathing the child or by a pediatrician during a routine exam. Crucial distinguishing factor: The mass is smooth, firm, and does NOT cross the midline (unlike Neuroblastoma, which is nodular and frequently crosses the midline). It moves downwards with respiration.
- Abdominal pain: Present in about 30-40% of cases (often occurs if the tumor undergoes rapid growth causing capsular stretching, or bleeding within the tumor).
- Blood in urine (Hematuria): Present in 15-25% of cases. Microscopic or macroscopic, resulting from tumor invasion into the renal collecting system.
- Hypertension (HTN): Physiological Expansion: Occurs in up to 25% of patients. Why? The growing tumor compresses the normal renal artery, leading to renal ischemia. The kidney responds by inappropriately secreting massive amounts of Renin, activating the RAAS pathway (Renin-Angiotensin-Aldosterone System), causing severe vasoconstriction and fluid retention. Rule: Check BP in ALL children with an abdominal mass!
- Fever: Low-grade, unexplained (due to tumor necrosis or cytokine release).
- Weight loss & Anorexia: Cachexia due to the high metabolic demand of the malignancy.
- Anemia: Due to chronic disease, hematuria, or tumor hemorrhage.
- Varicocele: Enlarged, dilated veins in the scrotum. Anatomical Expansion: Usually occurs on the LEFT side. Why? The left testicular/gonadal vein drains at a 90-degree angle directly into the Left Renal Vein. If a Wilms tumor extends a "tumor thrombus" into the left renal vein, it blocks gonadal drainage, causing backup and a varicocele.
- Respiratory distress: Occurs if the massive tumor pushes up against the diaphragm, restricting lung expansion.
- Cough & Hemoptysis: Suggests advanced disease with lung metastases (the lungs are the #1 site for Wilms tumor metastasis via hematogenous spread).
⚠️ ABSOLUTE NURSING PRIORITY: DO NOT PALPATE THE ABDOMEN!
Once a Wilms tumor is suspected, place a large warning sign over the child's bed reading: "DO NOT PALPATE ABDOMEN." The tumor is highly friable and encapsulated by a thin, fragile membrane. Hard or repeated palpation can cause the capsule to rupture, spilling millions of cancer cells into the peritoneal cavity, instantly upgrading the cancer to Stage III and drastically worsening the prognosis.
- Inspect the abdomen (avoid deep palpation).
- Measure blood pressure in both arms (to check for renin-induced HTN).
- Examine genitals for anomalies (hypospadias/cryptorchidism for WAGR/Denys-Drash).
- Check for aniridia (look closely at the iris with a penlight).
- Assess for hemihypertrophy.
- Listen to lungs (checking for effusions or metastatic masses).
- FBC (Full Blood Count): Anemia is common.
- Urinalysis: Checks for microscopic blood and protein.
- Kidney Function Tests (BUN, Creatinine): Usually normal unless bilateral, but baseline is needed before nephrectomy.
- Liver function tests & Coagulation studies: Essential baseline before major surgery.
Note on Tumor Markers: Unlike Neuroblastoma (which has elevated VMA/HVA in urine), Wilms tumor has no specific diagnostic tumor markers in the blood or urine.
- Ultrasound: The first-line, non-invasive test. Differentiates a solid tumor from a fluid-filled cyst. Checks both kidneys and evaluates if the tumor is invading the renal vein or inferior vena cava (IVC).
- CT scan (Abdomen/Pelvis): Provides exact anatomical detail, size, lymph node involvement, and checks the opposite kidney and liver for metastasis.
- MRI: Superior for visualizing IVC tumor thrombus extension (which can reach all the way into the right atrium of the heart!).
- Chest X-ray / Chest CT: Absolutely essential to rule out lung metastases (the most common site of distant spread).
- Generally CONTRAINDICATED before surgery in unilateral Wilms tumor. You do not want to risk seeding the needle tract or spilling the tumor. The diagnosis is confirmed pathologically after the entire kidney is removed en bloc.
- Exceptions: A biopsy is only done if the tumor looks highly atypical, if both kidneys are involved (bilateral), or if the tumor is deemed inoperable and needs chemotherapy to shrink it first.
Staging defines the extent of spread and directly dictates the intensity of chemotherapy and radiation required.
| Stage | Description |
|---|---|
| Stage I | Tumor is completely confined to the kidney and was completely completely removed with the capsule fully intact (no spillage). |
| Stage II | Tumor extends beyond the kidney (into renal fat or blood vessels) but was still completely removed with no residual cancer left behind. |
| Stage III | Non-hematogenous residual tumor left in the abdomen. This includes positive lymph nodes, incomplete resection, or tumor spillage/rupture before or during surgery. (Requires abdominal radiation). |
| Stage IV | Hematogenous distant metastases (spread via blood to the lungs, liver, bone, or brain). |
| Stage V | Bilateral kidney involvement at the time of initial diagnosis. |
IMPORTANT PRINCIPLE: The gold standard treatment involves a combination of Surgery, Chemotherapy, and sometimes Radiation. The exact sequence depends on the protocol (COG in America prefers upfront surgery; SIOP in Europe prefers upfront chemotherapy to shrink it first).
Goal: Remove the entire affected kidney, tumor, surrounding fat, and adrenal gland en bloc (all in one piece) without rupturing the capsule.
- Signage: DO NOT palpate abdomen!
- Blood pressure control: Give antihypertensives (e.g., Nifedipine, Captopril/Enalapril) if renin-induced HTN is present to prevent intra-op stroke.
- Treat anemia: Transfuse packed RBCs if severely anemic to optimize oxygen delivery for surgery.
- NPO & IV Access: 6-8 hours fasting. Ensure large-bore IV access and cross-match blood (tumors are highly vascular; high risk of massive hemorrhage).
- Bowel preparation: Sometimes needed if the massive tumor is compressing the colon.
- Psychological preparation: Explain to the child (using age-appropriate terms) that the "lump in their belly" will be removed. Comfort parents who are often shocked by the sudden diagnosis.
- Fluid Balance (CRITICAL): The child now only has ONE kidney. Strict Intake/Output monitoring is mandatory.
- Urine Output: Monitor hourly. Must be >1 mL/kg/hour. Danger Sign: If urine output drops, notify the doctor immediately. It could indicate failure of the solitary remaining kidney, severe dehydration, or surgical obstruction of the remaining ureter.
- Electrolytes: Monitor for hyperkalemia (high potassium) due to acute kidney injury or tumor lysis.
- Blood pressure: Monitor regularly. The remaining kidney can still secrete excess renin in response to fluid shifts, or the child may be hypotensive from surgical bleeding.
- Positioning & Activity: Semi-Fowler's (head elevated 30-45 degrees) to drop the abdominal organs away from the diaphragm, improving respiratory excursion. Early, gentle mobilization to prevent DVT/pneumonia, but avoid straining.
- Pain Management: Epidural or PCA (patient-controlled analgesia) with IV morphine. Crucial Contraindication: AVOID NSAIDs (like Ibuprofen/Diclofenac) because they decrease renal blood flow and can damage the single remaining kidney!
- Wound Care: Monitor the large flank/transabdominal incision for bleeding, hematoma, or infection. Monitor surgical drains.
- Bowel Function: Risk of paralytic ileus. Maintain NPO with IV fluids until bowel sounds return and flatus is passed, then progress from clear liquids to a regular diet.
Case: A child's preoperative MRI shows the Wilms tumor has grown a "tail" (tumor thrombus) straight up the renal vein and into the Inferior Vena Cava (IVC), almost reaching the heart. What specific post-operative complication must you monitor for?
Answer: Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE). Removing an IVC tumor often requires complex vascular reconstruction or bypass. The nurse must strictly monitor lower limb circulation, swelling, and administer prescribed anticoagulants (Heparin/LMWH) to prevent fatal clots.
Used for almost all stages (except some very early Stage I favorable tumors). Chemotherapy shrinks metastases and kills micrometastatic disease.
- Vincristine: A mitotic inhibitor. Side effects: Peripheral neuropathy (foot drop, loss of reflexes), severe constipation, and paralytic ileus. (Monitor bowel movements strictly!).
- Dactinomycin (Actinomycin D): An antitumor antibiotic. Side effects: It is a severe vesicant (causes massive tissue necrosis if the IV line leaks). Ensure perfect IV patency; never give IM/SubQ. Can also cause liver toxicity (Veno-occlusive disease).
- Doxorubicin (Adriamycin): Added for Stage III/IV. Side effects: Cardiotoxicity. Can cause irreversible heart failure years later. A baseline Echocardiogram is mandatory before starting.
- Cyclophosphamide & Etoposide: Added for high-risk or anaplastic (unfavorable) histology. Side effects: Hemorrhagic cystitis (requires aggressive hydration).
- Radiation Recall: If a child receives Dactinomycin or Doxorubicin and later receives abdominal radiation, the skin that was previously irradiated may suddenly become bright red, blistered, and inflamed (Radiation Recall Dermatitis).
- Indications: Used for Stage III (if the tumor ruptured/spilled), Stage IV (to treat lung/brain mets), or any stage with Unfavorable Histology. Usually applied to the whole abdomen or flank.
- Nursing Care: Gentle skin care (no harsh soaps/lotions). Aggressive nausea/vomiting management. Monitor for radiation enteritis (severe diarrhea, cramping) and bowel obstruction due to radiation-induced inflammation and strictures.
- Goal: Preserve as much functional kidney tissue as absolutely possible to prevent the child from becoming dependent on lifelong dialysis.
- Management: Standard protocol is flipped. A biopsy is done first to confirm histology. Then, neoadjuvant (pre-surgery) chemotherapy is given for several weeks to shrink both tumors. Finally, Nephron-sparing surgery (Partial Nephrectomy) is performed to cut out the tumors while leaving healthy kidney tissue behind.
- Nursing Care: Exquisitely careful fluid and electrolyte management post-op. Long-term monitoring of GFR and renal function. Dialysis may be required if insufficient tissue survives.
- Tumor Rupture / Spillage:
- Can happen from trauma (seatbelt injury), rough handling, or intra-operatively.
- Consequence: Instantly increases the stage to Stage III, requiring highly toxic whole-abdominal radiation.
- Nursing: If sudden rupture is suspected pre-op (sudden massive increase in abdominal pain, rapidly dropping BP/shock), prepare for emergency surgery and monitor for chemical peritonitis.
- Post-operative Bleeding:
- The tumor bed and renal vessels are massive. A slipped surgical ligature can cause fatal internal bleeding.
- Signs: Tachycardia, hypotension, pallor, rapidly distending abdomen, sudden massive increase in bloody drain output.
- Management: Immediate fluid resuscitation, blood transfusion, and rush back to the OR for re-exploration.
- Acute Kidney Injury (AKI):
- From the remaining kidney being overwhelmed, severe hypovolemia (dehydration), or administration of nephrotoxic drugs (e.g., Gentamicin, NSAIDs). Dialysis may be temporarily needed.
- Long-Term Survivorship Complications:
- Renal Failure: Chronic kidney disease years later due to hyperfiltration injury of the single remaining kidney.
- Heart Failure: Dilated cardiomyopathy from Doxorubicin toxicity.
- Secondary Primary Malignancies: Developing leukemia or bone cancer decades later as a direct result of DNA damage from the childhood chemotherapy and radiation.
- Musculoskeletal problems: Flank radiation stunts bone and muscle growth on that side, leading to severe scoliosis (curvature of the spine) and underdeveloped abdominal muscles.
Wilms tumor represents one of the great success stories of modern pediatric oncology. Due to highly coordinated, multi-disciplinary protocol treatments (surgery + chemo + radiation), survival rates are excellent.
- Overall Cure Rate: ~90%
- Stage I-II (Favorable Histology): >95% survival.
- Stage III: 85-90% survival.
- Stage IV (Metastatic): 70-80% survival (requires highly intensive, toxic treatment).
- Unfavorable Histology (Anaplastic): Prognosis drops significantly to 50-70% due to chemo-resistance.
- Bilateral (Stage V): 70-80% with a careful kidney-sparing approach.
Quick Quiz
Wilms Tumor Quiz
Paediatrics - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Wilms Tumor Quiz
Paediatrics
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.