
A brain tumor is an abnormal growth of cells inside the skull. Because the skull is a hard box that cannot expand, any growth inside creates pressure and damages the brain.
To truly understand brain tumors, you must understand the Monro-Kellie Hypothesis. The skull is a rigid, closed vault containing exactly three things: Brain tissue (80%), Blood (10%), and Cerebrospinal Fluid/CSF (10%).
Because the skull cannot expand, if a 4th component (a tumor) starts growing, one of the other three must be pushed out to make room. First, CSF is pushed down the spine. Then, blood flow is restricted (causing brain ischemia). Finally, the brain tissue itself is pushed out through the bottom of the skull (Herniation), which is fatal.
- Medulloblastoma:
- Most common malignant brain tumor in children.
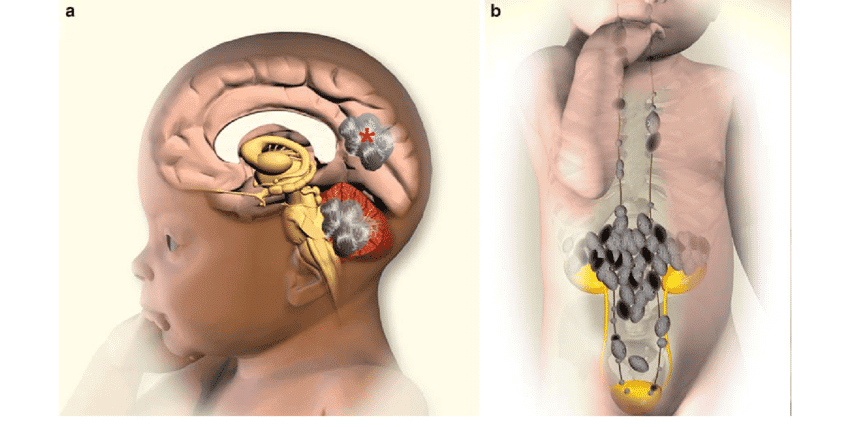
- Starts in the cerebellum (the back of the brain, which controls balance and coordination).
- Can spread through the spinal fluid (often called "drop metastases" because gravity pulls the cancer cells down the spinal cord).
- More common in boys.
- Low-Grade Glioma (Astrocytoma):
- Slow-growing, often benign.
- Pathophysiology: Arises from astrocytes, the star-shaped glial cells that normally form the Blood-Brain Barrier.
- Can be located in the cerebellum or the optic nerve (affecting vision).
- Pilocytic astrocytoma is the most common type.
- Ependymoma:
- Starts in the ventricles (the fluid spaces in the brain).
- Pathophysiology: Arises from ependymal cells, the ciliated cells that line the ventricles and help produce/circulate CSF.
- Can physically block cerebrospinal fluid (CSF) flow, causing a backup of fluid known as hydrocephalus.
- Brainstem Glioma:
- Located in the brainstem (the medulla, pons, and midbrain).
- Physiological Danger: The brainstem is the control center for vital, involuntary functions like breathing, heart rate, and blood pressure.
- Difficult (or impossible) to operate on without killing the patient.
- Often has a very poor prognosis.
- Craniopharyngioma:
- Located near the pituitary gland (the hormone control center of the body).
- Affects growth (Growth Hormone disruption), vision (it presses on the optic chiasm causing bitemporal hemianopsia/tunnel vision), and water balance.
- Water Balance: Can cause Diabetes Insipidus due to a lack of Anti-Diuretic Hormone (ADH), leading to massive, dilute urination.
Symptoms heavily depend on the tumor's location, its size, and the child's age.
- Headache: Worse in the morning, wakes the child from sleep, and gets worse with coughing or straining (Valsalva maneuver increases pressure).
- Vomiting: Especially in the morning, projectile (shoots out forcefully), and notably occurs without nausea.
Physiology tip: Why worse in the morning? When sleeping flat, gravity doesn't help drain venous blood from the head. Also, breathing slows during sleep, retaining CO2. CO2 is a potent vasodilator, which increases blood volume in the brain, spiking the ICP first thing in the morning!
- Bulging fontanelle: Seen in infants because the "soft spot" on the head bulges out (their skull bones are not yet fused).
- Sunset eyes: In infants – the eyes look downward, and the white of the eye (sclera) shows above the iris. (Parinaud syndrome from dorsal midbrain compression).
- Increased head circumference: In infants and young children, the head literally grows faster than normal because the unfused skull sutures stretch apart.
- Irritability: Infant cries constantly, pitched in a high tone, and cannot be comforted.
- Lethargy: Child sleeps excessively, hard to wake.
- Ataxia: Unsteady walking, falling to one side, wide-based gait (feet far apart to maintain balance).
- Tremor: Shaking hands specifically when reaching for objects (Intention tremor).
- Dysmetria: Misses target when reaching (overshoots or undershoots).
- Nystagmus: Eyes move back and forth involuntarily.
- Seizures: New-onset seizures in a previously healthy child are highly suspicious of a brain mass.
- Vision changes: Squinting, double vision (diplopia), loss of peripheral vision, child bumps into things.
- Behavior changes: Personality changes, school performance drops, memory problems (especially if in frontal/temporal lobes).
- Weakness: One side of the body weaker than the other (hemiparesis) due to motor cortex compression.
- Cranial nerve palsies: Facial droop, difficulty swallowing, hoarse voice, tongue deviation.
- Endocrine problems: Growth failure, diabetes insipidus (excessive thirst and urination), delayed or early puberty.
- Neurological Examination:
- Check cranial nerves (pupil response, eye movements, facial sensation, hearing, gag reflex, tongue movement, shoulder shrug).
- Check strength and sensation in all limbs.
- Check balance and coordination (heel-to-toe walking, finger-to-nose test).
- Check fundoscopy (looking at the back of the eye with an ophthalmoscope) for papilledema (swelling of the optic disc from severe intracranial pressure pushing down the optic nerve).
- Imaging:
- CT Scan: Quick, available in many Ugandan hospitals. Shows tumor location, size, bleeding, and hydrocephalus. Downside: Uses radiation.
- MRI: Better detail, no radiation. Shows exact tumor type and relation to important brain structures. May require sedation or general anesthesia in young children (because they must stay perfectly still).
- Nursing care for MRI: Remove all metal objects (hair clips, jewelry, coins), check for implants, explain loud noises to the child, give sedation as ordered, monitor vitals during scan if anesthesia used, ensure child is NPO (nothing by mouth) if sedated.
- Lumbar Puncture (LP):
- Checks for tumor cells in spinal fluid.
-
CRITICAL WARNING: Only done AFTER imaging confirms no risk of brain herniation! If intracranial pressure is very high, doing an LP creates a low-pressure vacuum below the brain. The brain will instantly be sucked down through the foramen magnum (coning/herniation), which is instantly fatal.
- Biopsy or Surgery:
- Tissue sample needed for exact, definitive diagnosis (grading and typing). May be done as part of the surgery to remove the tumor.
Goal: Remove as much tumor as safely possible without damaging healthy brain tissue (Maximal safe resection).
- Psychological preparation: Explain to the child (use dolls, pictures), reassure parents, allow parents to stay until anesthesia takes effect.
- Shave head: Only shave the minimal area needed (do not shave entire head unless necessary). Use clippers, not razors (razors create micro-abrasions that drastically increase infection risk).
- Steroids: Usually Dexamethasone to reduce brain swelling around the tumor. Nursing Monitor: Watch for high blood sugar (steroid-induced diabetes), mood changes, increased appetite, and GI bleeding.
- Anticonvulsants: Given prophylactically if the child has seizures or if the tumor is near a seizure-prone area (like the cortex).
- Baseline assessment: Document exact neurological status (strength, speech, vision) BEFORE surgery for comparison after surgery. (If they wake up weak, you need to know if it's new!).
- NPO: Nothing by mouth for 6-8 hours before surgery to prevent aspiration under anesthesia.
- IV access: Ensure good IV line, type and cross-match blood for possible transfusion.
- Positioning: Head of bed elevated 30-45 degrees to reduce brain pressure. Keep head in a neutral midline position (not twisted). Avoid neck flexion, which blocks the jugular veins and prevents blood from draining out of the brain!
- Neurological checks: Every 15 minutes for the first hour, every 30 minutes for 2 hours, then every hour for 24 hours, then every 4 hours. Check:
- Level of consciousness (AVPU: Alert, Voice, Pain, Unresponsive; or GCS: Glasgow Coma Scale).
- Pupil size and reaction to light (use penlight).
- Movement of all four limbs.
- Vital signs (blood pressure, pulse, respiration, temperature).
Cushing's Triad is a late, critical sign of severe brain pressure (impending herniation). It consists of:
- High blood pressure (Widening pulse pressure)
- Slow pulse (Bradycardia)
- Irregular breathing (Cheyne-Stokes respirations)
- Fluid management: Strict input/output charting. Often fluid restriction is ordered (e.g., 2/3 maintenance) to prevent brain swelling. Use a pediatric infusion pump. Avoid hypotonic fluids (like plain dextrose water) because they cause water to rush into cells, which will drastically worsen brain swelling.
- Pain management: Codeine, paracetamol, morphine if severe. Avoid NSAIDs (aspirin, ibuprofen) due to the risk of intracranial bleeding.
- Seizure precautions: Keep suction and oxygen ready, padded side rails. Do not restrain during a seizure, turn head to side, time the seizure, and give diazepam or lorazepam if it lasts >5 minutes.
- Wound care: Keep dressing clean and dry. Check for a CSF leak (clear fluid dripping from the wound, nose, or ear). Check for the "halo sign" on gauze (blood in the center, surrounded by a yellowish ring of CSF). Check for bleeding, swelling, redness.
- Temperature control: Avoid fever! Fever increases brain metabolism and swelling. Use paracetamol and cooling measures. Watch closely for infection.
- Nutrition: Start with clear liquids when awake, progress to a regular diet as tolerated. Some children have swallowing problems (dysphagia) after posterior fossa surgery – do a swallowing assessment first.
- Communication: Child may have temporary or permanent speech problems. Use picture boards, gestures, patience.
- Posterior fossa syndrome: After cerebellum surgery, the child may be mute, emotionally labile, have swallowing problems, and weakness. Usually temporary but can last weeks. Requires intensive rehabilitation.
- Hydrocephalus: If CSF flow is blocked, they may need a temporary external ventricular drain (EVD) or a permanent shunt.
- EVD nursing care: Keep the drainage system at the correct prescribed level (usually 15cm above the ear). Do not let it drop below level (too much drainage causes the brain ventricles to collapse and tear blood vessels, causing bleeding). Do not raise it above level (drainage stops, pressure builds). Keep system closed (do not disconnect). Monitor CSF color (should be clear/straw-colored; blood or pus is abnormal). Monitor amount hourly. Never clamp without a doctor's order!
- Aseptic meningitis: Fever, headache, stiff neck after surgery (not caused by bacteria, but by chemical irritation from blood/tissue in the CSF). Usually responds to steroids.
- Cranial nerve damage: Facial weakness, hearing loss, swallowing problems. May need a feeding tube, or eye protection/taping if they cannot blink.
Used for tumors that cannot be completely removed or that tend to spread.
- Medulloblastoma: Chemotherapy is essential (vincristine, cisplatin, lomustine, cyclophosphamide).
- Ependymoma: May need chemotherapy if there is residual or recurrent tumor.
- Glioma: Less responsive to chemotherapy; surgery and radiation are the main treatments.
- Special considerations for brain tumor chemotherapy:
- Many systemic drugs cannot cross the blood-brain barrier.
- Intrathecal chemotherapy (injected directly into the spinal fluid) may be used to bypass the barrier.
- High-dose methotrexate requires highly specialized monitoring (hydration, leucovorin rescue).
Used for medulloblastoma, ependymoma, and some gliomas.
- Craniospinal irradiation is used for medulloblastoma (radiating the whole brain and the entire spine because it drops metastases).
- Nursing care:
- Skin care (gentle washing, no perfumes, use loose hats).
- Fatigue management.
- Monitor for somnolence syndrome (excessive, profound sleepiness occurring 4-6 weeks after radiation ends).
- Monitor for endocrine problems (growth hormone deficiency, thyroid problems due to radiation scatter).
- Cognitive decline: Especially profound in young developing brains. Medical teams try to avoid radiation in children under age 3 if at all possible.
- Ventriculoperitoneal (VP) shunt: A surgically implanted tube that runs from the brain ventricle, under the skin, down to the abdomen (peritoneum) to drain excess CSF.
- Nursing care: Monitor for shunt malfunction (headache, vomiting, lethargy, irritability, sunsetting eyes, increased head size).
- Monitor for infection (fever, redness tracking along the shunt tract under the skin, abdominal pain, peritonitis).
- If an infection occurs, it usually requires surgical removal of the shunt, placement of an external drain, and heavy IV antibiotics.
- Pilocytic astrocytoma: >90% cure rate with surgery alone.
- Medulloblastoma: 70-80% cure rate with surgery + radiation + chemotherapy (Prognosis is worse if it has metastasized or if there is residual tumor).
- Ependymoma: 50-70% survival depending on location and if it was completely removed.
- Brainstem glioma: Very poor, especially diffuse intrinsic pontine glioma (DIPG) – generally has a 9-12 months median survival.
🧠 Mnemonic: Brain Tumor Post-Op Nursing Priorities
Remember "H.E.A.D." to monitor the post-op brain tumor patient:
- Head elevated 30-45° (Promotes venous drainage)
- Evaluate Neuro status often (GCS, Pupils, Cushing's triad)
- Assess for CSF leaks (Check dressings for Halo sign)
- Decrease metabolic demands (Strict fever control, pain meds, avoid seizures)
Cancer that develops from immature nerve cells (neuroblasts). It usually starts in the adrenal glands (the small glands on top of the kidneys that make stress hormones) or along the sympathetic nerve chain in the spine/abdomen/chest. It is most common in infants and children under 5 years.
It develops from fetal neural crest tissue that fails to mature properly. The MYCN oncogene amplification makes it highly aggressive.
- Abdominal mass: Firm, irregular mass that crosses the midline of the abdomen. (High-Yield Differential: Wilms tumor is usually smooth and stays on one side).
- Abdominal pain, distension, constipation.
- Hypertension: High blood pressure caused by kidney artery compression OR the tumor directly secreting catecholamines (adrenaline).
- Respiratory distress if a chest tumor compresses the lungs.
- Bone pain: Child refuses to walk, cries when moved.
- Periorbital ecchymosis ("Raccoon eyes"): Bruising around both eyes caused by tumor metastasis into the orbital bones.
- Proptosis: Bulging eyes.
- Bone marrow failure: Anemia, bruising, infection (clinically looks like leukemia).
- Skin nodules: Blue/purple skin nodules in infants ("blueberry muffin baby").
- Hepatomegaly: Massive liver enlargement in infants (Stage 4S).
- Opsoclonus-myoclonus syndrome: "Dancing eyes, dancing feet." Rapid, irregular eye movements and jerking muscles. (Associated with a better tumor prognosis, but the neurological damage can be permanent).
- Secretory diarrhea: The tumor secretes Vasoactive Intestinal Peptide (VIP), causing severe watery diarrhea and dehydration.
- Sweating and Palpitations: From catecholamine release.
Case: A 3-year-old child presents with a large abdominal mass. How can the nurse differentiate between Wilms Tumor (Nephroblastoma) and Neuroblastoma during physical assessment?
Answer: During palpation, a Wilms tumor typically feels smooth and is confined to one side of the abdomen (does not cross the midline). A Neuroblastoma usually feels nodular/irregular and heavily crosses the midline. Additionally, if the child has "raccoon eyes" or severe hypertension, it points strongly to Neuroblastoma.
- Laboratory Tests:
- Urinary catecholamines (VMA and HVA): Elevated in 90% of cases. This is the key diagnostic marker! (Because the tumor grows from adrenal medullary cells, it spits out adrenaline breakdown products into the urine).
- FBC, LDH, Ferritin, Neuron-specific enolase (NSE).
- Imaging: Ultrasound, CT/MRI, Bone scan. MIBG scan: A special nuclear medicine scan using radioactive iodine that targets neuroblastoma cells. It lights up all primary and metastatic sites.
- Biopsy: Bilateral bone marrow aspiration (both hips), tumor biopsy, and MYCN amplification testing (crucial for prognosis).
- Staging (INSS):
- Stage 1: Localized, completely removed.
- Stage 2: Localized with residual or lymph node involvement.
- Stage 3: Large tumor crossing midline.
- Stage 4: Spread to distant lymph nodes, bone, marrow, liver, skin.
- Stage 4S: Special "magic" stage for infants (<1 year) with spread limited to liver, skin, and/or minimal bone marrow. It frequently spontaneously regresses and cures itself!
- LOW RISK: (Stage 1, some Stage 2, Stage 4S). Surgery alone, or observation only (for 4S spontaneous regression).
- INTERMEDIATE RISK: (Stage 3, some Stage 4 in infants). Surgery + Moderate chemotherapy (Carboplatin, cyclophosphamide, doxorubicin, etoposide) for 4-8 cycles.
- HIGH RISK (Very Intensive): (Stage 4 in children >18 months, or MYCN amplified).
- Induction chemo: Cisplatin, etoposide, doxorubicin, cyclophosphamide, vincristine. (Intense immunocompromise monitoring).
- Surgery & Radiation: To remove shrunk tumors and radiate metastatic sites.
- Autologous Stem Cell Transplant: Collect the child's own stem cells, blast the body with lethal high-dose chemo (busulfan, melphalan) to kill hidden cancer cells, then rescue the patient by giving their stem cells back. (Nursing: Strict isolation, intense mucositis).
- Differentiation therapy: 13-cis-retinoic acid (isotretinoin/Accutane) for 6 months post-transplant. It chemically forces any remaining primitive neuroblastoma cells to mature into harmless normal nerve cells! (Nursing: Causes severe dry skin/lips. Highly teratogenic. Avoid Vit A).
- Immunotherapy: Anti-GD2 antibody (dinutuximab). Targets GD2, a protein on neuroblastoma cells. Side effects: GD2 is also on pain nerves, causing horrific severe pain requiring continuous IV morphine. Also causes Capillary Leak Syndrome (massive swelling, hypotension). Pre-medicate heavily!
Prognosis: Low risk (>95%), Intermediate (80-90%), High risk (40-50% despite brutal treatment). Stage 4S is excellent. MYCN amplification always means a worse prognosis.
Quick Quiz
Brain & Neuroblastoma Quiz
Paediatrics - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
Brain & Neuroblastoma Quiz
Paediatrics
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.